Download presentation
Presentation is loading. Please wait.

1
Ski injuries to the upper extremities
Eugene Bailey, MD Department of Family Medicine SUNY Upstate Medical University Toggenberg MA Presentation January 03, 2010 Recently, the increase in snowboarding has increased the “mix” of upper ext injuries occurring at ski slopes. Upper ext injuries are 3x higher among snowboarders than skiers. Wrist and forearm injuries have replaced shoulder injuries as the second most common injury today. These fractures, which often require surgical stabilization or prolonged immobilization by a cast, carry a high risk of permanent impairment. In addition, for the person who suffers such a fracture, the lost wages, time away from school or work and treatment costs are significant. Elbow fractures and/or dislocations do not seem to be increasing in frequency but continue to be a cause for great concern because of the potential loss of distal circulation or sensation. Preserving the function of the hand remains the paramount concern when evaluating and stabilizing upper-extremity injuries.

2
Objectives General Comments Shoulder Injurties Humerus fractures Elbow
ShoulderDislocation Clavicular fracture Scapular fracture Acromioclavicular joint (ACJ) injury Humerus fractures Head Shaft Suprachondylar Elbow Anterior/Posterior dislocation Olecrenon fracture Radial head fracture Wrist Scaphoid fracture Colles fracture Hand/Fingers Skier’s thumb (Gamekeeper’s thumb)
 injury. Humerus fractures. Head. Shaft. Suprachondylar. Elbow. Anterior/Posterior dislocation. Olecrenon fracture. Radial head fracture. Wrist. Scaphoid fracture. Colles fracture. Hand/Fingers. Skier’s thumb (Gamekeeper’s thumb)")
3
Not going to cover Bicipital tendonitis
Medial and Lateral epichondylitis Nursemaid’s elbow Carpel tunnel syndrome Bursitis Finger fractures

4
General Comments Zone of Injury
Despite an obvious fracture or dislocation, there are always surrounding tissues including muscle and ligaments as well as neurovascular structures that must be considered. There may be obvious deformity but bleeding close by.

5
General Comments In the field
ABCs Airway Breathing Circulation Always assess neurovascular status (CMS = circulation, motor and sensory) Control any bleeding Do not move victim until stabilized
 Control any bleeding. Do not move victim until stabilized.")
6
General Comments If possible, always ask the patient to “point with one finger to the area that hurts the most.” Remove jewelry, etc before splinting Patient will self-splint the upper extremity (internal rotation, elbow flexed and adducted to body)
")
7
Remember "Ability and experience are probably the most important factors in determining an individual's likelihood of injury when pursuing an outdoor sport."

8
“ARMS” Appearance and alignment Radial pulse
Motor function and mechanism of injury Sensation

9
Self-splinting

10
Prevention

11
Case Scenario A call comes to you over your radio that a skier is down and appears to have an injury. You grab a toboggan and respond to the scene quickly

