Download presentation
Presentation is loading. Please wait.

1
Board Review DH227 Medical Emergencies
Lisa Mayo, RDH, BSDH Concorde Career College

2
Hypertension (HBP) Classifications of BP Levels in Adults Category
Systolic Diastolic Normal <120 And <80 Prehypertension 120 – 139 Or High Blood Pressure Stage 1 Hypertension 140 – 159 Stage 2 Hypertension >160 > 100

3
Hypertensive Emergency
Symptoms – similar to MI (heart attack) or CVA (cerebrovascular accident or stroke)– difficult to determine exact emergency Altered consciousness Visual loss Seizures Nausea/vomiting Eventually coma Sudden increase in BP > 180/110 often as high as 220/140 Dyspnea(labored breathing) Chest pain Dysarthria(difficulty speaking) Weakness 12-12
 or CVA (cerebrovascular accident or stroke)– difficult to determine exact emergency. Altered consciousness. Visual loss. Seizures. Nausea/vomiting. Eventually coma. Sudden increase in BP > 180/110 often as high as 220/140. Dyspnea(labored breathing) Chest pain. Dysarthria(difficulty speaking) Weakness")
4
Hypertensive Emergency
Treatment Treat quickly to reduce BP to prevent further end organ damage like acute MI, aortic dissection or CVA. Treating hypertension secondary Seat patient upright Contact EMS Monitor vital signs Administer O2 4-6L/minute In hospital pt will receive a vasodilator or nitroglycerin. 12-12

5
Hypotension Treatment Position supine with feet raised Assess airway
Administer O2 4-6L/minute Monitor vital signs If no improvement, contact EMS 12-12

6
Shock Condition produced when the cardio-vascular pulmonary system fails to deliver enough oxygenated blood to body tissues to support metabolic needs. Tissues use anaerobic (without air) metabolic processes. Produces acidosis (increased acidity in blood) and harmful toxins.
 metabolic processes. Produces acidosis (increased acidity in blood) and harmful toxins.")
7
Shock Basic positioning Upright Semi upright
Supine and horz with the brain on the same level as the heart If face RED = raise head Face is Pale = raise the tail

8
Shock Stages: 1. Initial 2. Compensatory 3. Progressive 4. Refractory
Types: Hypovolemic Cardiogenic Obstructive Distributive Anaphylactic Septic Neurogenic

9
Syncope(cerebral ischemia)
Sudden, transient loss of consciousness and postural tone with spontaneous recovery. Often caused by loss of cerebral oxygenation and perfusion Often sign of another underlying condition Often associated with a stressful condition Most common med ER in the dental office Most syncopal episodes occur during the administration of local anesthetics.

11
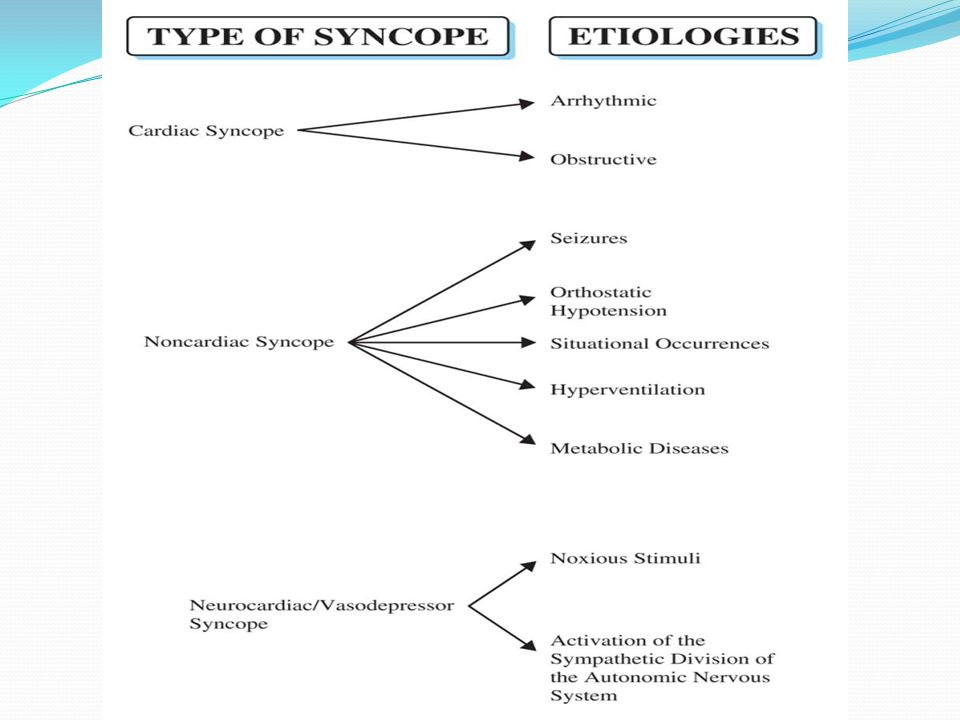
Types of syncope Cardiac: usually from underlying heart disease, common from arrhythmias or obstructions of the heart, potentially fatal, referral to MD Noncardiac: due to seizures, orthostatic hypotension, situation occurrences(coughing, urinating, Valsalva’s maneuver-forced expiratory effort against a closed airway, hyperventilation, metabolic disease(hypoglycemia, hypoxemia: low oxygen in blood) Neurocardiac: most common form encountered by dental professionals, associated with pain, fear, exhaustion, illness, activation of the autonomic nervous system: fight or flight response
 Neurocardiac: most common form encountered by dental professionals, associated with pain, fear, exhaustion, illness, activation of the autonomic nervous system: fight or flight response.")
12
Treatment of Syncope Remove objects from oral cavity
Position supine with feet elevated Open airway Assess circulation Loosen tight clothing Administer oxygen, 4-6L/minute Monitor vital signs Call EMS if symptoms do not change 12-12

