Download presentation
Presentation is loading. Please wait.

1
Understanding Cardiac Imaging
Aashish D. Dadarwala, D.O. Director of Medical Education Long Beach Medical Center

2
Thoracic Landmarks

3
Radiographic Landmarks - Male

4
Radiographic Landmarks - Female

5
Superimposed gross and radiographic anatomy

6
Benefits of a PA / Lateral Chest Radiograph in Cardiac Evaluation vs
Benefits of a PA / Lateral Chest Radiograph in Cardiac Evaluation vs. Portable Radiography Unfortunately, in portable radiography the following will lead to false diagnosis of cardiac pathology: Heart physically closer to film Balanced gravitational force on upper and lower vasculature Magnification secondary to proximity of x-ray tube Poor inspiratory effort

7
International Medicine

8
Thoracic Landmarks – lateral view

9
52 year old male comes to your office for a routine physical
52 year old male comes to your office for a routine physical. You perform a CXR. Did you help or hurt this patient? Diagnosis? Hypertension: The prominence of an ectatic aorta is seen with a bulge noted along the superior right heart border. With increased systemic resistance over a long duration, the unwinding of the ascending aorta becomes increasing prominent and the left ventricular wall begins to hypertrophy (not to be confused with dilatation). The descending aorta in this film is normal in size.
. The descending aorta in this film is normal in size.")
10
Same patient comes to your office 3 years later after bartending in Peru? (and forgot his meds in Smithtown) Congestive Heart Failure: Kerley A Lines – These lines are long, straight and typically seen between the hilum and pleura depending on the accumulation of abnormal amounts of edema within the perilymphatic connective tissue. These are reversible with edema, but irreversible with pneumoconiosis or lymphangitic carcinoma Kerley B Lines – These lines are short, straight lines in the peripheral lung field also caused by an increase in interstitial fluid, primarily within the perilymphatic interstitial tissue. Kerley C Lines – These are a lacy network of lines seen in interstitial pulmonary edema and caused by the superimposition of many Kerley B lines.

11
Closer Look – Kerley A and B lines

12
53 year old with MI 2 years ago c/o increasing shortness of breath
53 year old with MI 2 years ago c/o increasing shortness of breath. Diagnosis? Notice the increasing amount of fluid obscuring the right hemidiaphragm and now fluid is seen within the right middle fissure. Heart size is relatively preserved. How can you distinguish this from a consolidated process?

13
Right Sided, Lateral Decubitus Film

14
Using what we learn each day….

15
As an intern, the vascular surgeon calls you at 2 am to check the pacer tip. Your response?
Even though the pacer tip is located overlying the right ventricle, if there is a problem with improper firing, it’s important to check if the pacer is anterior or posterior. A lateral film must be ordered and the proper continuity of the pacer wires should be assessed.

16
Where is the tip of the patient’s right ventricular pacer?
Notice the distal tip of the pacer wires is located in the posterior aspect of the heart. The right ventricle is adjacent to the sternum. While the wires do appear to be entering the right atrium, the most likely explanation is the inadvertent placement into the coronary sinus.

17
A 24 year old medical student has a history of asthma and reports to the clinic for shortness of breath. What is your diagnosis? With the absence of lung markings on the right, the cardiac silhouette is shifted to the left and the apparent opacity on the right cardiac border is the entire lung collapsed onto itself (i.e. no aeration of bronchioles). The findings are suggestive of a right-sided pneumothorax. Only minimal shifting of the mediastinum is noted. Always check the penetration of the film before making a diagnosis.
. The findings are suggestive of a right-sided pneumothorax. Only minimal shifting of the mediastinum is noted. Always check the penetration of the film before making a diagnosis.")
18
61 year old hispanic male with a widened pulse pressure and history of endocarditis. Diagnosis?

19
Aortic Regurgitation In patients with aortic regurgitation, CXR findings of a dilated ascending aorta and enlarged left ventricle are together suggestive. Moreover, note the descending aorta and aortic knob are not dilated. There is no evidence of failure in this patient. Several causes of an enlarged ascending aorta include Marfan’s disease, aortic insufficiency, post-stenotic dilation and aortic aneurysms.

20
Sudden chest pain and shortness of breath in a construction worker admitted for esophageal cancer. Diagnosis? A LUL atelectasis is described as a veil covering the left lung field and obscuring the entire cardiac silhouette. Note the elevated left hemidiaphragm and tracheal deviation. Also, there are no distinct air bronchograms. A lateral film would be helpful in this case.

21
Left Upper Lobe Atelectasis
Atelectasis is the loss of lung volume and the direct sign is displacement of the fissures. Note in this case, the lower lung field appear remarkably clear. And so even though this is not evident on the PA image, the lateral shows clear opacification overlying the the anterior mediastinum. Together, these findings are consistent with a LUL atelectasis.

22
25 year old pt with increasing shortness of breath, no fever or cough
25 year old pt with increasing shortness of breath, no fever or cough. Diagnosis? Although not the best image, the increased density of the left heart silhouette should indicate a retrocardiac opacity/mass or left lower lobe atelectasis. If you note carefully, the right heart border is abnormally overlying the vertebral bodies suggesting that the increased density is caused by an atelectatic lower left lung as opposed to a space occupying mass/infiltrate. A subtle triangular shadow along the left lateral border may also suggest some linear atelectasis.

23
39 yo female has increasing dyspnea with exertion and a good history elicits that as a child, she had a fever and rash, untreated. Diagnosis?