12
Upper extremity injuries Snowboarding
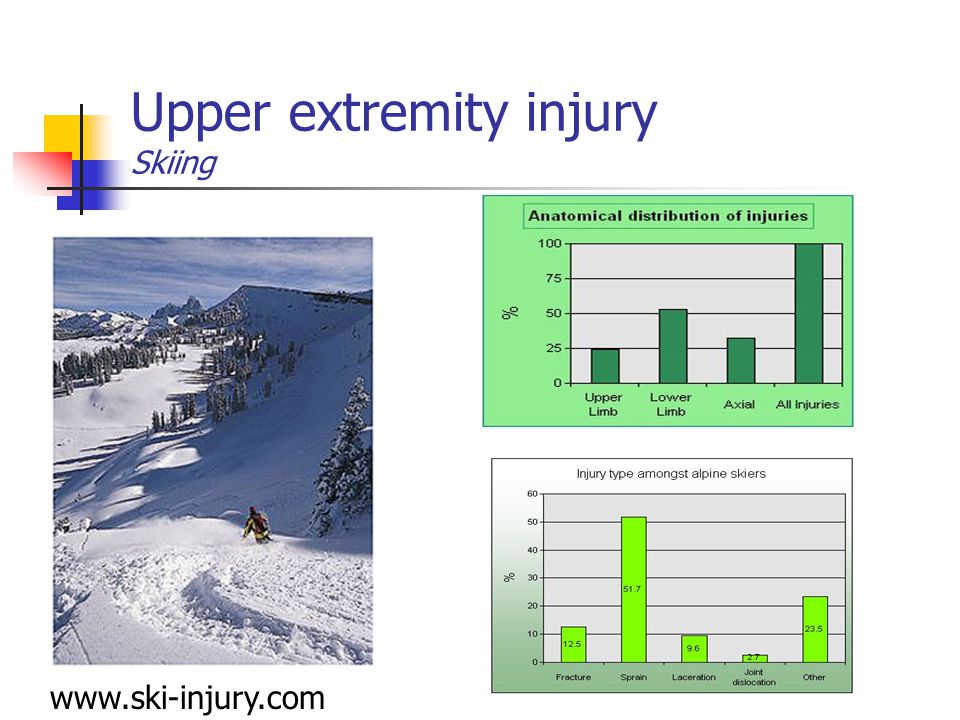
The American Journal of Sports Medicine 28: (2000) © 2000 American Orthopaedic Society for Sports Medicine Upper Extremity Snowboarding Injuries Ten-Year Results from the Colorado Snowboard Injury Survey Jan R. Idzikowski, PA-C*, Peter C. Janes, MD and Paul J. Abbott, MD Vail-Summit Orthopaedics and Sports Medicine, High Country Health Care, PC, Vail, Colorado Address correspondence and reprint requests to Jan R. Idzikowski, PA-C, Vail-Summit Orthopaedics and Sports Medicine, High Country Health Care PC, 181 W. Meadow Drive, Vail, CO 81657 A survey of snowboarding injuries was conducted over 10 seasons (1988 to 1998). A questionnaire evaluating 20 variables was used to collect data from 47 medical facilities near Colorado ski resorts. A total of 7430 snowboarding-related injuries were seen. A control group consisted of 3107 noninjured snowboarders. Most of those injured were 30 years of age or younger; 74% of injuries occurred in men and 26% in women; 39% of injured snowboarders were beginners and 61% were intermediate or experts. Men rode at more advanced levels than women. Injured snowboarders were more likely than noninjured snowboarders to be beginners. There were 3645 (49.06% of total) upper extremity injuries; 56.43% were fractures, 26.78% sprains, and 9.66% dislocations. The most common site of injury was the wrist (21.6% of all snowboarding injuries). Wrist fractures (except to the scaphoid) and sprains were more common in beginners, women, and younger age groups. Intermediate and expert men were more likely to sustain hand, elbow, and shoulder injuries, as well as more severe injuries. Falling was the predominant mechanism of upper extremity injuries. Snowboarders who wore protective wrist guards were half as likely to sustain wrist injuries as those who did not wear guards.
 © 2000 American Orthopaedic Society for Sports Medicine. Upper Extremity Snowboarding Injuries. Ten-Year Results from the Colorado Snowboard Injury Survey. Jan R. Idzikowski, PA-C*, Peter C. Janes, MD and Paul J. Abbott, MD. Vail-Summit Orthopaedics and Sports Medicine, High Country Health Care, PC, Vail, Colorado. Address correspondence and reprint requests to Jan R. Idzikowski, PA-C, Vail-Summit Orthopaedics and Sports Medicine, High Country Health Care PC, 181 W. Meadow Drive, Vail, CO A survey of snowboarding injuries was conducted over 10 seasons (1988 to 1998). A questionnaire evaluating 20 variables was used to collect data from 47 medical facilities near Colorado ski resorts. A total of 7430 snowboarding-related injuries were seen. A control group consisted of 3107 noninjured snowboarders. Most of those injured were 30 years of age or younger; 74% of injuries occurred in men and 26% in women; 39% of injured snowboarders were beginners and 61% were intermediate or experts. Men rode at more advanced levels than women. Injured snowboarders were more likely than noninjured snowboarders to be beginners. There were 3645 (49.06% of total) upper extremity injuries; 56.43% were fractures, 26.78% sprains, and 9.66% dislocations. The most common site of injury was the wrist (21.6% of all snowboarding injuries). Wrist fractures (except to the scaphoid) and sprains were more common in beginners, women, and younger age groups. Intermediate and expert men were more likely to sustain hand, elbow, and shoulder injuries, as well as more severe injuries. Falling was the predominant mechanism of upper extremity injuries. Snowboarders who wore protective wrist guards were half as likely to sustain wrist injuries as those who did not wear guards.")
13
Upper extremity injuries Snowboarding – Val, Colorado (10 year survey)
