Download presentation
Presentation is loading. Please wait.

1
Techniques for Practical 1
Year One Block 2 Cervical, Thoracic, Shoulder, Elbow, Wrist

2
Opponen’s Roll Grasp first digit (thenar emin.) and fifth digit (hypothenar emin.) with each hand Contact pisiform and navicular (scaphoid) bones with thumbs Extend wrist, abduct and laterally rotate first digit with counterforce over hypothenar area Use thumbs to stretch at boney contact points the transverse carpal ligament in lateral/medial direction
 bones with thumbs. Extend wrist, abduct and laterally rotate first digit with counterforce over hypothenar area. Use thumbs to stretch at boney contact points the transverse carpal ligament in lateral/medial direction.")
3
Treatment for Abduction Somatic Dysfunction of the Wrist
Doctor and patient facing each other, seated or standing Doctor grasps patient’s wrist and places it into pronation and abduction Doctor moves patient’s wrist from the original position in abduction to and just past the adduction barrier in a smooth gentle motion. the picture shows the final position of the wrist and hand no nicholas reference

4
Treatment for Adduction Somatic Dysfunction of Wrist
Doctor and patient facing each other, seated or standing Doctor grasps patient’s wrist and places it into pronation and adduction Doctor moves patient’s wrist from the original position in adduction to and just past the abduction barrier in a smooth, gentle motion the picture shows the final hand position. Note that these 2 treatments are HVLA treatments, but they don’t follow the usual rules for HVLA. usually with HVLA we place the patient right up against the barrier and make a very small, quick thrust. In these 2 cases, we start away from the barrier and make larger, but still quick, thrusts toward the barrier. no nicholas reference

5
Direct, Articulatory – Wrist Ab-/Ad-duction S/D
Grasp pronated wrist and contact posterior surface joint margin with thumbs Apply traction and carry wrist into direction of dysfunction Gently articulate toward the restricted barrier with low to medium velocity and medium amplitude.

6
Treatment of Flexion Somatic Dysfunction
Patient seated, doctor standing or sitting facing patient. Doctor grasps the patient's wrist with the doctor’s thumbs on the dorsal aspect of the wrist, pressing on the dysfunctional bone. The doctor may reinforce the pressure of the treating thumb by adding pressure with the other thumb. The doctor’s hands wrap around the wrist to contact the palmar aspect of the patient’s hand. The patient’s wrist is initially held in flexion A simple repeated motion is carried out, moving the wrist from flexion to extension, while maintaining pressure over the displaced carpal bone. Flexion Somatic Dysfunction = Dorsal Carpal Dysfunction The Nicholas text says that traction is not needed for this technique. However, if you want to use traction, you can try it and see how it works for you. If you choose to use traction, realize that it will only be a small amount

7
Treatment of Extension Somatic Dysfunction
Patient seated, doctor standing or sitting facing patient. Doctor grasps the patient's wrist with the doctor’s thumbs on the dorsal aspect of the wrist, resting on the dysfunctional bone. The doctor’s hands wrap around the wrist so that the index fingers can press on the dysfunctional bone. The patient’s wrist is initially held in extension. A simple repeated motion is carried out, moving the wrist from extension to flexion, while maintaining pressure over the displaced carpal bone. There is no Nicholas reference for this technique, but it is basically the reverse of the previous one. It is in kimberly Sitting Direct HVLA

8
Squeeze w/Circumduction (4760.11A)
Place heel of both hands over radiocarpal region of carpal bones & interlace fingers Attempt to distract fingers while squeezing fingers together Causes the heel of each hand to squeeze together Circumduct wrist in circular or figure eight fashion

9
Radioulnar Interosseous Membrane, Direct Method
Pt. sits and physician stands in front Hold supinated forearm in palms of both hands with physician thumbs crossed over the anterior surface of the pt. forearm with the interosseous dysfunction between the thumbs. Contact the lateral side of the ulna with one thumb and the medial side of the radius with the other thumb

