Download presentation
Presentation is loading. Please wait.

1
Diabetes-Related Emergencies 4-14

2
Case Scenario Your patient, Jeff Johnson, is a 29-year-old male disc jockey in good health. His medical history reveals that he is a controlled Type 1 diabetic who takes insulin daily. He is late for his 8:00 a.m. appointment stating that he did a gig last night and overslept. He had just enough time to administer his medication but did not want to be any later for his dental appointment, so he skipped breakfast. 4-14

3
Case Scenario You begin the intra/extra oral examination before the oral prophylaxis and notice he is salivating profusely. You ask him where he is and his response is confused and irrational. You take his vital signs and find a bounding pulse and shallow respirations. He is conscious. From what emergency do you suspect Jeff is suffering? 4-14

4
Diabetes Mellitus Characterized by elevated levels of blood glucose resulting from an impaired ability to product or use the hormone insulin.** Etiology: reduction or absence of production of insulin by beta cells of pancreas or defect of insulin receptors Insulin aids in conversion of sugar and starches to a form transported to cells and used for energy 4-14

5
Diabetes Mellitus 3 types Type 1 (formerly IDDM or Juvenile) Type 2 (formerly NIDDM or adult onset) Gestational 4 th category pre-diabetes or impaired glucose tolerance Pg 166, table 16.1 4-14
 Type 2 (formerly NIDDM or adult onset) Gestational 4 th category pre-diabetes or impaired glucose tolerance Pg 166, table")
6
Type 1 Diabetes Mellitus Absolute lack of insulin Pancreatic beta cells within Islets of Langerhans destroyed due to immune dysfunction In Islets of Langerhans: alpha cells secrete glucagon-raising blood glucose; beta cells secrete insulin lowering blood glucose. Dependent on supplemental insulin for survival 5-10% of all diabetics 4-14

7
Type 2 Diabetes Mellitus This type of diabetes is increasing comprising 90-95% of all diabetics due to: Increase in life span Sedentary lifestyle Poor diet and exercise of adolescents Pancreas unable to produce sufficient insulin or the body is not able to use the insulin that is produced 4-14

8
Physiology of Diabetes** Cells of the body need insulin to take in glucose. Liver uses insulin to store glucose as glycogen. If glucose and glycogen are not available in the body for energy, the body must break down other materials for fuel/energy. 4-14

9
Gestational Diabetes Mellitus Glucose intolerance with initial onset during pregnancy Usually disappears after pregnancy, but may return years later Etiology: enzyme in placenta and destruction of insulin by placenta causes the development of gestational diabetes. If untreated infant can have fetal macrosomia (big baby syndrome), hypoglycemia, hypocalcemia, or hyperbilirubinemia( too much bilirubin in infants blood and the newborn’s liver can not process the bilirubin causing jaundice. Bilirubin is produced in the liver, when the liver breaks down red blood cells 4-14
, hypoglycemia, hypocalcemia, or hyperbilirubinemia( too much bilirubin in infants blood and the newborn’s liver can not process the bilirubin causing jaundice. Bilirubin is produced in the liver, when the liver breaks down red blood cells")
10
Fetal Macrosomia: big baby syndrome 4-14

11
Diabetes Testing 2 types Fasting Plasma Glucose Test (FPG) 12 – 14 hour fast – blood glucose between 100 – 125: pre-diabetes; blood glucose: > 126 diabetes Oral Glucose Tolerance Test (OGTT) 12 -14 hour fast and then drinking a glucose-rich beverage – 2 hours later blood glucose: 140 – 199 prediabetes; blood glucose: > 200 diabetes 4-14
 12 – 14 hour fast – blood glucose between 100 – 125: pre-diabetes; blood glucose: > 126 diabetes Oral Glucose Tolerance Test (OGTT) hour fast and then drinking a glucose-rich beverage – 2 hours later blood glucose: 140 – 199 prediabetes; blood glucose: > 200 diabetes 4-14")
12
Systemic Complications Many – 4 major Diabetic retinopathy Diabetic neuropathy Diabetic nephropathy Oral Manifestations 4-14