13
Treatment of Syncope If unconsciousness persists summon EMS
No longer recommended to use ammonia inhalants due to adverse side effects in some patients. Longer patient in syncope more likely seizure will occur. Recurrence of another syncopal episode is at a higher risk for the first 24 hours following the episode. Once consciousness returns Keep pt in supine position until patient feels well enough to be returned to upright position and pulse returns to normal. 12-12

14
Respiratory Emergencies
Criteria: conscious pt, difficulty breathing, sit pt upright Categories Hyperventilation Asthma COPD

15
Hyperventilation: signs & symptoms
Lightheadedness, dizziness, impaired vision Seizures possible Can cause hypocalcemia: reduction in calcium levels in blood Tetany: caused by low calcium levels, manifests as twitching of muscles or spasms, with sharp flexion of wrist and ankle joints(carpopedal spasms) Numbness of extremities: parasthesia Chvostek’s sign: from hypocalcemia-an abnormal spasm of the facial muscles elicited by light taps on the facial nerve.
 Numbness of extremities: parasthesia. Chvostek’s sign: from hypocalcemia-an abnormal spasm of the facial muscles elicited by light taps on the facial nerve.")
16
Hyperventilation Management
Operator remain calm Place patient in position of their choice: usually upright Loosen tight clothing in neck area Work with patient to control rate of respirations Have pt count to 10 in one breath Breath through pursed lips or nose NO MORE PAPER BAGS: can cause suffocation and cardiac arrest.

17
Hyperventilation treatment
Monitor vitals DO NOT ADMINISTER OXYGEN: can make condition worse. Administer benzodiazepine (Lorazepam 1-2mg IM or Diazepam 2-5mg IM) We do NOT have in clinic No improvement call EMS
 We do NOT have in clinic. No improvement call EMS.")
18
Asthma Airways are hypersensitive to certain triggers known as stimuli. In response to the stimuli the bronchi contract into spasm resulting in dyspnea (difficulty in breathing). Inflammation is the result of the body’s immune response to inhaled allergen. Inflammation leads to airway narrowing and mucus production which leads to coughing and wheezing on expiration and inspiration.
. Inflammation is the result of the body’s immune response to inhaled allergen. Inflammation leads to airway narrowing and mucus production which leads to coughing and wheezing on expiration and inspiration.")
19
Asthma Bronchial inflammation is the result of the body’s immune response to an inhaled allergen. Typical allergens: waste from household insects, grass, pollen, mold, pet epithelial cells Cause body to initiate humoral immune response which produces antibodies Immunoglobulin E (IgE)is the specific antibody for environmental allergens Causes inflammatory response leading to asthma attack symptoms
is the specific antibody for environmental allergens. Causes inflammatory response leading to asthma attack symptoms.")
20
5 types of Asthma Extrinsic Intrinsic Drug-induced Exercise-induced
Infectious

21
Extrinsic Most common 50% of all asthmatics
Inherited allergic predisposition Triggers or stimuli from outside of body Pollen, dust, mold, tobacco smoke Dental office: eugenol, impression materials, resins, latex

22
Intrinsic asthma Second major category
Develops in adults over the age 35, but can be found in children Triggered by psychological and physiological stress – example: dental appointments

23
Drug-induced asthma NSAIDS: nonsteroidal anti-inflammatory drugs like ibuprofen and aspirin. Metabisulfite: a preservative found in some foods or local anesthetics containing epinephrine

24
Exercise induced Begins shortly after start of exercise resulting in severe bronchospasms. Inhalation of cold air may provoke mucosal irritation and airway hypersensitivity. Often found in children and young adults due to increased activity levels.

25
Infectious Viral infections of respiratory tract most common cause.
Frequently seen in children and results in increased airway resistance caused by inflammatory response to the bronchi to infection. Treatment of infection reduces asthma symptoms.

