Download presentation
Presentation is loading. Please wait.

1
X-ray Interpretation

2
Objectives • List the reasons for obtaining a Chest x-ray
Identify anatomical structures present on a chest film. • Recognize a normal chest radiograph. • Recognize and name the radiographic signs of atelectasis, consolidation, pneumothorax, pleural effusions, and hyperinflation frequently seen in patients with cardiopulmonary disease.

3
A Chest x-ray is very valuable in answering the following questions
Thus, one can easily see the cost-effectiveness of this relatively simple test. In patient's with lung or heart disease, chest x-rays obtained at yearly, or longer, intervals may provide information about the progression, stability or improvement of disease. Is the heart enlarged or normal? Are there signs of heart failure and fluid overload? Does the patient have pneumonia or a collapsed lung? Is there evidence of emphysema? Are there findings of an aneurysm involving the aorta? Is there fluid in the sac that surrounds the lung? Is there free air under the diaphragm to suggest a hole in the bowel wall? Is there a tumor in the lung that could represent cancer? Are there changes of bronchitis or emphysema?

4
Standard PA or posterior – anterior Radiograph
Patient usually upright Distance of beam determines magnification and clarity • Place the films on the view box as though you were facing the patient with his left on your right side.

5
Standard Lateral Chest Radiograph
Left side of the chest against filmholder (cassette); beam from right at a distance of six feet; Lesions located behind the left side of the heart or in the base of the lung are often invisible on the PA view because the heart or diaphragm shadow hides it the lateral will generally show such lesions
; beam from right at a distance of six feet; Lesions located behind the left side of the heart or in the base of the lung are often invisible on the PA view because the heart or diaphragm shadow hides it. the lateral will generally show such lesions.")
6
X-rays are a study of densities
DENSITIES Air < fat < liver < blood < muscle < bone < barium < lead. Air — least dense; most transparent or radiolucent; unobstructed beam or air-filled densities appear black Lungs, gastric bubble, trachea, ? bifurcation of bronchi Fat — breasts Fluid — most of what you see; vessels, heart, diaphragm, soft tissues, mediastinal structures Mineral — most dense (or radiopaque) of body structures; mostly Ca++; bones (marrow is aerated), aortic calcifications such as the aortic knob, ? calcification of the coronary arteries, old granulomas; bullets, safety pins, etc.
 of body structures; mostly Ca++; bones (marrow is aerated), aortic calcifications such as the aortic knob, calcification of the coronary arteries, old granulomas; bullets, safety pins, etc.")
7
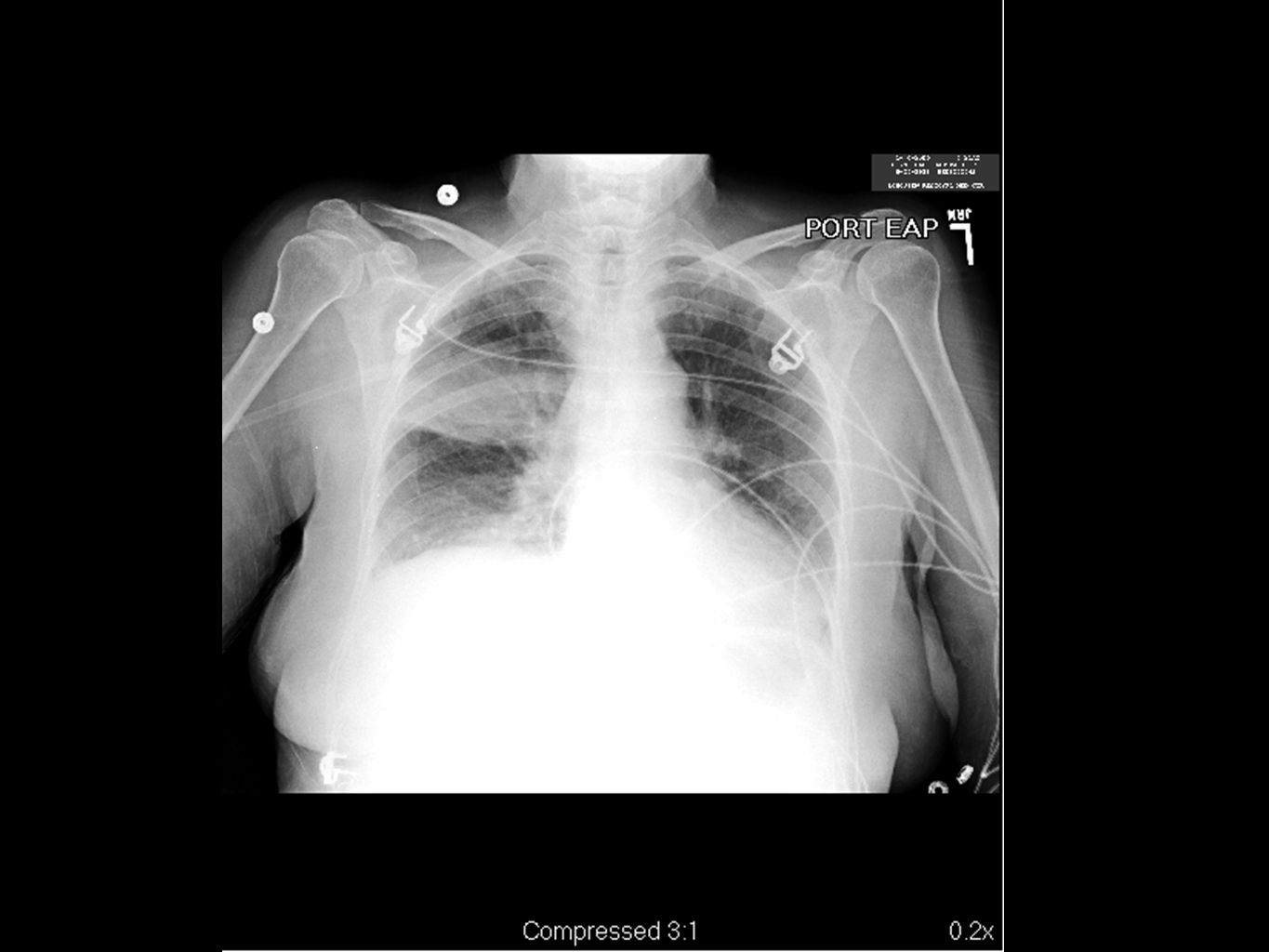
Different Densities on an ICU Chest X-ray