Most 30 yrs or younger 74% men, 26% women 39% beginners, 61% intermediate or experts Men rode more advanced levels than women Results Injured were more likely to be beginners than non-injured 49.06% upper extremities (56.43% fractures, 26.78% sprains and 9.66% dislocations) Wrist fx (x scaphoid) more common in beginners, women and younger age groups Intermediate and expert were more likely to sustain hand, elbow and shoulder injuries as well as more severe injuries Snowboarders who wear protective wrist guards are ½ as likely to sustain wrist injury The American Journal of Sports Medicine 28: (2000) © 2000 American Orthopaedic Society for Sports Medicine Upper Extremity Snowboarding Injuries Ten-Year Results from the Colorado Snowboard Injury Survey Jan R. Idzikowski, PA-C*, Peter C. Janes, MD and Paul J. Abbott, MD Vail-Summit Orthopaedics and Sports Medicine, High Country Health Care, PC, Vail, Colorado Address correspondence and reprint requests to Jan R. Idzikowski, PA-C, Vail-Summit Orthopaedics and Sports Medicine, High Country Health Care PC, 181 W. Meadow Drive, Vail, CO 81657 A survey of snowboarding injuries was conducted over 10 seasons (1988 to 1998). A questionnaire evaluating 20 variables was used to collect data from 47 medical facilities near Colorado ski resorts. A total of 7430 snowboarding-related injuries were seen. A control group consisted of 3107 noninjured snowboarders. Most of those injured were 30 years of age or younger; 74% of injuries occurred in men and 26% in women; 39% of injured snowboarders were beginners and 61% were intermediate or experts. Men rode at more advanced levels than women. Injured snowboarders were more likely than noninjured snowboarders to be beginners. There were 3645 (49.06% of total) upper extremity injuries; 56.43% were fractures, 26.78% sprains, and 9.66% dislocations. The most common site of injury was the wrist (21.6% of all snowboarding injuries). Wrist fractures (except to the scaphoid) and sprains were more common in beginners, women, and younger age groups. Intermediate and expert men were more likely to sustain hand, elbow, and shoulder injuries, as well as more severe injuries. Falling was the predominant mechanism of upper extremity injuries. Snowboarders who wore protective wrist guards were half as likely to sustain wrist injuries as those who did not wear guards. Idzikowski, et al. AJSM 2000;28:
 Wrist fx (x scaphoid) more common in beginners, women and younger age groups. Intermediate and expert were more likely to sustain hand, elbow and shoulder injuries as well as more severe injuries. Snowboarders who wear protective wrist guards are ½ as likely to sustain wrist injury. The American Journal of Sports Medicine 28: (2000) © 2000 American Orthopaedic Society for Sports Medicine. Upper Extremity Snowboarding Injuries. Ten-Year Results from the Colorado Snowboard Injury Survey. Jan R. Idzikowski, PA-C*, Peter C. Janes, MD and Paul J. Abbott, MD. Vail-Summit Orthopaedics and Sports Medicine, High Country Health Care, PC, Vail, Colorado. Address correspondence and reprint requests to Jan R. Idzikowski, PA-C, Vail-Summit Orthopaedics and Sports Medicine, High Country Health Care PC, 181 W. Meadow Drive, Vail, CO A survey of snowboarding injuries was conducted over 10 seasons (1988 to 1998). A questionnaire evaluating 20 variables was used to collect data from 47 medical facilities near Colorado ski resorts. A total of 7430 snowboarding-related injuries were seen. A control group consisted of 3107 noninjured snowboarders. Most of those injured were 30 years of age or younger; 74% of injuries occurred in men and 26% in women; 39% of injured snowboarders were beginners and 61% were intermediate or experts. Men rode at more advanced levels than women. Injured snowboarders were more likely than noninjured snowboarders to be beginners. There were 3645 (49.06% of total) upper extremity injuries; 56.43% were fractures, 26.78% sprains, and 9.66% dislocations. The most common site of injury was the wrist (21.6% of all snowboarding injuries). Wrist fractures (except to the scaphoid) and sprains were more common in beginners, women, and younger age groups. Intermediate and expert men were more likely to sustain hand, elbow, and shoulder injuries, as well as more severe injuries. Falling was the predominant mechanism of upper extremity injuries. Snowboarders who wore protective wrist guards were half as likely to sustain wrist injuries as those who did not wear guards. Idzikowski, et al. AJSM 2000;28:")
14
Upper extremity injury Skiing
15
Upper extremity injury Skiboard