26
Treatment of asthma attack
Prevention of acute episodes in dental setting important goal. Including limiting exposure to known allergens and identified triggers. Patients should bring bronchodilator to appointment and should have ready access. Nitrous oxide not contraindicated, but used with judgment of patient symptoms. Local anesthetics with epinephrine may trigger attack – not recommended.

27
Treatment asthma attack
Stop treatment Position patient upright with arms forward Self-administer own bronchodilator Inhale slowly and exhale through pursed lips If patient does not have own inhaler use inhaler from emergency kit Albuterol recommended – fast acting and long duration (4-6 hours)
")
28
Treatment of Asthma Attack
Position patient upright with arms forward Self-administer own bronchodilator Inhale slowly and exhale through pursed lips If patient does not have own inhaler use inhaler from emergency kit Albuterol recommended – fast acting and long duration (4-6 hours) 1-13
")
29
Resp Emerg: COPD Management Emphysema, bronchitis, chronic asthma
Manage sitting upright and encourage coughing Low flow O2: too much can reduce hypoxic drive May not be able to breathe on own again

30
Cardiac Emergencies Categories Congestive Heart Failure Chest Pain
Angina Angina and MI Angina vs AMI

31
Cardiac Emerg: Congestive Heart Failure
RT heart failure Edema ankles Cyanotic Prominent jugular veins More popular LF heart failure Dyspnea, coughing, orthopnea Congestive heart failure: combo of both, sign will be Pink frothy sputum (saliva and blood mixed) Manage: seated upright and initiate CPR LIFE THREATENING!
 Manage: seated upright and initiate CPR. LIFE THREATENING!")
32
Cardiac Emerg: Chest Pain
Criteria: acute, substernal pain, conscious victim Angina or AMI Management Position comfortable ABC’s Definitive care: hx of angina – admin nitroglycerine 0.3mL if needed up to 3x then call EMS. Admin O % No hx angina: same as w/ angina except use AED if needed. May admin ASA 325mg or 50/50 N2O Monitor pt

33
Nitroglycerine Fairly unstable med Allow pt to admin their own
Various types: sprays, pill, patch Never give to pt with low blood pressure Do not give to pt who has consumed alcohol

34
Angina Chest pain due to angina is one of the more common medical emergencies in the dental office. Angina due to inadequate supply and/or increased demand for oxygen to the myocardium (myocardial ischemia). Clinicians should be aware of the patient’s whose medical hx indicate past incidences of angina. CAD, presenting as angina or AMI, is the leading cause of sudden death in the US.
. Clinicians should be aware of the patient’s whose medical hx indicate past incidences of angina. CAD, presenting as angina or AMI, is the leading cause of sudden death in the US.")
35
Cardiac Emerg: Angina and MI
Symptoms similar Pale, cool skin Chest pain: possible after exertion/meal/stress Substernal pain Levine sign (hand on chest from pain) What is the Difference? MI pain more intense and lasts longer Not relieved by nitroglycerine tablets Diabetics may experience a silent MI: because of neuropathy, may not even feel it
 What is the Difference MI pain more intense and lasts longer. Not relieved by nitroglycerine tablets. Diabetics may experience a silent MI: because of neuropathy, may not even feel it.")
36
Cardiac Emerg: Angina vs AMI
Acute Myocardial Infarction (AMI) May or may not have previous hx of disease Not relieved by nitroglycerine Longer duration
 May or may not have previous hx of disease. Not relieved by nitroglycerine. Longer duration.")
37
Acute Myocardial Infarction (AMI)
Necrosis of a portion of the myocardium due to total or partial occlusion of a coronary artery. Occlusion caused by atherosclerosis, thrombus, or a coronary spasm. May form rapidly or over a period of time. MI can lead to cardiac arrest: when the heart fails to beat. Providing basic life support prior to EMS arriving could save a life. Acute myocardial infarction causes necrosis of a portion of the heart muscle due to total or part occlusion of a coronary artery. The occlusion may be caused by atherosclerosis, a thrombus or spasm. AMI can form rapidly or over a period of time and can lead to cardiac arrest. 1-13

38
Acute Myocardial Infarction (AMI)
Cardiac dysrhythmia may occur after MI and is a high risk for death Dysrhythmia may present as: Bradycardia Ventricular tachycardia – rapid contraction with inadequate ventricular filling Ventricular fibrillation – disorganized, irregular contraction of ventricles Asystole – absence of heart contraction One or 2 hours after onset of symptoms, cardiac dysrhythmia presents the greatest risk for death. More than half of the deaths from an AMI occur outside the hospital setting. So important to know CPR is critical. Dysrhythmia may present as a low heart rate, ventricular tachycardia, ventricular fibrillation, or asystole. 1-13