8
Anatomy Silhouette Sign / Air Bronchogram

9
What am I looking at?

10
What am I looking at?

11
Right Upper Lobe

13
Right Middle Lobe

14
Right Lower Lobe

15
Left Upper Lobe

16
Left Lower Lobe

17
Normal Cardiac Anatomy (PA view)
On PA projection, the right cardiac border is formed by the right atrium while the left cardiac border is formed by the left ventricle. The right ventricle and left atrium are superimposed structures and are not border forming. The Superior vena cava: forms a right paramedian border. 1 = right brachiocephalic vessels 2 = ascending aorta and superimposed SVC 3 = right atrium (RA) 4 = inferior vena cava (IVC) 5 = left brachiocephalic vessels 6 = aortic knob/arch 7 = pulmonary trunk 8 = left atrial appendage (LA) 9 = left ventricle (LV)
 4 = inferior vena cava (IVC) 5 = left brachiocephalic vessels 6 = aortic knob/arch 7 = pulmonary trunk. 8 = left atrial appendage (LA) 9 = left ventricle (LV)")
19
Normal Cardiac Anatomy (Lateral view)
")
21
Comparing normal to copd lateral

22
Pleura

23
How to Read a Chest X-ray
Go from general observations to specific details. Sometimes a change may be so major that the old saw about missing the forest for the trees comes true. Read the Chest X-ray in a systematic fashion: L shoulder L chest wall Lower Chest R chest wall R shoulder Cervical spine and soft tissue Chest / Ribs Hilum Lungs Pleura

24
LEFT SHOULDER GIRDLE Soft tissues - look at overall amount, then check for the following: calcifications, obvious mass effect, abnormal air collections Bones - look at each bone for abnormalities Joints- are articular relationships normal, joint spaces narrowed, widened, any calcification in the cartilages, air in the joint space, abnormal fat pads, etc.

