Download presentation
Presentation is loading. Please wait.

1
RADIOGRAPHY Makes use of high energy photons called X-rays Have the ability to pass thro’ matter/tissue some of the x-ray photons are absorbed (attenuated) by the matter/tissues depending on the density, atomic number and the thickness of the tissue i.e. the higher the d.a.t. (Density, Atomic number, Thickness) of a tissue the more x- rays that tissue will absorb. Tissues that absorb a lot of X-rays appear white (OPAQUE) while those that do not absorb much of X- rays appear black (LUSCENT) on radiographs
 of a tissue the more x- rays that tissue will absorb. Tissues that absorb a lot of X-rays appear white (OPAQUE) while those that do not absorb much of X- rays appear black (LUSCENT) on radiographs.")
2
Chest Radiographs PA (posterior to anterior) and Lateral (left) Minimizes magnification of heart (heart closest to film) Portable (nearly always AP) Supine or Erect Specialized Views Lordotic Lateral decubitus (for effusions, pneumothorax)
 and Lateral (left) Minimizes magnification of heart (heart closest to film) Portable (nearly always AP) Supine or Erect Specialized Views Lordotic Lateral decubitus (for effusions, pneumothorax)")
3
FROM THE PA EXAM WE CAN EVALUATE POSITIONS RIGHT OR LEFT AND SUPERIOR OR INFERIOR. THE LATERAL EXAM HELPS TO IDENTIFY STRUCTURES RELATIVE TO THE ANTERIOR OR POSTERIOR AND SUPERIOR OR INFERIOR PLANES.

4
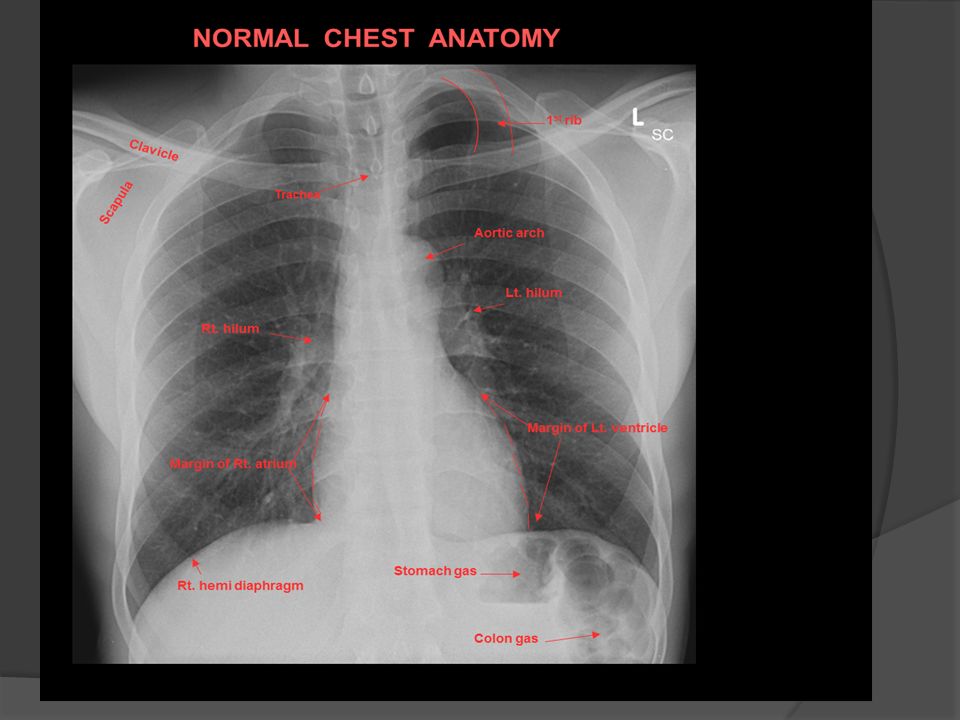
Chest Radiograph: Approach and Normal Anatomy THERE IS NO ONE APPROACH: BE SYSTEMATIC Bone and Soft Tissue including abdomen Heart Mediastinum-aorta, trachea Hila Pulmonary Vasculature Lungs Pleura