10
Muscle Energy technique continued
Pt. is instructed to “turn palm downward” while physician offers isometric counterforce. PRONATION!! Maintain counterforce 3-5 seconds and both pt. and physician simultaneously relax Take up the slack and repeat (usually 3x) RECHECK YOUR FINDINGS!!
 RECHECK YOUR FINDINGS!!")
12
Tx: Radial Head Posterior- Direct Muscle Energy
Correct Abduction or Adduction first Contact the posterior aspect of radial head with thumb of lateral hand Grasp distal radius and ulna and engage barrier with forearm supination & wrist extension Patient attempts to pronate (Dr. resists) Relax, engage new barrier Dr.’s thumb and supination force will move radial head anterior Thumb on anterior distal radius supinate *
 Relax, engage new barrier. Dr.’s thumb and supination force will move radial head anterior. Thumb on anterior distal radius. supinate. *")
13
Tx: Radial Head Anterior- Direct Muscle Energy
Grasp the hand on the side of the dysfunction contacting the dorsal aspect of the distal radius with the thumb

14
Tx: Radial Head Anterior, continued
The physician’s other hand is palm up with the thumb resting against the anterior and medial aspect of the radial head The physician pronates the patient’s forearm to the edge of the restrictive barrier. Tell the patient to supinate and use an isometric force. Hold 3-5 seconds, stop and relax. Take up the slack to the new restrictive barrier. Repeat 3-5 times RECHECK FINDINGS!!!

15
Dx of Ulnar Abduction and abduction motion testing
Pt seated/ Dr. Standing Dr. contacts patient’s elbow and wrist at elbow - thenar eminence to medial aspect of olecranon and finger to lateral condyle - apply force with finger to thenar (+) extending arm from elbow while attempting adduction is met with resistance (olecranon will not laterally glide) Pt may experience pain and crepitus may occur as the olecranon seats in the olecranon fossa.
 extending arm from elbow while attempting adduction is met with resistance (olecranon will not laterally glide) Pt may experience pain and crepitus may occur as the olecranon seats in the olecranon fossa.")
16
Tx of Ulnar Abduction with Medial Glide SD: Direct Technique - Ariticulatory - 4741.11B
Patients elbow flexed ~ 90o with Dr firmly grasping distal forearm from lateral aspect Dr. grasps the elbow with thenar eminence on medial margin of olecranon and fingers on lateral condyle apply lateral and slightly superior force at medial contact and adduction force at distal forearm Take arm into full Extension in a sweeping motion applying the same forces above.

17
Tx of Ulnar Adduction with Lateral Glide SD: Direct Technique - Articulatory - 4742.11B
Pt seated/Dr standing Patients elbow slightly flexed ~ 90o. Dr firmly grasps distal forearm from medial aspect Dr. grasps the elbow with thumb or thenar eminence to lateral margin of olecranon apply medial and slightly superior force at lateral contact and abduction force at distal forearm engaging the barrier. Take arm into full extension in a sweeping motion applying the same forces above.