39
Signs and Symptoms of AMI
Classic symptom: chest pain lasting 20 minutes or longer Pressure, tightness, heaviness, burning, squeezing, crushing sensation in middle of chest and/or lower 1/3 of epigastrium Pain may radiate down arms, shoulders, jaw, or back Classic symptom of an AMI is chest pain lasting 20 minutes or more, pressure, tightness, heaviness, burning , squeezing, or crushing sensation in the middle of the chest and lower third of epigastrium. Pain can radiate down the arms, shoulders, jaw or back. 1-13

40
Signs and Symptoms of AMI
Weakness, dyspnea, diaphoresis, irregular pulse, nausea, vomiting, sense of impending doom, clutching chest (Levine Sign) Women show different symptoms: atypical discomfort, upper abdominal pain, shortness of breath, fatigue Diabetics suffer silent MIs. The elderly show signs of shortness of breath, dizziness, pulmonary edema, and/or an altered mental status Signs and symptoms of AMI: patient may feel weakness, have trouble breathing, a cold sweat, irregular pulse, nausea, vomiting, sense of impending doom, Levine sign: clutching of the chest. Women show different symptoms like: atypical discomfort, upper abdominal pain, shortness of breath or fatigue. Diabetics can suffer silent heart attacks and the elderly show signs of shortness of breath, dizziness, pulmonary edema and an altered mental status. Table 10.3 in book shows signs and symptoms of a MI. 1-13
 Women show different symptoms: atypical discomfort, upper abdominal pain, shortness of breath, fatigue. Diabetics suffer silent MIs. The elderly show signs of shortness of breath, dizziness, pulmonary edema, and/or an altered mental status. Signs and symptoms of AMI: patient may feel weakness, have trouble breathing, a cold sweat, irregular pulse, nausea, vomiting, sense of impending doom, Levine sign: clutching of the chest. Women show different symptoms like: atypical discomfort, upper abdominal pain, shortness of breath or fatigue. Diabetics can suffer silent heart attacks and the elderly show signs of shortness of breath, dizziness, pulmonary edema and an altered mental status. Table 10.3 in book shows signs and symptoms of a MI")
41
Treatment of AMI Recognize signs and symptoms Terminate procedure
If there is a history of angina, follow protocol for angina If no history of angina, contact EMS immediately Position patient comfortably, probably upright or semi-supine Assess ABC’s Clinician should treat chest pain as cardiac related until a cardiac cause can be ruled out. Treatment should stop immediately. If the patient has a history of angina follow protocol for angina. No history of angina then 911 called immediately, position patient where they are comfortable, assess ABCs…. 1-13

42
Treatment of AMI Administer oxygen 4-6L/minute via nasal cannula
Monitor vital signs: taken before giving nitro or immediately after. Administer nitroglycerine from emergency cart – 3 doses over a 15 minute period Do not give nitroglycerine to patients with low blood pressure Nitroglycerin should alleviate pain within 2 to 4 minutes If pain diminishes and then returns, most likely AMI Give oxygen through a nasal cannula, monitor vitals, administer nitroglycerine: 3 doses over a 15 minute period. If the pain diminishes but returns most likely the patient is suffering from an AMI. Vitals should be taken before giving nitro or immediately after. Do not give nitro to patients with hypotension 1-13

43
Treatment of AMI Administer aspirin chewed 325 mg. – antithrombotic effect – clinical effect reached in 20 minutes Aspirin should be chewed to enter bloodstream quicker Manage pain to prevent cardiogenic shock with nitrous oxide, if available If cardiac arrest occurs, perform CPR with AED Aspirin has a proven antithrombotic effect and helps in revascularization of the myocardium during an ischemic attack mg given as soon as AMI is recognized. Aspirin should be chewed to get into bloodstream faster. Manage pain to prevent cardiogenic shock with nitrous oxide if it is available. If cardiac arrest occurs, perform CPR with an AED. Using the AED in the first 3-5 minutes of cardiac arrest, patient has the best chance for survival. 1-13

44
Cerebrovascular Accident (CVA)
Interruption of blood flow to the brain Symptoms Severe headache Paralysis Slurred speech, slowed reactions Management Semi-upright ABC’s Lay pt paralyzed side down when possible BLS, EMS No drugs admin. GET THEM TO HOSPITAL!

45
CVA: cerebrovascular accident
AKA stroke, brain attack Abnormal condition of the brain characterized by occlusion or hemorrhage of a blood vessel resulting in lack of oxygen (ischemia) Leads to cell death Using “brain attack” instead of stroke so people will become more familiar with the signs and symptoms Cva: cerebrovascular accident. Also known as a stoke or brain attack. Lack of blood supply to blood vessels results in a loss of oxygen to the brain cells causing cell death. Brain attack used instead of stroke so public will become familiar with CVA signs and symptoms. Reducing deaths and disabilities from CVA 12-12
 Leads to cell death. Using brain attack instead of stroke so people will become more familiar with the signs and symptoms. Cva: cerebrovascular accident. Also known as a stoke or brain attack. Lack of blood supply to blood vessels results in a loss of oxygen to the brain cells causing cell death. Brain attack used instead of stroke so public will become familiar with CVA signs and symptoms. Reducing deaths and disabilities from CVA")
46
CVA Second leading cause of death world wide – 4.6 million annually
United States’ third leading cause of death and disability – 700,000 cases per year – 100,000 recurrent strokes per year Stroke is the 2nd cause of death world wide, 3th cause of death in US 12-12