7
NORMAL ANATOMY PA View Clavicle Rib Intercostal Space Vertebral Column

8
Sternum Rib Bone Anatomy

9
Heart Size Normal is <50% on PA upright radiograph

10
NORMAL HEART

11
Cardiac Anatomy: Right Sided Chambers

12
Cardiac Anatomy: Left Sided Chambers

13
NORMAL HEART BORDERS

14
SVC Aortic Arch Right Descending Pulmonary Artery Left Descending Pulmonary Atery

15
Lungs posteriorly should get darker as you go down more inferiorly Retrosternal Airspace Scapula IVC Pulmonary Vessels Hilum

16
Airway Anatomy Trachea Cartilage Membranous posteriorly Carina Bifurcation Bronchus Left and right Lobar (RUL,RML,LUL,LLL) Segmental (8 left, 10 right)
 Segmental (8 left, 10 right)")
17
Trachea Carina R + L Main Bronchi

18
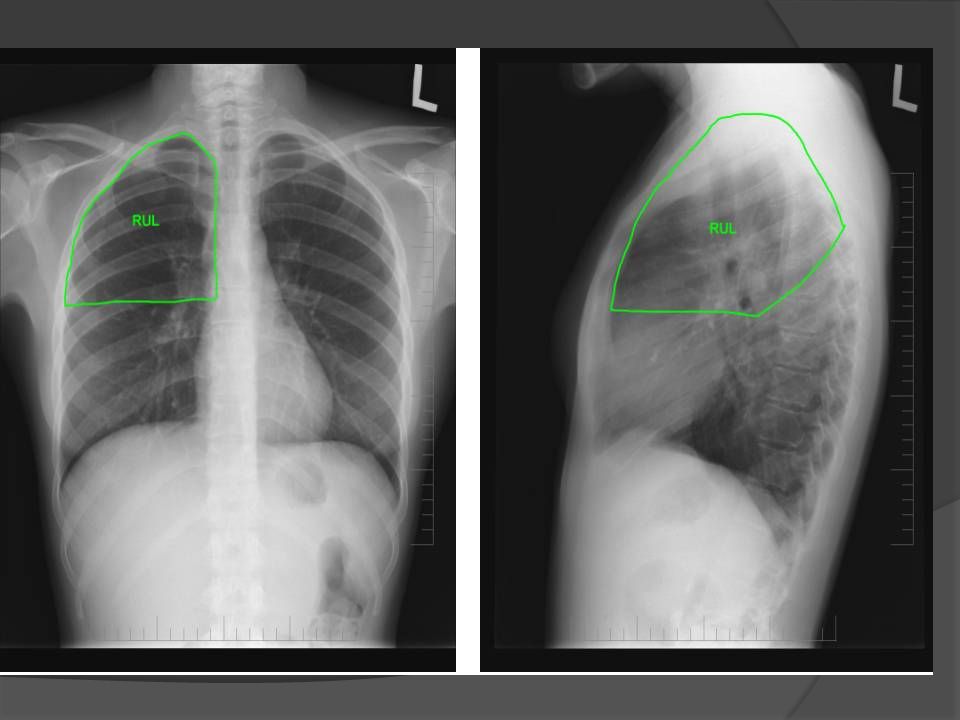
Lung Anatomy Lobes are separated by fissures Right Upper Lobe Middle Lobe Lower Lobe Left Upper Lobe (includes lingula) Lower Lobe
 Lower Lobe")
24
Pleura and Fissures Pleura Lubricates and prevents friction during respiration Potential Space – Don’t see unless abnormal Parietal pleura: Lines chest wall, mediastinal and diaphragmatic surfaces Visceral pleura: Lines lungs, fissures