16
Shoulder Injuries

17
Shoulder dislocation MOI: Majority are anterior dislocation (97%)
Fall onto an outstretched hand c the momentum of the fall twisting the body around wretching the shoulder out of joint Posterior blow to shoulder Majority are anterior dislocation (97%)
")
18
Shoulder dislocation The diagnosis of a dislocated shoulder is usually clinical Walk slowly holding affected arm, careful not to move it. Usually arm is away from body. Loss of smooth contour of the shoulder anatomy The diagnosis of a dislocated shoulder is usually clinical - you can often tell one as soon as they walk in the clinic door! Those with dislocated shoulders tend to walk slowly, being extremely careful to hold the affected arm to prevent any (extremely painful) movement in the arm. Their stance is often such that they tend to lean towards the affected side. On examination, the affected shoulder joint has lost its normal smooth curved shape and you can often feel a gap where the humeral head used to sit in the joint
 movement in the arm. Their stance is often such that they tend to lean towards the affected side. On examination, the affected shoulder joint has lost its normal smooth curved shape and you can often feel a gap where the humeral head used to sit in the joint.")
19
Radiograph of Anterior shoulder dislocation

20
Shoulder dislocation X-rays do not have to be obtained before treatment There are numerous techniques for reduction Traction Leverage Theodor Kocher, a famous nineteenth century surgeon whose main interest was thyroid surgery, described possibly the best known leverage technique.26 Interestingly, although he described his method of manipulation in 1870, a wall painting in the Egyptian tomb of Ipuy, dating back to 1200BC, looks deceptively similar, resulting in speculation that "Kocher's method" is actually 3000 years old!27 With this technique, the affected arm is flexed at the elbow and pressed (adducted) against the side of the body. The forearm is rotated outwards until resistance is felt. The externally rotated upper arm is then lifted in a sagittal plane as far as possible forwards and finally, internal rotation is performed (Figure 4). No traction was involved in the original description.28 Kocher’s technique
 against the side of the body. The forearm is rotated outwards until resistance is felt. The externally rotated upper arm is then lifted in a sagittal plane as far as possible forwards and finally, internal rotation is performed (Figure 4). No traction was involved in the original description.28. Kocher’s technique.")
21
Shoulder dislocation Immobilize the injured joint Blanket roll Sling
Sling and swath Ice

24
Clavicular fracture Most commonly fractured bone in the entire body!
MOI: Transmission of force up the arm Fall onto shoulder Direct blow to the clavicle

25
Clavicular fracture presents with:
pain to direct palpation over the clavicle or with movement of the arm or neck may be deformity of the bone with swelling and ecchymosis. (“tenting” over fracture site) Arm held to the side Palpate for crepitus
 Arm held to the side. Palpate for crepitus.")
26
Clavicular Fracture Middle third - 80% Proximal third - 5%
Distal third classification Middle third % Proximal third - 5% Distal third %

27
Clavicular Fracture Simple sling Figure-of-eight Ice
Do not apply if causes patient discomfort Do not apply for distal fractures Ice Anderson, et.al., Acta Orthop Scand 1987;58:71-74 Stanley, et. al., Injury 1988;19:

28
Scapular Fracture MOI: Forceful, direct blow to the back
Very rare because well protected by muscles Always assess for spinal injury or breathing difficulty Sling and swathe

29
Acromio-clavicular joint (ACJ) injury
 injury")
30
ACJ Injury MOI: Injury to the ligament causes
Falling directly onto the adducted shoulder Injury to the ligament causes Tear (subluxation) Dislocation
 Dislocation.")
31
ACJ Injury Grade Grade Grade 3………

32
ACJ Injury Presentation:
Type 1/Grade 1 – local tenderness without deformity Type 2,3,4,5,6/ Grade 2,3 – local tenderness with deformity

33
ACJ Injury Simple sling! Collar and cuff Ice

34
Humerus Injuries

35
Bony Anatomy: Humerus Distally – 2 condyles forming articular surfaces of trochlea and capitellum Proximally – neck and head articulate with glenoid fossa of scapula