18
Sternoclavicular Dysfunction Assessment
ABduction (IG)/ADduction (SG) DO at head of table, patient supine DO monitors medial clavicle area Patient shrugs their shoulders. Both clavicles should move into Abduction, and the medial clavicles should move inferiorly In the absence of trauma, the dysfunctional (restricted) clavicle stays superior at the SC jointNamed an ADduction somatic dysfunction (superior glide) Example of a superior left SC joint
/ADduction (SG) DO at head of table, patient supine. DO monitors medial clavicle area. Patient shrugs their shoulders. Both clavicles should move into Abduction, and the medial clavicles should move inferiorly. In the absence of trauma, the dysfunctional (restricted) clavicle stays superior at the SC jointNamed an ADduction somatic dysfunction (superior glide) Example of a superior left SC joint.")
19
Sternoclavicular Dysfunction Assessment
Horizontal Flex (PG)/Horizontal Ext (AG) DO at head of table, patient supine Monitor the medial clavicle Patient reaches toward the ceiling with their arms. Their scapulae should come off the table. Both clavicles should move into horizontal flexion, and the medial clavicles should move posterior (posterior glide) In the absence of trauma, the dysfunctional (restricted) clavicle stays anterior at the SC jointNamed a horizontal extension (anterior glide) somatic dysfunction Example of an anterior SC
/Horizontal Ext (AG) DO at head of table, patient supine. Monitor the medial clavicle. Patient reaches toward the ceiling with their arms. Their scapulae should come off the table. Both clavicles should move into horizontal flexion, and the medial clavicles should move posterior (posterior glide) In the absence of trauma, the dysfunctional (restricted) clavicle stays anterior at the SC jointNamed a horizontal extension (anterior glide) somatic dysfunction. Example of an anterior SC.")
20
SC Joint – Articulatory method
Thumb on medial clavicle with caudad pressure Patient’s arm brought in a “backstroke” pattern – towards flexion through adduction and abduction and then ending up in extension Reassess

21
AC joint – Articulatory method
DO grasps patient elbow or forearm from behind DO monitors lateral edge of clavicle anteriorly with finger pads DO applies anterior/inferior pressure on the lateral side of the clavicle with thumb, flexes the patient’s elbow and extends and adducts the humerus to gap the AC joint DO further extends the shoulder and a circulatory articular sweep is applied – carry the elbow posteriorly superiorly anteromedially while maintaining adduction and capsular tension Recheck

22
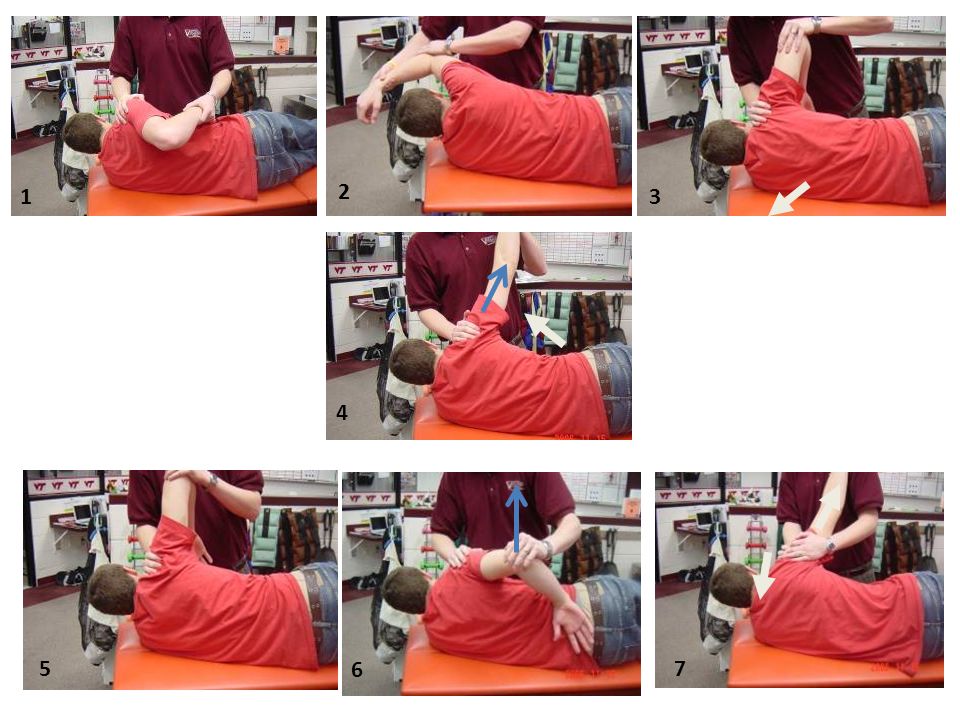
Spencer Technique The seven stages of motions are:
1. Engage GH extension barrier with elbow flexed 2. Engage GH flexion barrier with the elbow flexed 3. Circumduction with compression Start small circles, then gradually increase size Clockwise and counterclockwise May also do ME of IR/ER barriers 4. Traction with circumduction on straight arm Start small circles, then gradually increase size Clockwise and counterclockwise 5. Engage abduction barrier 6. Internal rotation with elbow flexed 7. GH pump with distraction and compression along straight arm Kimberly Manual, p Direct articulatory/ME

