Download presentation
Presentation is loading. Please wait.

1
CXR in Emergency Department
By : O. Ahmadi, MD. Professor Assistant of Esfahan medical School, Emergency Department of Al-Zahra Hospital

2
Normal CXR

3
Features that are typically examined on a chest X-ray
Every doctor will have a different approach to examining chest X-rays. A commonly used mnemonic for what to look for on a chest X-ray is: It May Prove Quite Right (but) Stop And Be Certain How Lungs Appear
 Stop And Be Certain How Lungs Appear.")
4
I = Identification (name, age, sex, indication for X-ray)
M = Markers (differentiate left from right ) P = Position - the spinous process of T4 should be between the heads of the clavicle (if it isn't the body is rotated)
 P = Position - the spinous process of T4 should be between the heads of the clavicle (if it isn t the body is rotated)")
5
Q = Quality - is the film penetrated properly
Q = Quality - is the film penetrated properly. In a properly penetrated film the vertebral interspaces should be visible behind the central (cardiac) shadow R = Respiration - chest X-rays are typically done with full inspiration (but)
 shadow. R = Respiration - chest X-rays are typically done with full inspiration. (but)")
6
S = Soft tissue - look for subcutaneous emphysema (suggestive of trauma), soft tissue swelling
A = Abdomen - look for free abdominal air (suggests penetrating trauma, peritonitis, or recent surgery) B = Bone - look for fractures (these tend to be at the lateral aspects because of the mechanics
 B = Bone - look for fractures (these tend to be at the lateral aspects because of the mechanics.")
7
C = Central shadow (cardiac silhouette) - greater than 50% of lateral distance in frontal view at the diaphragm suggests cardiac enlargement (usually secondary to heart failure) or a pericardial effusion . A widened mediastinum may suggest aortic dissection

8
H = Hila (of the lungs) - can be affected in lung disease, malignant processes and infection (hilar lymphadenopathy). L = Lungs - for consolidation, interstitial lung disease (reticular, nodular or reticulonodular), honeycombing, miliary pattern, granulomas, lung masses A = Absent structures/Apices of the lung (for pneumothorax)
, honeycombing, miliary pattern, granulomas, lung masses. A = Absent structures/Apices of the lung (for pneumothorax)")
9
Technique tips Sometimes the film may have been taken at an angle
The silhouette sign To identify PA or AP film

10
Effect of over- and underexposure on a chest x-ray. Overexposure (A)
Underexposure (B

11
Nipple shadows. midclavicular line over the lower half of both the right and the left lung (arrows). These should be bilateral
. These should be bilateral.")
12
Effect of position on the chest x-ray

13
Normal Anatomy and Variants

15
Situs inversus. The heart, stomach, and liver are all in reversed positions. Before you make this diagnosis, make sure that the technician has placed the right and left markers correctly.

16
Lung volume can be estimated by observing the point where a posterior rib crosses the dome of the diaphragm. Normal for PA film - 9th or 10th posterior rib. This point is at the 8th or 9th ribs in older patients

17
Free gas under the diaphragm indicates bowel perforation
Free gas under the diaphragm indicates bowel perforation. Note that this sign is only likely to be seen if an erect film is taken

18
Pericardial effusion

19
The right lung has 3 lobes: Right upper lobe, middle and lower lobe.
The left lung has 2 lobes: Left upper lobe (the lingula anatomically corresponds to the middle lobe on the right) and lower lobe
 and lower lobe.")
21
Pulmonary infiltrates
Atelectasis/collapse Loss of lung volume Anatomy shifts towards atelectasis Linear, smooth, wedge-shaped Apex of opacity starts at hilum Consolidation Normal lung volume No anatomical shift Consolidation Air bronchograms can occur in both.

23
Pneumonia Severe pneumonia is classically manifested by airspace disease and consolidation (alveoli and bronchioles that are completely filled Air bronchograms may occur (air in larger bronchi, outlined by consolidated surrounding parenchyma) Other radiographic features include: interstitial infiltrates that may be the only manifestation or may coexist with consolidative changes. ± associated parapneumonic effusion
 Other radiographic features include: interstitial infiltrates that may be the only manifestation or may coexist with consolidative changes. ± associated parapneumonic effusion.")
24
Air Bronchogram

25
Pneumonia

26
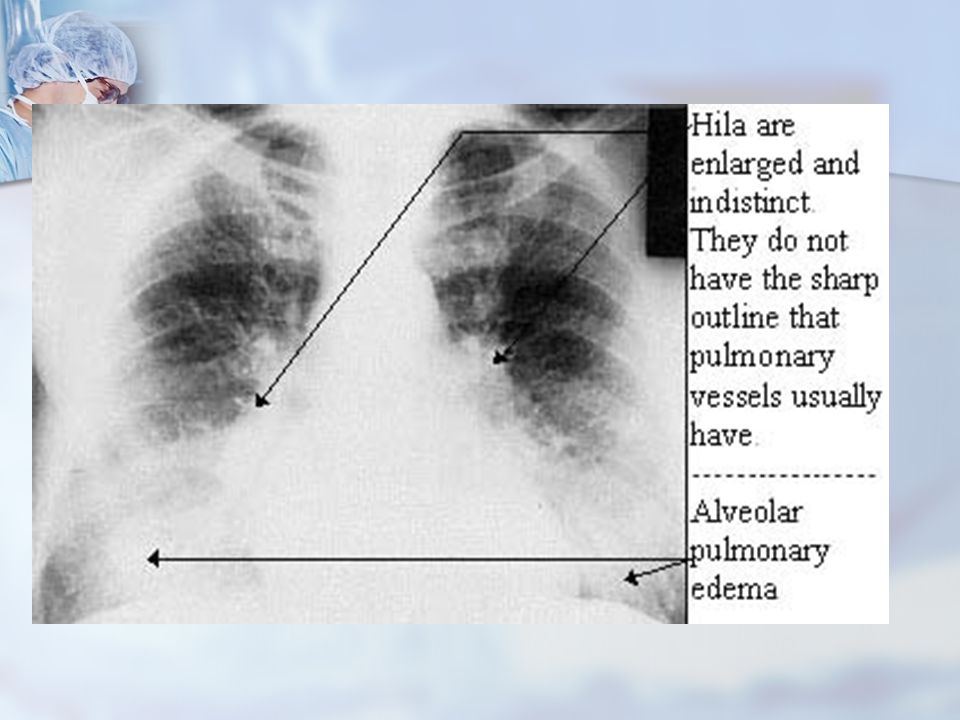
Pulmonary edema A hallmark of pulmonary edema is it’s ability to clear rapidly – within hours

29
Pneumothorax

31
Hemothorax

32
Contusion

33
Aortic Dissection

34
Pulmonary Embolism CXR Findings: Normal Atelectasis
Increased size pulmonary artery, azygos, SVC Elevated hemidiaphragm Edema away from site of PE Westermark's sign Oligemia of lung beyond occluded vessel May be localized, unilateral, or widespread Usually associated with increased size of pulmonary artery (Fleischner's sign) Hampton's Hump Associated with PE with infarction Triangular or rounded density at periphery or pleural based Best seen hours after event
 Hampton s Hump. Associated with PE with infarction. Triangular or rounded density at periphery or pleural based. Best seen hours after event.")
36
What`s wrong with this x ray?

Similar presentations












 –Partial.>")




>")