47
CVA: Treatment Primary goal in CVA treatment is to minimize the cognitive and physical limitations associated with the CVA Contact EMS immediately Position semi-supine Basic life support – check airway, breathing, and circulation Administer O2 4-6L/min if patient is having dyspnea (shortness of breath) or shows signs of hypoxia (body showing signs of lack of oxygen) Test glucose levels to rule out hypoglycemia Primary goal is to minimize the cognitive and physical limitations associated with the stoke. Call 911, provide CPR, give oxygen, test glucose levels to rule out hypoglycemia or low blood sugar. 12-12
 or shows signs of hypoxia (body showing signs of lack of oxygen) Test glucose levels to rule out hypoglycemia. Primary goal is to minimize the cognitive and physical limitations associated with the stoke. Call 911, provide CPR, give oxygen, test glucose levels to rule out hypoglycemia or low blood sugar")
48
CVA: Treatment Monitor vital signs Transport to ED as soon as possible
Aspirin for ischemic CVA reduces death and recurrence rates Aspirin for intracranial hemorrhage CVA patients also improved outcomes – however not recommended to be administered by anyone but a healthcare provider in the emergency department Recent studies show aspirin given to patients having an ischemic stoke reduces death and recurrence rates. Aspirin should only be given by a healthcare provider in the emergency department 12-12

49
CVA: Treatment In hospital CT scan to determine etiology
Hemorrhagic – probably surgery Ischemic – < 3 hours onset of symptoms then IV thrombolytic therapy with altaplase (r-tPa) – removes thrombus or embolus to restore blood flow Ineffective after 3 hours Contraindicated for hemorrhagic CVA because it can lead to further brain bleeding. Hemorrhagic stroke victims will most likely require surgery. Ischemic stoke victims can be given altaplase or r-tPA that can remove the thrombus or embolus to restore the blood flow to the brain. Only effective if med given 3 hours after stroke. 12-12
 – removes thrombus or embolus to restore blood flow. Ineffective after 3 hours. Contraindicated for hemorrhagic CVA because it can lead to further brain bleeding. Hemorrhagic stroke victims will most likely require surgery. Ischemic stoke victims can be given altaplase or r-tPA that can remove the thrombus or embolus to restore the blood flow to the brain. Only effective if med given 3 hours after stroke")
50
New info about strokes New evidence that there is a relationship between early tooth loss and both ischemic and hemorrhagic CVA. Theory is that the relationship between the microorganisms that cause periodontal disease, a chronic oral infection, producing more inflammatory markers and clotting factors, leading to an increase in platelet aggregation, thus contributing to atherosclerosis and thrombi formation. Another theory states that diseases that cause caries and perio disease are linked with CVA due to the fact that they share some common lifestyle factors.

51
Diabetes Millitus Metabolic disorder characterized by hyperglycemia
Etiology: reduction or absence of production of insulin by beta cells of pancreas or defect of insulin receptors Insulin aids in conversion of sugar and starches to a form transported to cells and used for energy

52
Diabetes 3 types Type 1 (formerly IDDM or Juvenile)
Type 2 (formerly NIDDM or adult onset) Gestational 4th category pre-diabetes or impaired glucose tolerance
 Gestational. 4th category pre-diabetes or impaired glucose tolerance.")
53
Type 1 Absolute lack of insulin
Pancreatic beta cells within Islets of Langerhans destroyed due to immune dysfunction In Islets of Langerhans: alpha cells secrete glucagon-raising blood glucose; beta cells secrete insulin lowering blood glucose. Dependent on supplemental insulin for survival 5-10% of all diabetics

54
Type 2 This type of diabetes is increasing comprising 90-95% of all diabetics due to: Increase in life span Sedentary lifestyle Poor diet and exercise of adolescents Pancreas unable to produce sufficient insulin or the body is not able to use the insulin that is produced

55
Gestational diabetes Glucose intolerance with initial onset during pregnancy Usually disappears after pregnancy, but may return years later Etiology: enzyme in placenta and destruction of insulin by placenta causes the development of gestational diabetes. If untreated infant can have fetal macrosomia (big baby syndrome), hypoglycemia, hypocalcemia, or hyperbilirubinemia( too much bilirubin in infants blood and the newborn’s liver can not process the bilirubin causing jaundice. Bilirubin is produced in the liver, when the liver breaks down red blood cells
, hypoglycemia, hypocalcemia, or hyperbilirubinemia( too much bilirubin in infants blood and the newborn’s liver can not process the bilirubin causing jaundice. Bilirubin is produced in the liver, when the liver breaks down red blood cells.")
56
Role of Dental Professional
Questions to ask all diabetic patients Do you monitor glucose levels? If so, how often? What were your most recent glucose levels? How are you feeling? Do you take medication and if so, did you take it today? Before treating a diabetic patient, the hygienist should ask the patient questions like: 1-13