25
Parietal Pleura Visceral pleura

26
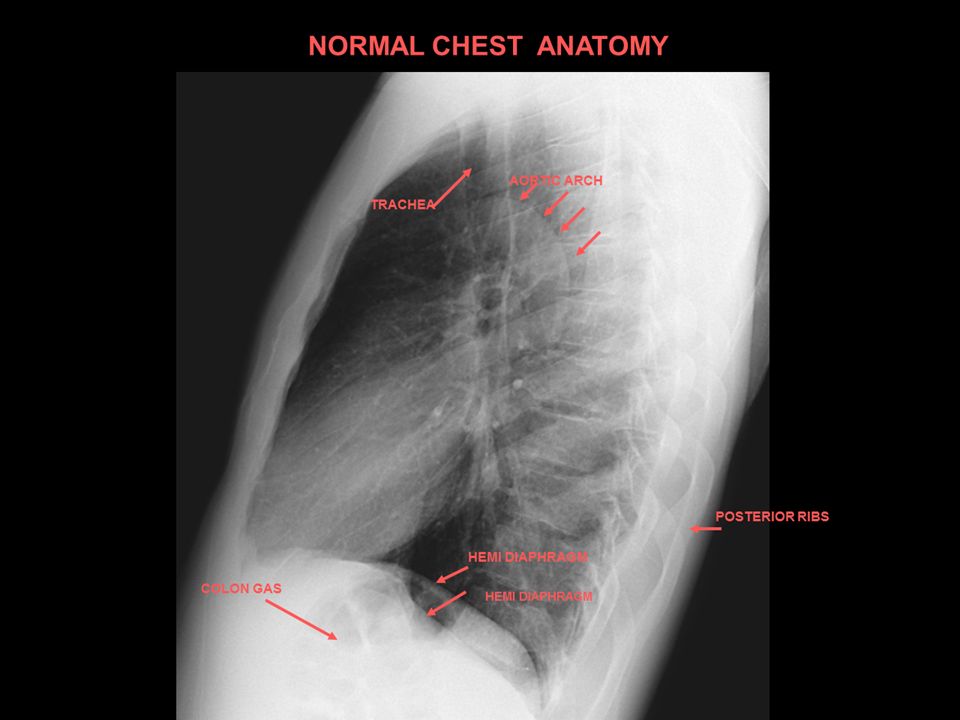
AORTIC ARCH LT. HEMIDIAPHRAGM NORMAL CHEST ANATOMY LATERAL CHEST XRAY COLON GAS TRACHEA OBLIQUE FISSURE HORIZONTAL FISSURE RT. HEMIDIAPHRAG M Diaphragm-AP view Diaphragm- Lateral view LT. RT. LT.

27
HORIZONTAL FISSURE FISSURES DIVIDE LUNGS INTO LOBES RIGHT lung has: UPPER MIDDLE lobes LOWER LEFT lung has: UPPER lobes LOWER

28
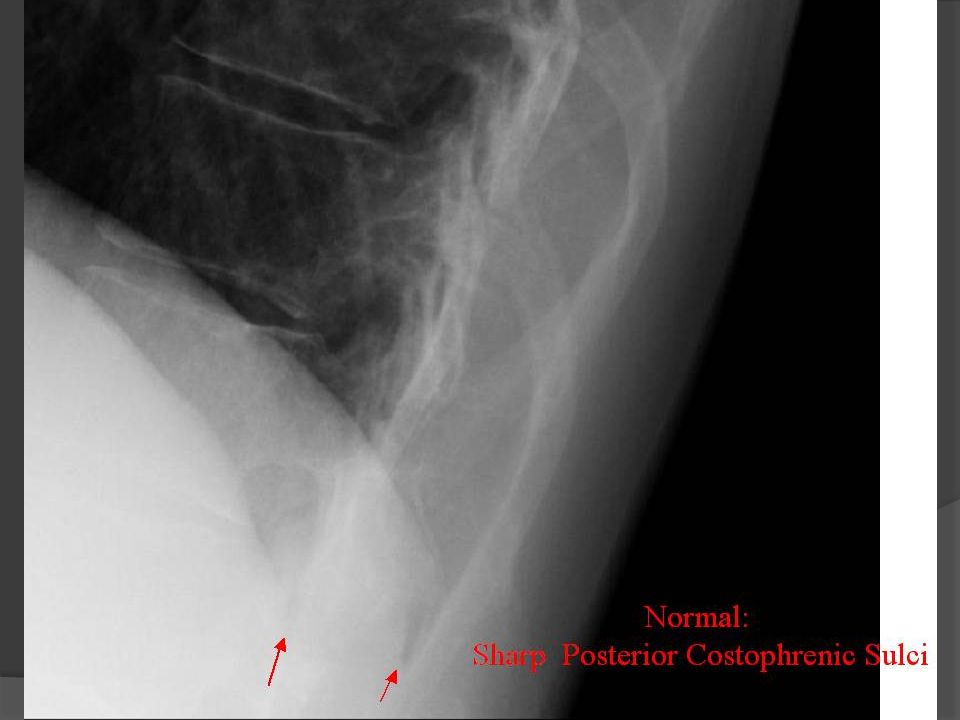
Diaphragms Normal: Sharp costophrenic sulcus