23
1 2 3 4 5 6 7
24
Myofascial release of the T spine

25
Myofascial release of the Scapula

26
Anterior TP 1-2 tx

27
Ant TP 3-6 tx

28
Ant TP tx T 7-9

29
Posterior midline TP tx

30
Post lateral TP tx

31
Suboccipital Inhibition
Objective: decrease suboccipital (SO) muscle tone 1) doctor at head of table; patient supine. 2) Pads of fingers just beneath superior nuchal line in the SO tissues 3) Lift head slightly so its entire weight is supported on fingers
 muscle tone. 1) doctor at head of table; patient supine. 2) Pads of fingers just beneath superior nuchal line in the SO tissues. 3) Lift head slightly so its entire weight is supported on fingers.")
32
Kneading Objective: Relax the cervical paravertebral muscles (PVM).
1) doctor standing on patient’s side; patient supine. 2) With caudad hand, reach across patient and cup PVM; Place cephalad hand on pt’s forehead 4) Push head away from you, then pull up and laterally on PVM tissue letting head roll back toward you.
 doctor standing on patient’s side; patient supine. 2) With caudad hand, reach across patient and cup PVM; Place cephalad hand on pt’s forehead. 4) Push head away from you, then pull up and laterally on PVM tissue letting head roll back toward you.")
33
Forward bending stretching
Objective: Stretch posterior cervical tissues 1) doctor at head of table; patient supine. Cross forearms and place them behind pt’s head with fingertips on pt’s shoulders. Exert slow forward bending stretch until a restrictive barrier is engaged, slowly increase to next barrier
 doctor at head of table; patient supine. Cross forearms and place them behind pt’s head with fingertips on pt’s shoulders. Exert slow forward bending stretch until a restrictive barrier is engaged, slowly increase to next barrier.")
34
Trapezius Stretch Objective: Relax the trapezius muscle
1) Patient supine, doctor at head of table 2) Stabilize one shoulder with opposite hand 3) With free hand contact same side of head as stabilized shoulder and introduce GENTLE stretch
 Patient supine, doctor at head of table. 2) Stabilize one shoulder with opposite hand. 3) With free hand contact same side of head as stabilized shoulder and introduce GENTLE stretch.")
35
Longitudinal Stretching
Objective: Relax the paravertebral muscles (PVM). 1) doctor at head of table; patient supine. 2) palmar surfaces of fingers of both hands under the neck near spinous processes 3) lift PVM with fingers and draw it toward you (cephalad = toward head) 4) release and carry tissue away from you (caudally = toward tail)
. 1) doctor at head of table; patient supine. 2) palmar surfaces of fingers of both hands under the neck near spinous processes. 3) lift PVM with fingers and draw it toward you (cephalad = toward head) 4) release and carry tissue away from you (caudally = toward tail)")
36
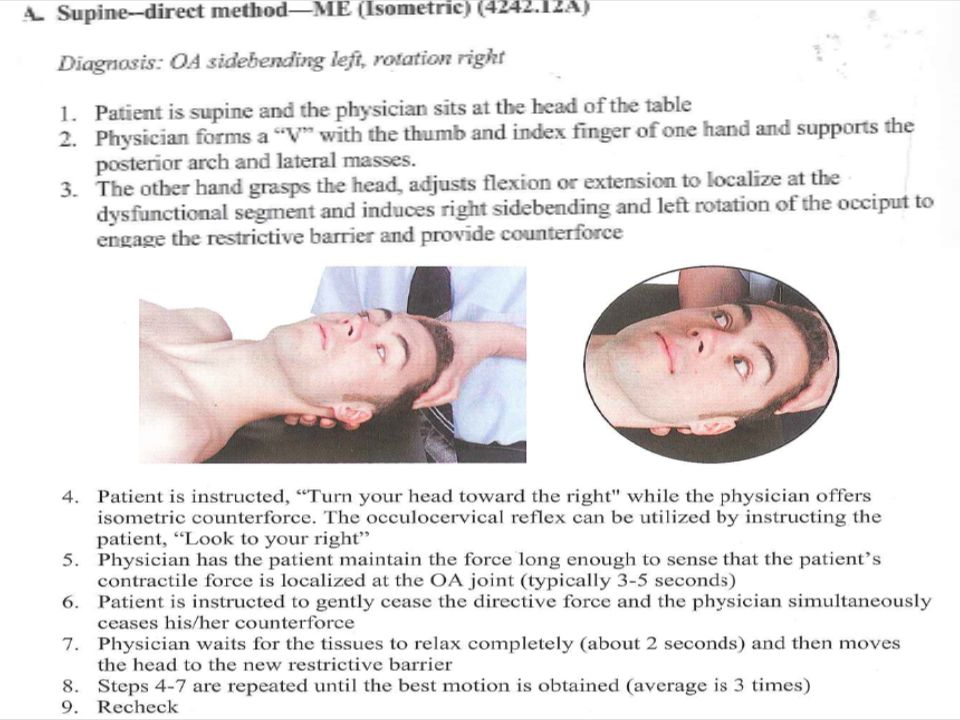
OA Joint Supine Direct ME – Flexion SD
Pt is supine & DO at head of table Support lateral masses of atlas between index finger & thumb Use other hand to grasp pt’s head and induce extension of the occiput to restrictive barrier Instruct pt to “Nod your chin toward your throat” while DO offers isometric counterforce & localizes to the OA joint Instruct pt to relax & engage new restrictive barrier Repeat steps 3-4 times & recheck