13
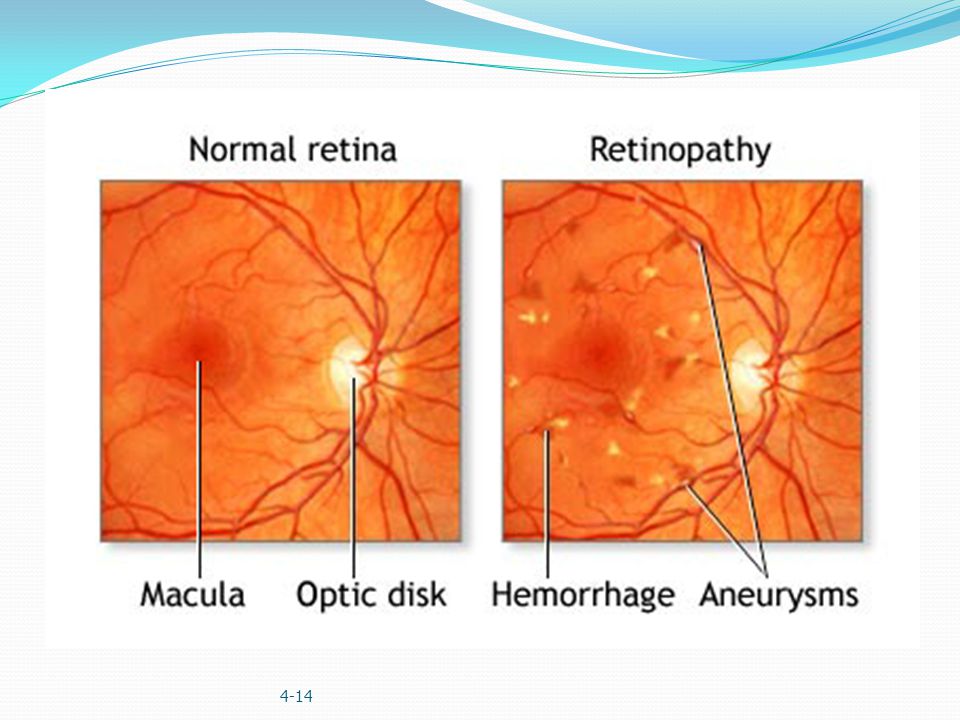
Diabetic Retinopathy (Eyes) Leading cause of blindness age 20 – 74 Mild form – increased vascular permeability Moderate form – vascular closure Severe form – growth of new blood vessels on retina and posterior surface of vitreous(layer of collagen) Macular edema or a retinal thickening from leaky blood vessels can develop at all stages of retinopathy Prevention: early screening for diabetes and glucose control. 4-14
15
Diabetic Neuropathy Mild to severe forms of nervous system damage affecting 60-70% of diabetics. Condition not well understood. Common symptoms: pain in the feet and hands, slow digestion, other neurological problems. 4-14

16
Caused by Diabetic Neuropathy 4-14

17
Macrovascular and Microvascular Complications Microangiopathic changes where the basement membrane of the capillaries thickens and can lead to the formation of a thrombi, impeding blood flow. Diminished blood flow can increase the risks of a stroke and/or myocardial infarctions. Lack of blood flow to nervous tissues can damage the nerves. Gangrene: loss of blood to a part of the body increasing the risk of losing a limb. 4-14