57
Role of Dental Professional
Questions to ask all diabetic patients Have you eaten today? If so, when? Are you having problems with your eyes, feet, legs? Do you see your physician regularly? Do you see an eye doctor yearly? Do you know your average hemoglobin value? 1-13

58
Role of Dental Professional
Strategies to implement: Schedule appointments in early to mid-morning Keep appointments short Instruct patients to continue normal dietary intake prior to appointment Check patient’s blood glucose level prior to any invasive procedure or if patient complains of not feeling well When scheduling and treating diabetic patients, make the appointments in the early to mid morning hours. Clinicians should keep the appointment short and remind the patient to continue normal eating habits prior to appointments. If possible, check the patient’s blood glucose level prior to any invasive procedure or if the patient complains of not feeling well. 1-13

59
Role of Dental Professional
Strategies to implement: Frequent recall examinations and prophylaxis Use of topical fluoride: Prevident 5000 paste or gel, Gelkam Recommending saliva substitutes: Biotene or Oral Balance Diabetic patients should be on a frequent recall schedule. The patient should be treated with topical fluoride and dry mouth aids. 1-13

60
Diabetic Medical Emergencies
Many – 4 major Diabetic retinopathy Diabetic neuropathy Diabetic nephropathy Oral Manifestations There are 3 medical emergencies a diabetic patient may suffer in a dental office: sever hyperglycemia or diabetic ketoacidosis, hyperosmolar hyperglycemic nonketotic syndrome and hypoglycemia. 1-13

61
Retinopathy Common sequela (resulting from) diabetes
Leading cause of blindness age 20 – 74 Mild form – increased vascular permeability Moderate form – vascular closure Severe form – growth of new blood vessels on retina and posterior surface of vitreous(layer of collagen) Macular edema or a retinal thickening from leaky blood vessels can develop at all stages of retinopathy Prevention: early screening for diabetes and glucose control.
 Macular edema or a retinal thickening from leaky blood vessels can develop at all stages of retinopathy. Prevention: early screening for diabetes and glucose control.")
62
Neuropathy Mild to severe forms of nervous system damage affecting 60-70% of diabetics. Condition not well understood. Common symptoms: pain in the feet and hands, slow digestion, other neurological problems.

63
Macrovascular and Microvascular Complications
Microangiopathic changes where the basement membrane of the capillaries thickens and can lead to the formation of a thrombi, impeding blood flow. Diminished blood flow can increase the risks of a stroke and/or myocardial infarctions. Lack of blood flow to nervous tissues can damage the nerves. Gangrene: loss of blood to a part of the body increasing the risk of losing a limb.

64
Diabetic Nephropathy (kidneys)
Damages small blood vessels in kidneys Impairs ability to filter impurities from blood Require transplant or dialysis to cleanse blood Once occurs 100% morbidity within 10 years

65
Oral Manifestations of Diabetes
Increased incidence of: Delayed wound healing leading to secondary oral and systemic infections Periodontal disease Abscesses Xerostomia (dry mouth) Caries Lichen planus (white lacy streaks on oral mucosa) Candidiasis (yeast infection in the oral cavity)
 Caries. Lichen planus (white lacy streaks on oral mucosa) Candidiasis (yeast infection in the oral cavity)")
66
Monitoring Best method to avoid complications is to maintain optimum glucose levels. Diabetics test blood several times a day Glucose monitor used Lancet – drop of blood Placed on test strip Inserted into a calibrated glucometer which will display the patient’s blood glucose readings.

67
Glucose Readings Normal reading 50 – 150 mg/dL
Less than 50 hypoglycemic Greater than 150 hyperglycemic Adjustment in medication needed or referral to MD

68
Diabetic Medical Emergencies
Diabetic Ketoacidosis (DKA)- severe hyperglycemia Hyperosmolar Hyperglycemic Nonketotic Syndrome (HHNKS) Hypoglycemia
- severe hyperglycemia. Hyperosmolar Hyperglycemic Nonketotic Syndrome (HHNKS) Hypoglycemia.")
69
Diabetic Ketoacidosis (DKA): severe hyperglycemia
Not a common occurrence in dental office Types of patients at risk for DKA Newly diagnosed Type 1 diabetics Patients that are not medicating or eating properly Brittle diabetics(when type 1 diabetics have unstable glucose levels) Patients with infections Alcohol and cocaine
 Patients with infections. Alcohol and cocaine.")
70
Diabetic Ketoacidosis (DKA)
Etiology: insufficient insulin levels in blood to sustain normal fat metabolism- severe hyperglycemia Glucose metabolism insufficient energy source so body metabolizes fatty acids for energy By products of fatty acids are ketones which cause the blood to be more acidic Ketones are one of a number of substances that increase in the blood as a result of faulty carbohydrate metabolism Ketones excreted in urine along with sodium and potassium can cause a severe electrolyte disturbance