37
OA Joint Supine Direct ME – Extension SD
Pt is supine & DO at head of table Support lateral masses of atlas between index finger & thumb Use other hand to grasp pt’s head and induce flexion of the occiput to restrictive barrier Instruct pt to “Raise your chin upward” while DO offers isometric counterforce & localizes to the OA joint Instruct pt to relax & engage new restrictive barrier Repeat steps 3-4 times & recheck

38
Pinch Technique for Sagittal Plane OA Flexion and Extension
Examiner sitting at patient’s side Stabilize tubercle of C1 with thumb and forefinger Cradle occiput in other hand Rock occiput forward and back Appreciate quality of movement

39
Multiple Plane Somatic Dysfunction of OA joint
Because of the ANATOMY of the condyles, the OA side-bends and rotates to opposite sides in either flexion or extension OA (F) or (E) SL RR OA (F) or (E) SR RL Brain attempts to keep the “eyes level on the horizon” at all cost OA asymmetries are compensated by activating the sub-occipital mm
 or (E) SL RR. OA (F) or (E) SR RL. Brain attempts to keep the eyes level on the horizon at all cost. OA asymmetries are compensated by activating the sub-occipital mm.")
40
Multiple Plane Somatic Dysfunction of OA joint
Inspection “Is this patient’s head on straight?” Look for deviation of the chin and tip of nose from the mid-line position

42
Somatic Dysfunction of the AA Joint
Motion testing Forward bend patient’s head to “lock-out” lower vertebrae Rotate left, rotate right Compare, assess, diagnose...