18
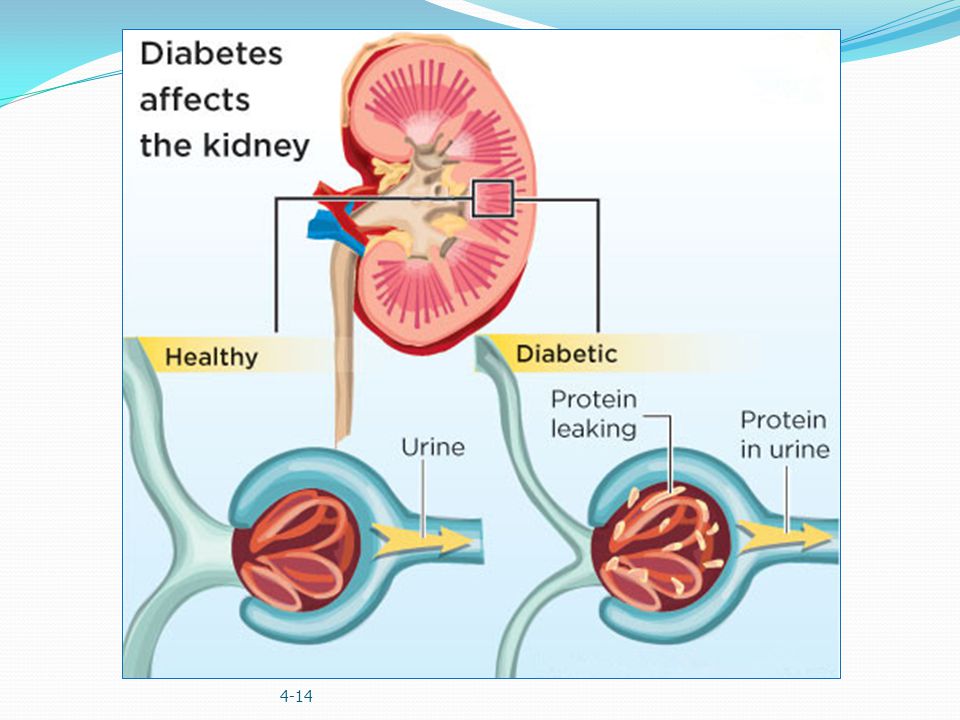
Diabetic Nephropathy (kidneys) Damages small blood vessels in kidneys Impairs ability to filter impurities from blood Require transplant or dialysis to cleanse blood Once occurs 100% morbidity within 10 years 4-14
 Damages small blood vessels in kidneys Impairs ability to filter impurities from blood Require transplant or dialysis to cleanse blood Once occurs 100% morbidity within 10 years 4-14")
20
Oral Manifestations of Diabetes Increased incidence of: Delayed wound healing leading to secondary oral and systemic infections Periodontal disease Abscesses Xerostomia (dry mouth) Caries Lichen planus (white lacy streaks on oral mucosa) Candidiasis (yeast infection in the oral cavity) 4-14
 Caries Lichen planus (white lacy streaks on oral mucosa) Candidiasis (yeast infection in the oral cavity) 4-14")
21
Lichen Planus 4-14

22
Candidiasis 4-14

23
Monitoring Best method to avoid complications is to maintain optimum glucose levels. Diabetics test blood several times a day Glucose monitor used Lancet – drop of blood Placed on test strip Inserted into a calibrated glucometer which will display the patient’s blood glucose readings. 4-14

24
Glucose Readings Normal reading 50 – 150 mg/dL Less than 50 hypoglycemic Greater than 150 hyperglycemic Adjustment in medication needed or referral to MD 4-14

25
Figure 16.1 Glucometer

26
Glucose Testing Another important test HbA1c or glycated hemoglobin test Reveals patient’s “average” blood glucose level over past 3 months Home test methods now available Maintaining optimal levels help reduce the risk of developing diabetic complications like: blindness, kidney disease, nerve damage, stroke and heart failure. 4-14
27
Medications and Treatments for Type I Diabetics Usually some type of insulin: Humalog, Novalog Different types based on time of onset, peak effectiveness, effective duration and maximal duration Need to be refrigerated to lengthen effectiveness 4-14

28
Medications and Treatments for Type II Diabetics Medication prescribed on the basis of cause and severity of condition More common medications: Metformin (Glucophage) Tolbutamide (Orinase) Glyburide (Micronase, DiaBeta, Glynase) 4-14
 Tolbutamide (Orinase) Glyburide (Micronase, DiaBeta, Glynase) 4-14")
29
Advances in Type I Diabetes Treatment Insulin pumps to replace daily injections Compact device with insulin filled syringe that is attached to a subcutaneously inserted catheter Catheter changed every 4-6 days Better glycemic and metabolic control Patient’s with pumps still need to monitor glucose levels 4-14

30
Figure 16.2 12-year-old Type 1 patient with insulin pump

31
Figure 16.3 Insulin pump in place

32
Transplantations in Type I Diabetics Pancreas or pancreatic islet cell transplantation Concerns: need for continuous immunosuppression to prevent rejection of the islet cells or pancreas. 4-14
33
Role of Dental Professional Questions to ask all diabetic patients Do you monitor glucose levels? If so, how often? What were your most recent glucose levels? How are you feeling? Do you take medication and if so, did you take it today? 4-14

34
Role of Dental Professional Questions to ask all diabetic patients Have you eaten today? If so, when? Are you having problems with your eyes, feet, legs? Do you see your physician regularly? Do you see an eye doctor yearly? Do you know your average hemoglobin value? 4-14

35
Role of Dental Professional Strategies to implement: Schedule appointments in early to mid-morning** Keep appointments short** Instruct patients to continue normal dietary intake prior to appointment** Check patient’s blood glucose level prior to any invasive procedure or if patient complains of not feeling well 4-14

36
Role of Dental Professional Strategies to implement: Frequent recall examinations and prophylaxis Use of topical fluoride: Prevident 5000 paste or gel, Gelkam Recommending saliva substitutes: Biotene or Oral Balance 4-14