30
Which is right and left diaphragm?

32
Approach to Chest Radiograph: Technical Factors Patient Identification (name and date) Markers (Left vs right) Assess for rotation (clavicles vs spinous process) Penetration (thoracic spine should be visible) Degree of Inpiration: 6 th anterior or 10 th posterior
 Markers (Left vs right) Assess for rotation (clavicles vs spinous process) Penetration (thoracic spine should be visible) Degree of Inpiration: 6 th anterior or 10 th posterior")
33
Inspiration/Expiration Images Expiration Heart size appear larger Mediastinum is wider Pulmonary vasculature indistinct

34
Inspiration: Same Patient Expiration Expiration: Breathing out: the size of heart looks wider compared with inspiration, also lungs appear to be lighter (whiter) due to lack of air. Inspiration: Breathing in: the size of heart looks normal (smaller than that in Expiration). Also lungs appear to be darker due to full-air expanded lung tissue.
. Also lungs appear to be darker due to full-air expanded lung tissue..")
35
Abnormal Cases Bone Cardiovascular Airspace Disease including Silhouette Sign Interstitial Disease and Pulmonary Edema Atelectasis Pulmonary Nodule Pleura and Diaphragm Mediastinal Mass

36
Fractures Right side ribs are clearly separated from each others where we can see a gap or darkness between two pieces of light (white) bone images
 bone images")
37
37154 slides Increased Cardiac Size: Can be Cardiac or Pericardial Pericardial EffusionDilated Cardiomyopathy 37

38
38 Normal lung Individual alveoli are too small to resolve, but together they appear radiolucent.

39
39 Air-space Disease Filling of alveoli by: water, blood, pus, proteinaceous fluid, or cells -opacities -consolidation

40
Air-space pattern of lung disease 40

41
41154 slides Bronchopneumonia Pattern: Airspace Nodules 41

42
42154 slides Right Lower Lobe Pneumonia Left Right: Partially seen 42

43
43154 slides Left Lower Lobe Pneumonia 43

44
Where is the pneumonia?

45
45

46
46154 slides Right Middle Lobe Pneumonia 46

47
THE FLAT BORDER ALONG THE INFERIOR MARGIN OF THE PNEUMONIA TELLS US THIS IS ABOVE THE MINOR FISSURE AND HAS TO BE IN THE RIGHT UPPER LOBE.

48
PERFUSION VENTILATION HERE WE SEE A DEFECT ON THE PERFUSION SCAN WITH A NORMAL VENTILATION SCAN OF THE SAME AREA. THIS IS SUPPORTIVE OF A PULMONARY EMBOLUS BLOCKING BLOOD FLOW DISTALLY IN THE RT LUNG. THIS HAS NO EFFECT ON THE VENTILATION PORTION OF THE SCAN

49
49 In a normal chest radiograph, the visible interstitium is the branching pulmonary vessels The branching disappears peripherally because they are beyond resolution of the xray

50
50 Interstitial Disease

51
51 Hazy or ill defined interstitial lung disease usually indicates acute disease Sharp, well defined and distorted interstitial lung disease usually indicates chronic disease Interstital dz appears as linear, nodular, or reticular (net-like) Interstitial Disease
 Interstitial Disease")
52
52 Interstitial pattern of lung disease

53
53154 slides Interstitial Disease: Pulmonary Fibrosis 53

54
54 Interstitial Disease Reticular=net-like Nodular Reticulonodular: Combination of the two patterns

55
55154 slides Reticular Pattern 55

56
56154 slides Miliary Nodular Pattern: Miliary 56

57
57 Pulmonary Edema Pleural Effusions/Cardiomegaly Vascular Redistribution / Enlargement Interstitial Changes Indistinct pulmonary vasculature Kerly lines Fissural Thickening Bronchial Cuffing Alveolar Edema Perihilar air space disease “Batwing” or “butterfly” appearance

58
58154 slides Pulmonary Edema Minor fissure 58

59
59154 slides Alveolar Edema Alveolar Pulmonary Edema 59

60
60 Emphysema (imaging findings) bilaterally flat, depressed hemidiaphragm lung overinflation increased pulmonary radiolucency increased retrosternal space (>4.5cm) accentuated kyphosis increased intercostal spaces prominent hilar vasculature, decreased peripheral bullae
 bilaterally flat, depressed hemidiaphragm lung overinflation increased pulmonary radiolucency increased retrosternal space (>4.5cm) accentuated kyphosis increased intercostal spaces prominent hilar vasculature, decreased peripheral bullae")
61
61 emphysema normal