43
Diagnosis of the AA Test seated active & passive motion. (regional scanning) Test supine motion specific to AA. Flex head beyond 45o, then rotate patient’s head passively. Supine, inspect & palpate. T-A-R-T!!! C1 lateral masses located between mastoid process and ramus of mandible. Supine, localized motion testing of the AA Compare right verses left rotation. ***And remember!!! -- Somatic dysfunction at the AA joint is descriptive only of the motion of the atlas on the axis (C1 on C2) *** = AA left rotation or AA right rotation FOR EXAMPLE: Usual findings (eg. Left rotation) Transverse process and lateral mass of C1 (Atlas) are posterior on L tip near mastoid process Transverse process and lateral mass of C1 (Atlas) are anterior on R tip near angle of mandible MOTION present to L (L rotation) Diagnosis: AA left rotation: AARL or AA right rotation: AARR
 *** = AA left rotation or AA right rotation. FOR EXAMPLE: Usual findings (eg. Left rotation) Transverse process and lateral mass of C1 (Atlas) are posterior on L tip near mastoid process. Transverse process and lateral mass of C1 (Atlas) are anterior on R tip near angle of mandible. MOTION present to L (L rotation) Diagnosis: AA left rotation: AARL or AA right rotation: AARR.")
44
Direct, Muscle Energy of AA- 4231.11B
Forward bend head to >45o To lock out lower cervicals MCP joint of the index finger contacts lateral mass of atlas (C1) on posterior rotated side Rotate into barrier (maintain flexion) Sweeten with SB Instruct patient to turn his/her head the opposite direction against your force - use isometric force for 3-5 sec. Upon relaxation, engage the new barrier & repeat M.E. 2-3 more times MCP joint = metacarpal-phalangeal joint Remember Obliquus capitus inferior (suboccipital muscle) origin: SP C2 insertion: TP C1 function: rotate C1 to same side
 on posterior rotated side. Rotate into barrier (maintain flexion) Sweeten with SB. Instruct patient to turn his/her head the opposite direction against your force - use isometric force for 3-5 sec. Upon relaxation, engage the new barrier & repeat M.E. 2-3 more times. MCP joint = metacarpal-phalangeal joint. Remember Obliquus capitus inferior (suboccipital muscle) origin: SP C2. insertion: TP C1. function: rotate C1 to same side.")
45
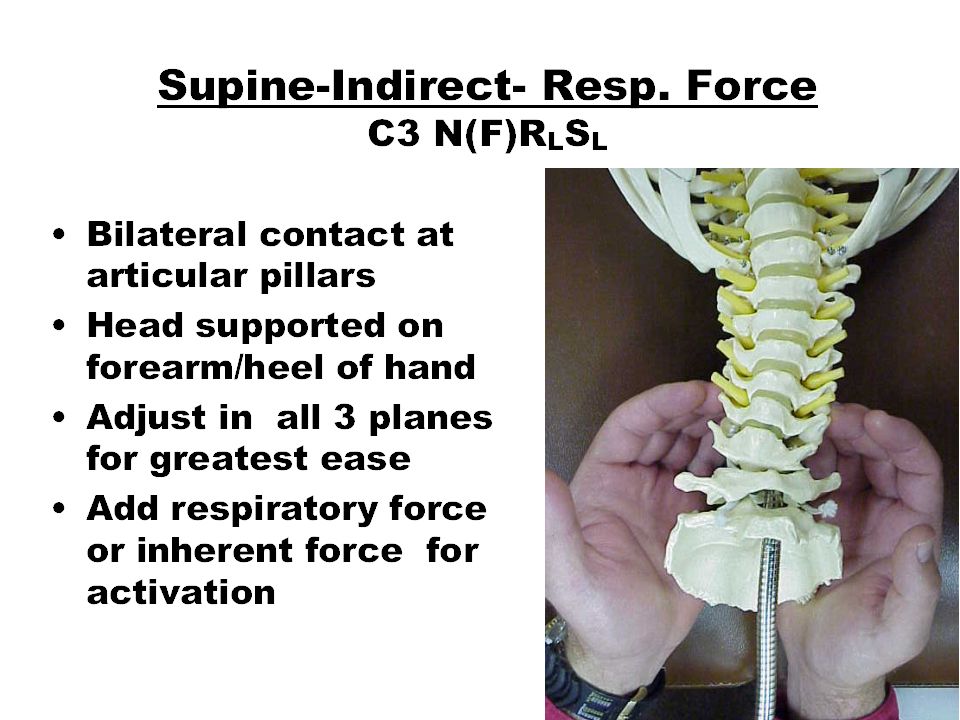
Supine-Direct-ME C3 NRLSL
Reach under spine to contact the convex side. Pull with fingers to induce Right Sidebending (reverse the curve)
")
46
ME for Typical Cervical RLSL