71
Diabetic Ketoacidosis (DKA)
Body exhales carbon dioxide in an attempt to reverse acidosis Leads to tachypnea and increased depth of respirations – Kussmaul respirations (air hunger)
")
72
Signs and Symptoms of DKA
Alteration in mental status Ranging from drowsiness to coma Dehydrated – poor skin turgor Skin and mucous membranes warm and dry Increased thirst Muscle weakness, severe fatigue, and difficulty walking

73
Signs and Symptoms of DKA
Nausea and vomiting Blurred vision due to fluid accumulation in lens of eye Tachypnea and Kussmaul breathing Fruity odor on breath Hypotension Tachycardia In children: cerebral edema is a common complications with a high mortality and morbidity rate.

74
Treatment of DKA Determine an accurate blood glucose level
Need to lower blood glucose level with insulin Should only be administered by medical professional to prevent hypoglycemia Contact EMS IV fluids needed to reverse dehydration Monitor vital signs Position patient supine

75
Hyperosmolar Hyperglycemic State
Patient will be hyperglycemic and dehydrated, but not acidotic Usually affects infirm, neglected, institutionalized, or mentally deficient diabetic patients Cannot recognize thirst Uncommon in dental office

76
Severe Hypoglycemia Used to be known as insulin shock
Blood glucose level below 40 – 50 mg/dL (milligram per deciliter) Severe hypoglycemia affects 30% of diabetics Etiology: missed meal, alcohol, increased exercise without adjusting insulin dosage
 Severe hypoglycemia affects 30% of diabetics. Etiology: missed meal, alcohol, increased exercise without adjusting insulin dosage.")
77
Signs and Symptoms of Severe Hypoglycemia
Dizziness Fainting Weakness Headache Intense hunger Cold, clammy skin More likely to occur in dental office than DKA or Hyperosmolar state

78
Signs and Symptoms of Severe Hypoglycemia
Profuse perspiration Irritability or aggressive behavior Confusion Seizure Eventually coma

79
Treatment of Severe Hypoglycemia
Conscious Patient Administer grams of sugar: table sugar, honey, candy, OJ, glucose tablets/paste Secure airway Monitor vital signs Positive response should occur within 10 – 15 minutes

80
Treatment of Severe Hypoglycemia
Unconscious Patient Tx of choice is Glucagon: 1 mg administered subcutaneously, intramuscularly or intravenously. Contact EMS Maintain airway Monitor vital signs

81
Thyroid Hypothyroidism: emergency is Myxedema Coma
Hyperthyroidism: emergency is Thyroid Storm Management Supine w/ legs slightly elevated ABC’s Call EMS Admin IV 5% dextrose if available and O2 Hospital Care Hypo: mass doses of thyroid hormone for days Hyper: mass doses of antithyroid drug propranolol to block andrenergic-medicated effects of thyroid hormones and lg doses of glucocorticosteroids to prevent acute adrenal

82
Thyroid Storm Life threatening Exacerbation of hyperthyroid state
Etiologies: undiagnosed hyperthyroid disease, overzealous treatment of hypothyroidism, discontinuance of medication, trauma, infection, DKA, CVA, stress, toxemia of pregnancy, fright, surgery 10 – 50% fatal A thyroid storm is a life threatening emergency due to an exacerbation of a hyperthyroid state. Causes can be undiagnosed thyroid disease, overtreatment of hypothyroidism, stopping antithyroid meds, trauma, infection, ketoacidosis, stoke, stress, toxemia of pregnancy, fright, and surgery % of thyroid storm cases are fatal. 1-13

83
Signs and Symptoms of Thyroid Storm
Exaggeration of hyperthyroid symptoms Fever: as high as 108 degrees F. Diaphoresis CNS – restlessness, confusion, anxiety, psychosis Pg 212, Table 18.2 Signs and symptoms of a thyroid storm are fever as high as 108 degrees F, diaphoreses, it affects the CNS causing restlessness, confusion, anxiety and psychosis. 1-13

84
Signs and Symptoms of Thyroid Storm
GI symptoms – nausea, vomiting, diarrhea, jaundice Increased systolic BP Widened pulse pressure Arrhythmias Patient may suffer from Gi symptoms like nausea, vomiting, diarrhea, jaundice. Systolic blood pressure is increased, tachycardia, widened pulse pressure, and arrthymias. 1-13