62
62 Emphysema

63
63 Bullous emphysema

64
64154 slides Enlarged Retrosternal Air Space Flattened Diaphragms Bullous Emphysema 64

65
ATELECTASIS

66
Atelectasis

67
Left lower lobe collapse Further investigations?

68
68154 slides Solitary Pulmonary Nodule: What Would You Do Next? 1) Compare with Any Available Previous 2) Computed Tomography 68 Pulmonary Nodule
 Compare with Any Available Previous 2) Computed Tomography 68 Pulmonary Nodule.")
69
69154 slides Multiple Nodules: Diagnosis?Metastases 69

70
70 Pleura and Diaphragm Pleural Effusion Lateral decubitus>Lateral>PA in sensitivity Pneumothorax Upright Deep sulcus sign in supine

71
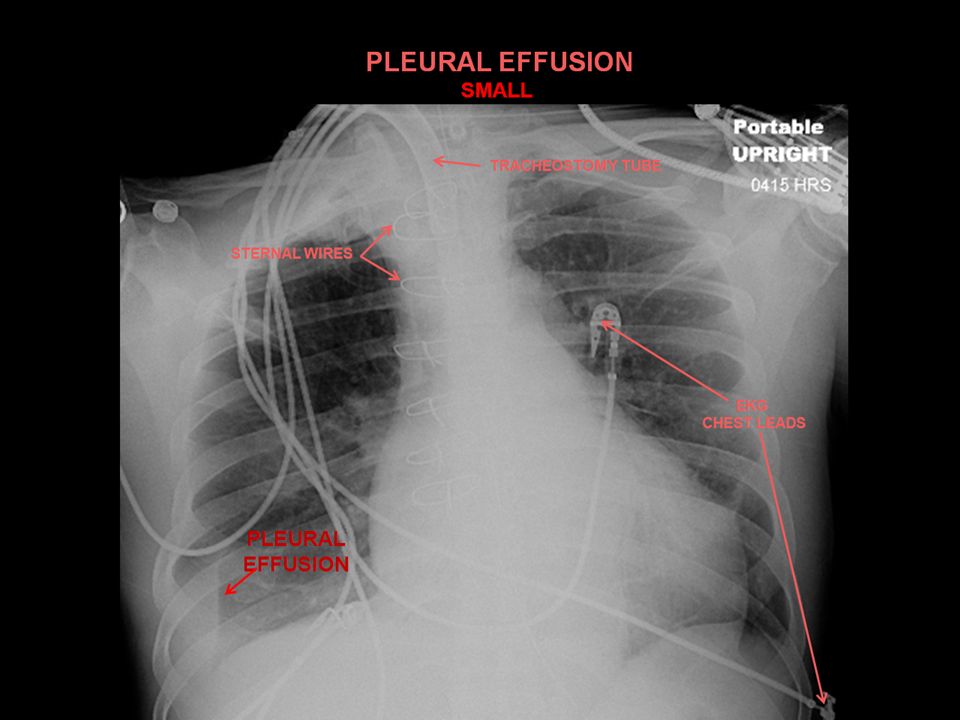
71154 slides Small Pleural Effusion 71

72
72154 slides Small Pleural Effusion Normal: Sharp Angles Blunted posterior costophrenic sulcus 72