48
Jones Strain-Counterstrain Anterior C1 Tender Point
A.k.a the OA joint TP High on posterior ascending ramus of mandible Contact TP & rotate away 90º Find it, fold it, hold it, recheck! REVIEW!!!

50
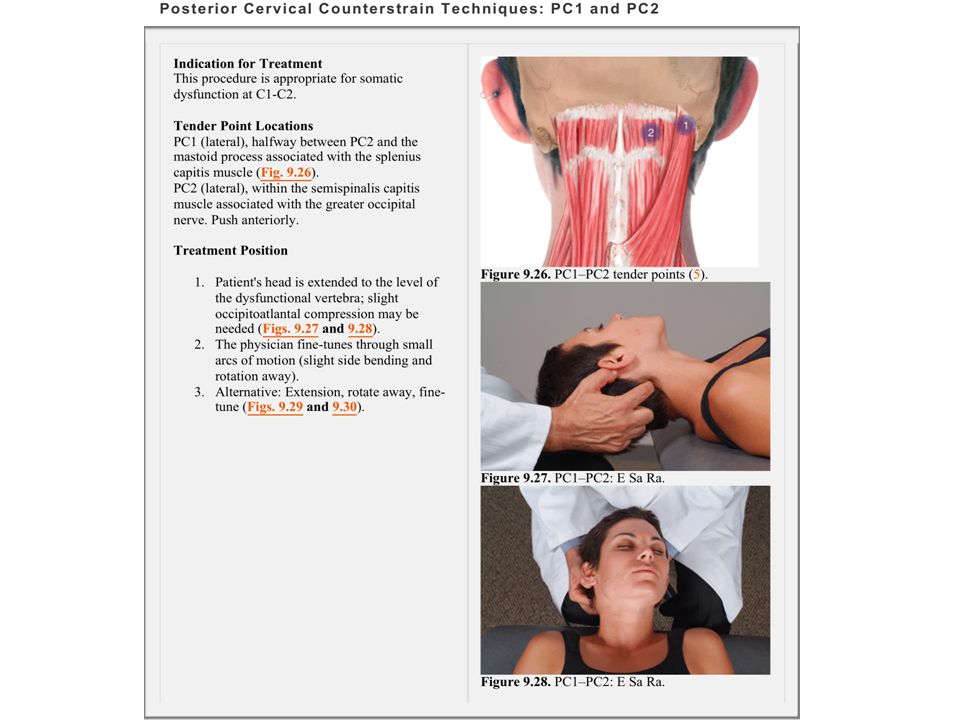
Indication for Treatment This procedure is appropriate for somatic dysfunction at C3 to C7. Tender Point Location The tender point lies at PC3 to PC7 posterolateral, at lateral surface of the articular process associated with the dysfunctional segment (Fig. 9.36). Treatment Position The physician extends the head and neck to the level of the dysfunctional segment with minimal to moderate side bending directed at the segment and minimal to moderate rotation away (Figs. 9.37, 9.38, 9.39, 9.40, PC3, PC3, PC6, and PC6, respectively). The physician fine-tunes. PC3 TP- eSaRA
. The physician fine-tunes. PC3 TP- eSaRA.")
Similar presentations











 Lecture 3 Myology of the Elbow.>")
 While standing upright with feet.>")






 While standing upright with feet.>")