85
Seizures Criteria: unconscious victim, tonic-clonic seizure activitiy
Most critical stage if the postictal phase (once seizure has stopped) Airway management imperative If unconscious: might close off airway Management Prevent injury, NEVER place fingers in mouth ABC’s Low O2 after seizure: EMS needed Key time=5min. If seizure longer= call EMS
 Airway management imperative. If unconscious: might close off airway. Management. Prevent injury, NEVER place fingers in mouth. ABC’s. Low O2 after seizure: EMS needed. Key time=5min. If seizure longer= call EMS.")
86
Seizures See handout for Types

87
Allergy Usual progression Allergic rxns Anaphylaxis
Skin – eyes – nose – GI – Resp - Cardio Allergic rxns Mild to mod usually involves skin, eyes, nose, sometimes resp Anaphylaxis Severe allergic response Involves all systems, esp resp Will lead to cario collapse and death

88
Allergy Management Position comfortable ABC’s
Admin Benadryl 50mg tablets for 2-3 days, 3-4x/day or Benadryl IM Anaphylaxis: admin a pre-loaded epi syringe sublingually 0.1ml for a total of 3 doses every 5min Call EMS, pt will need more then epi

89
Allergy Overdose Elevated vitals, talkativeness, anxiety, headache, dizzy, flushed Slurred speech, blurred vision, ringing in ears, severe-resp difficulty Epi Elevated vitals, anxiety, tremors, throbbing, headache, dizziness, pallor, heart palpitations, resp difficulty

90
Local Anes Overdoes Situations
Unconscious pt Pre-Injenction Stage: hyperventilation or syncope Supine, syncope management, calm pt During Injection: allergy Admin epi if severe Admin benadryl if mild Post-Injection: overdose Manage symptoms and monitor vitals

91
Emergency Drug Kits Epi (Pre-Injectable) Allergic Rxn
Nitroglycerine Chest Pain Oxygen Resp Distress Albuterol Asthma Frosting cake mix Diabetes Benadryl Allergic Rxn Aspirin Heart Issues AED Life Saver!

92
Adrenal Crisis Body severely lacking cortisol 2 reasons:
Individual not yet diagnosed – needs cortisol to maintain carbohydrate and protein metabolism Often happens as this condition mimics other illnesses like gastrointestinal illness or psychiatric disease. Adrenal crisis is a condition when the body is severely lacking cortisol. Adrenal crisis can happen in 2 ways: a person has not been diagnosed with adrenal insufficiency yet and now their body is in severe need of cortisol to maintain normal carbohydrate and protein metabolism and help control the immune system. Often goes unrecognized in its early stages because it mimics other disorders like gastrointestinal illness or psychiatric disease 1-13

93
Adrenal Crisis 2nd reason:
Patient with adrenal insufficiency in a stressful situation and requires additional cortisol Often occurs in individuals on long time steroid therapy and the adrenal cortex atrophies. 2nd reason is when a patient with adrenal insufficiency is put in a stressful situation when the body requires additional cortisol but is unable to produce it. Happens when a patient on long term steroid therapy experiences a reduction in ACTH. With long term steroid use the adrenal cortex will atrophy increasing the need in glucocorticoids. 1-13

94
Signs and Symptoms of Adrenal Crisis
Fatigue Lethargy Muscle weakness Headache Signs and symptoms of adrenal crisis include… 1-13

95
Signs and Symptoms of Adrenal Crisis
Confusion Fever Nausea Vomiting 1-13

96
Signs and Symptoms of Adrenal Crisis
Abdominal pain Hypotension – when coupled with stress can lead to shock and cardiovascular collapse Tachycardia Diaphoresis- profuse sweating Dehydration Hypotension without an appropriate amount of glucocorticords during times of stress can lead to shock and cardiovascular collapse. If hypotension is left untreated, death can result 1-13

97
Treatment of Adrenal Crisis
Contact EMS Stabilize until EMS arrives Maintain airway Monitor vital signs Managing an adrenal crisis requires stabilization of the patient until EMS arrives. Maintain patient’s airway, monitor vitals 1-13

98
Treatment of Adrenal Crisis
Administer O2 if needed IV fluids needed, as well as glucocorticoids which should only be administered by medical professional Therapy will help alleviate cardiac arrhythmias, GI disturbances, hypotension, and electrolyte inbalance If the patient is having trouble breathing give oxygen 2-5 L/min through a nasal cannula. EMS will likely start an IV of sodium chloride fluid to replace fluid volume and correct sodium deficiency. Patient will also need glucocorticoids. Mineral corticoids need to be given to patients with primary adrenal insufficiency not usually needed in the 2nd type. Therapy will help alleviate cardiac arrhythmias, GI disturbances, hypotension, and electrolyte imbalance. Better to over treat than under treat a patient who might be suffering from adrenal crisis. 1-13

Similar presentations



 in the lungs and in the.>")








 Hyperventilation (panic attack)>")