24
Mitral Stenosis Mitral stenosis creates a characteristic configuration dominated by an enlarged left atrium. As a result, the left main stem brochus is shifted up and appears more horizontal. Moreso, just below the aortic knob on the patient’s left, there is a convex bulge which represents the left atrial appendage. Finally, look for enlarged pulmonary veins and cephalization.

26
24 year old male playing sports on a cold thanksgiving day now with decreased breath sounds RUL field. Diagnosis? A right upper lobe atelectasis produces a wedge like density adjacent to the right side of the upper spine and mediastinum. The trachea is shifted and the lung markings are stretched upward to fill in the remaining space. Notice how the vasculature is spread out compared to the left hemithorax. Since bronchi serve individual lobes there are specific appearances that accompany individual lobar atelectasis.

27
Same patient now with fever and increasing cough. Diagnosis?
Here there is resolution of the RUL infiltrate but we’ve lost the right heart border as well as the left heart border. The remained of the heart and mediatstinum appear normal. The loss of the right border is due to a confluence of shadows from a consolidation and soft tissue (i.e. right heart border). The findings suggest more of an infiltrative process than an atelectatic process.
. The findings suggest more of an infiltrative process than an atelectatic process.")
28
Same patient, continues to play football on Christmas day. Diagnosis?
Pneumothorax: The pressure in the pleural space is normally 5 cm of water below atmospheric. If air is introduced into the pleura space and the visceral and parietal layers of the pleura are allowed to separate, the lungs will begin to collapse and the thoracic cage will enlarge. The complete translucency on the left with absence of vascular markings is characteristic. The small central density on the left is the collapsed lung.

29
35 year old female with 2 day hx of sharp chest pain mostly in the back and left arm. Diagnosis?

30
EKG findings: Vital Signs: 140/80, pulse 102, resp. rate 18, T = 37 Celsius. Physical Exam and Blood Pressure clues… Do I admit this patient?? Causes??

31
Echocardiogram: A fluid collection greater than 20 mm in diameter (echo-free area) is consider a large pericardial effusion. However, the determination to remove the fluid is based on the signs or symptoms of tamponade including JVD, pulses paradoxes and decreased peripheral pulses. A drop >10 mm for systolic pressure with inspiration suggests pulses paradoxes. This phenomenon is due to increased pressure from the tamponade causing decreased filling of the right atrium and ventricle with subsequent drop in pulmonary and left ventricular pressures and filling.
 is consider a large pericardial effusion. However, the determination to remove the fluid is based on the signs or symptoms of tamponade including JVD, pulses paradoxes and decreased peripheral pulses. A drop >10 mm for systolic pressure with inspiration suggests pulses paradoxes. This phenomenon is due to increased pressure from the tamponade causing decreased filling of the right atrium and ventricle with subsequent drop in pulmonary and left ventricular pressures and filling.")
32
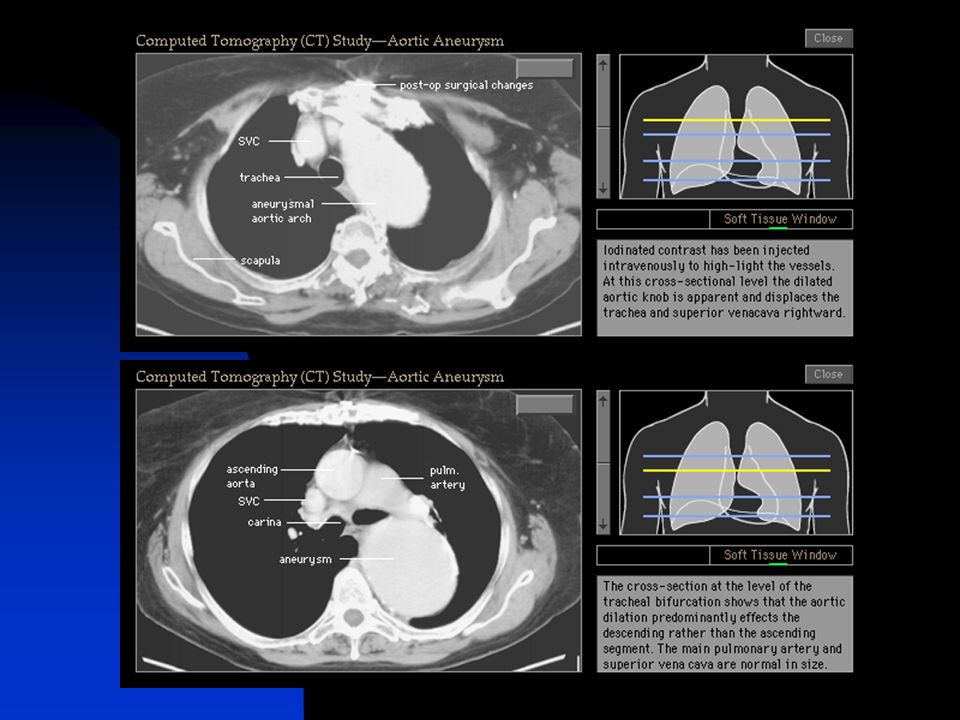
CAT Scan Chest:

34
65 year old male with chest pain and mottled lower extremities
65 year old male with chest pain and mottled lower extremities. Diagnosis?

36
Keep up the good work NYCOM Students!!!!
Thank You..

Similar presentations







 –Partial.>")