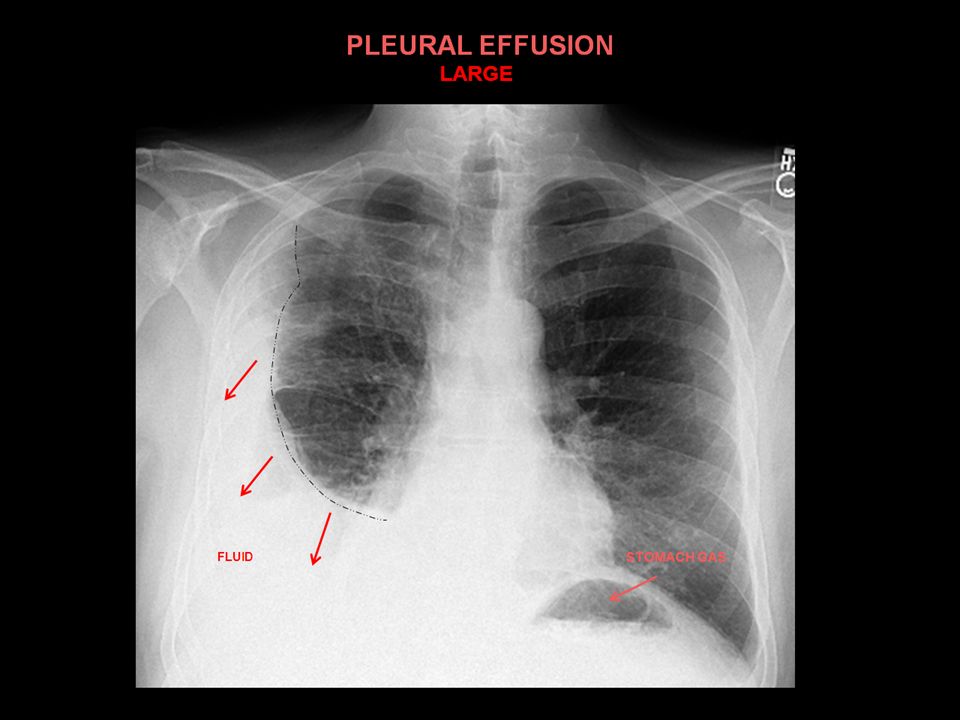
75
75154 slides Large Pleural Effusion 75

76
76

77
77154 slides Inspiration Expiration 77

78
78154 slides Collapsed Right Lung Tension Pneumothorax: Requires chest tube Tracheal Deviation What would you do with this patient? 78

79
HEMOTHORAX

80
In the previous image: OUR PATIENT HERE WAS UNFORTUNATELY ON THE RECEIVING END OF A BULLET HERE THERE IS ASYMMETRY AS WELL BUT THE RT. SIDE IS MORE DENSE (WHITER) THAN THE LEFT. THERE IS A BAND OF FLUID/ SOFT TISSUE DENSITY ALONG THE RT. CHEST WALL. THIS IS FLUID IN THE PLEURAL SPACE ( BLOOD) AND FILLS A SIMILAR SPACE COMPARED WITH OUR SUBCLAVIAN MISADVENTURE. IT IS OF SOFT TISSUE DENSITY AS OPPOSED TO AIR DENSITY. BLOOD AS WELL AS ALL FLUID IS THE SAME DENSITY ON X-RAY. THIS IS NOT A SIMPLE PLEURAL EFFUSION BUT CALLED A HEMOTHORAX.
 THAN THE LEFT. THERE IS A BAND OF FLUID/ SOFT TISSUE DENSITY ALONG THE RT. CHEST WALL. THIS IS FLUID IN THE PLEURAL SPACE ( BLOOD) AND FILLS A SIMILAR SPACE COMPARED WITH OUR SUBCLAVIAN MISADVENTURE. IT IS OF SOFT TISSUE DENSITY AS OPPOSED TO AIR DENSITY. BLOOD AS WELL AS ALL FLUID IS THE SAME DENSITY ON X-RAY. THIS IS NOT A SIMPLE PLEURAL EFFUSION BUT CALLED A HEMOTHORAX..")
81
81 Classification of Mediastinum Anatomic Superior: above sternal angle Anterior Middle: heart and pericardium Posterior There are radiographic classification e.g. Felson’s

82
82 Anterior Mediastinal Mass The 4 T’s Thyroid Thymus (Thymoma) Teratoma Terrible Lymphoma (Tumour)
 Teratoma Terrible Lymphoma (Tumour)")
83
83154 slides Thyroid Goiter Most common superior mediastinal mass extending to thoracic inlet Note Tracheal Deviation 83

84
84154 slides Benign thymoma Normal 84

85
85154 slides Lateral CXR shows: mass is anterior NORMAL 85

86
86 Lymphadenopathy Lung Cancer Lymphadenopathy

87
87154 slides Normal Hilar and Mediastinal Lymphadenopathy Diagnosis? 87

88
88154 slides Hilar Lymphadenopathy on lateral Normal 88

Similar presentations











 –Partial.>")