37
Diabetic Medical Emergencies Diabetic Ketoacidosis (DKA)- severe hyperglycemia Hyperosmolar Hyperglycemic Nonketotic Syndrome (HHNKS) Hypoglycemia 4-14
- severe hyperglycemia Hyperosmolar Hyperglycemic Nonketotic Syndrome (HHNKS) Hypoglycemia 4-14")
38
Diabetic Ketoacidosis (DKA): severe hyperglycemia Not a common occurrence in dental office Types of patients at risk for DKA Newly diagnosed Type 1 diabetics Patients that are not medicating or eating properly Brittle diabetics(when type 1 diabetics have unstable glucose levels) Patients with infections Alcohol and cocaine 4-14
: severe hyperglycemia Not a common occurrence in dental office Types of patients at risk for DKA Newly diagnosed Type 1 diabetics Patients that are not medicating or eating properly Brittle diabetics(when type 1 diabetics have unstable glucose levels) Patients with infections Alcohol and cocaine 4-14")
39
Diabetic Ketoacidosis (DKA) Etiology: insufficient insulin levels in blood to sustain normal fat metabolism- severe hyperglycemia Glucose metabolism insufficient energy source so body metabolizes fatty acids for energy By products of fatty acids are ketones which cause the blood to be more acidic Ketones are one of a number of substances that increase in the blood as a result of faulty carbohydrate metabolism 4-14
 Etiology: insufficient insulin levels in blood to sustain normal fat metabolism- severe hyperglycemia Glucose metabolism insufficient energy source so body metabolizes fatty acids for energy By products of fatty acids are ketones which cause the blood to be more acidic Ketones are one of a number of substances that increase in the blood as a result of faulty carbohydrate metabolism 4-14")
40
Diabetic Ketoacidosis (DKA) Body exhales carbon dioxide in an attempt to reverse acidosis Leads to tachypnea and increased depth of respirations – Kussmaul respirations (air hunger) 4-14
 Body exhales carbon dioxide in an attempt to reverse acidosis Leads to tachypnea and increased depth of respirations – Kussmaul respirations (air hunger) 4-14")
41
Signs and Symptoms of DKA** Polydipsia: excessive thirst Polyuria: excessive urination Polyphagia: excessive hunger Nausea Dry flushed skin Deep and rapid respirations (Kussmaul’s respiration) Weak and rapid pulse “Fruity” breath odor May become unconscious 4-14
 Weak and rapid pulse Fruity breath odor May become unconscious 4-14")
42
Treatment of DKA Stop dental treatment Need to lower blood glucose level with insulin Should only be administered by medical professional to prevent hypoglycemia Contact EMS IV fluids needed to reverse dehydration Monitor vital signs Position patient supine 4-14

43
Hyperosmolar Hyperglycemic State Patient will be hyperglycemic and dehydrated, but not acidotic Usually affects infirm, neglected, institutionalized, or mentally deficient diabetic patients Cannot recognize thirst Uncommon in dental office 4-14

44
Diabetic Emergency: hypoglycemia or hyperinsulinism** Occurs when too much insulin is present and the person’s blood glucose is abnormally low. Below 50 mg/dL May occur when patient increases insulin dosage, omits a meal, vomits or exercises excessively. 4-14

45
Signs and symptoms of hypoglycemia** Sudden onset Altered level of consciousness Confusion Anxiousness Incoherence Uncooperative Pale, moist skin Dizziness Weakness Not be thirsty and have normal breath odor 4-14

46
Treatment of Severe Hypoglycemia Conscious Patient Administer 15-20 grams of sugar: table sugar, honey, candy, OJ, glucose tablets/paste Secure airway Monitor vital signs Positive response should occur within 10 – 15 minutes 4-14

47
Figure 16.4 Oral glucose tablets, paste, sugar packets

48
Treatment of Severe Hypoglycemia Unconscious Patient Tx of choice is Glucagon: 1 mg administered subcutaneously, intramuscularly or intravenously. Contact EMS Maintain airway Monitor vital signs 4-14

49
Figure 16.5 Injectable glucagon

50
Case Resolution: Jeff’s signs and symptoms are those of severe hypoglycemia. Indication of too much insulin and not enough glucose. Jeff was given 6 glucose tablets, which quickly reversed the symptoms of hypoglycemia. He was monitored in office for 30 minutes, given info on managing his diabetes and rescheduled for an appt immediately after lunch.

Similar presentations