25
LEFT SHOULDER GIRDLE

26
LEFT CHEST WALL Look for overall thickness, subcutaneous emphysema, calcification. Look for sharp, distinct muscle fat planes

27
BREAST TISSUE In males and females, some asymmetry can occur from standing with unequal pressure against the film holder. Notice how the apparent lung density changes from the lung area covered by the soft tissue of the breast to the lung area inferior to the breast.

28
ABDOMEN The visibility of structures is highly variable
Gastric and bowel gas - Is amount and location normal? Check for free peritoneal air position of patient will change location of free air. Look for calcifications and masses - can they be localized to a specific structure.

29
RIGHT CHEST WALL Look for overall thickness, subcutaneous emphysema, calcification. Look for sharp, distinct muscle fat planes.

30
RIGHT SHOULDER GIRDLE

31
NECK SOFT TISSUES AND SPINE
Amount of soft tissue, presence of calcifications, subcutaneous emphysema, position and size of trachea. For the cervical spine, check alignment and note any major congenital abnormalities. Then look at specific parts of the vertebra and disc spaces, checking for erosions, boney destruction, disc / joint narrowing or other abnormalities.

32
THORACIC SPINE AND RIB CAGE
Concentrate on the skeletal detail -- "look through" the mediastinum and lungs. First check overall alignment of the spine and symmetry of the rib cage, double check bone density (this is a gross estimate).
.")
33
RIBS Compare individual ribs side to side 1. Posterior rib
2. Anterior Rib

34
Hilum (pleural = hila.) "lung root;" medusa-like tangle of arteries and veins on either side of the heart shadow. Irregular medial shadow in each lung where the bronchi and pulmonary arteries enter. Other structures in these areas, particularly lymph nodes, are normally so small as to be unapparent.

35
Pulmonary hilum

36
FRONTAL VIEW OF THE HILA
On the frontal view most of the hilar shadows are the left and right pulmonary arteries. The left pulmonary artery is always more superior than the right, thus making the left hilum appear higher. Calcified lymph nodes may be visible within the hilar shadows.

37
LATERAL VIEW OF THE HILA

38
Hilar Adenopathy

39
Hilar Adenopathy

40
Lungs

41
LUNGS Compare overall size of one lung to the other,
Look for major areas of abnormal lucency or density

42
Pleura

43
Pleura Check the frontal view for minor fissure thickness and location, and on the lateral view, look for minor and major fissures These are normally fine delicate structures that do not show up on the digitized images.

44
Pleura

46
Stomach Anatomy

49
Let’s look at some examples

50
Terminology Silhouette sign Atelectasis Consolidation Pneumothorax
Pleural effusion Nodule Hyperinflation Loculated Lateral Decubitus

51
Silhouette Sign When two objects of the same
density touch each other, the edge between them disappears A B

52
Using the Silhouette Sign
Right middle lobe silhouettes right heart border Lingula silhouettes left heart border Right lower lobe silhouettes right hemidiaphragm Left lower lobe silhouettes left hemidiaphragm Where is this patient’s heart?

53
Silhouette Sign

54
Silhouette of the Right Heart Border
Right middle lobe Infiltrate showing obliteration of the right heart border

55
Atelectasis = collapse (volume loss)
To diagnose atelectasis, there must be evidence of volume loss such as displacement of a fissure or hilum.

56
Atelectasis of right lung – shift of the mediastinal structures TOWARDS the side of opacification

57
Tension Pneumothorax

58
Pleural Effusion

59
Loculated Hydropneumothorax

60
Pulmonary Nodule

61
Hyperinflation

63
Hyperinflation

64
Pneumonia

65
Subpulmonic effusion

66
Final Exam

69
Conclusion Should be able to look at a CXR and determine whether it is normal Identify obvious abnormalities on the CXR, including boney, soft tissue, cardiac and pulmonary pathology Be able to understand basic radiology terminology

Similar presentations















 –Partial.>")