36
Humeral Fractures MOI Head - Direct trauma to the humerus from collision with an object or fall directly onto the bone Shaft – bent forces like breaking a stick (shear or torsion) Supraconylar – upper transmission of force on outstretched hand
 Supraconylar – upper transmission of force on outstretched hand.")
37
Humeral Head fracture Diagnosis
Upper humeral fractures usually involve the surgical neck of the bone extracapsular low incidence of avascular necrosis (AVN) Anatomical Neck intracapsular higher incidence of AVN High index of suspicion – consider MOI or elderly Upper fragment is abducted and externally rotated by muscles inserting into greater tubercle and lower fragment is adducted and internally rotated by internal rotators CMS evaluation – arterial occlusion Careful radiologic evaluation is necessary
 Anatomical Neck. intracapsular. higher incidence of AVN. High index of suspicion – consider MOI or elderly. Upper fragment is abducted and externally rotated by muscles inserting into greater tubercle and lower fragment is adducted and internally rotated by internal rotators. CMS evaluation – arterial occlusion. Careful radiologic evaluation is necessary.")
38
Humeral Head Fractures NEER Classification
Stable or unstable classification (compression fxs tend to be stable, shear injuries tend to be unstable) Axillary view is essential in that it best depicts displacement and angulation. Displaced = >10mm and/or angulation > 45 deg One part fractures are <1cm displaced and < 45 deg angulated NEER classification first described in 1970, then simplified in 1975. Developed from the retrospective review of 300 fractures. Requirements to classify fractures: Adequate radiographs (= Trauma series +/- CT scans) Knowledge of the pathology & deforming forces Segment Angulation of 45deg. Segment Displacement of 1cm Reliability of Neer classification: 3 studies have shown poor inter & intraobserver reliability: Kristiansen B, Andersen UL, Olsen CA, Varmarken JE. Skeletal Radiol. 1988;17(6): did not use full trauma series; used a condensed Neer classification; intra-observer reliability was not assessed. Sidor ML, Zuckerman JD, Lyon T, Koval K, Cuomo F, Schoenberg N. J Bone Joint Surg Am Dec;75(12): demonstrated that experience improves reliability. Siebenrock KA, Gerber C. J Bone Joint Surg Am Dec;75(12): * *Velpeau view if cannot abduct arm
 Axillary view is essential in that it best depicts displacement and angulation. Displaced = >10mm and/or angulation > 45 deg. One part fractures are <1cm displaced and < 45 deg angulated. NEER classification. first described in 1970, then simplified in Developed from the retrospective review of 300 fractures. Requirements to classify fractures: Adequate radiographs (= Trauma series +/- CT scans) Knowledge of the pathology & deforming forces. Segment Angulation of 45deg. Segment Displacement of 1cm. Reliability of Neer classification: 3 studies have shown poor inter & intraobserver reliability: Kristiansen B, Andersen UL, Olsen CA, Varmarken JE. Skeletal Radiol. 1988;17(6): did not use full trauma series; used a condensed Neer classification; intra-observer reliability was not assessed. Sidor ML, Zuckerman JD, Lyon T, Koval K, Cuomo F, Schoenberg N. J Bone Joint Surg Am Dec;75(12): demonstrated that experience improves reliability. Siebenrock KA, Gerber C. J Bone Joint Surg Am Dec;75(12): * *Velpeau view if cannot abduct arm.")
39
Humeral Head Fractures Treatment
One part fractures (no fracture fragments displaced < 1cm or 45 deg) Non-operative immobilization in sling1-2 weeks Early motion started immediately 75% good to excellent results; 10% poor Any other fracture Closed reduction with percutaneous pinning ORIF 2-6 weeks to allow pain free movement One part fractures are when patients can actively move the extremity s pain; passive movement produces minimal pain and no bone movement noted. Generally, immobilization > 2 weeks will lead to stiffness.
 Non-operative immobilization in sling1-2 weeks. Early motion started immediately. 75% good to excellent results; 10% poor. Any other fracture. Closed reduction with percutaneous pinning. ORIF. 2-6 weeks to allow pain free movement. One part fractures are when patients can actively move the extremity s pain; passive movement produces minimal pain and no bone movement noted. Generally, immobilization > 2 weeks will lead to stiffness.")
40
Humeral Fractures Complications
Avascular Necrosis of Humeral Head Especially at risk with 4 part fractures Non-union 3-6 mos after injury Shoulder stiffness with prolonged immobilization Non impact fxs are more likely to non-union.

41
Humeral Shaft Fracture Diagnosis
Fractures of the shaft of the humerus 1-3% of all fractures Up to 18% have radial nn palsey mechanism: - bending force produces transverse frx of the shaft; - torsion force will result in a spiral fracture; - combination of bending and torsion produce oblique frx w/ or w/o a butterfly fragment; - compression forces will frx either proximal or distal ends of humerus; types of humeral shaft frx: - transverse humeral fractures: - distal third frx - short oblique fractures: - displaced frx thru distal shaft are difficult to reduce & are difficult to maintain in reduced position; - these fractures may be associated w/ delayed healing; - long spiral fractures: - spiral, comminuted, and oblique fractures have the advantage of generous fracture surface areas and tend to heal rapidly; - if displaced with a gap which does not close when rotational alignment is restored, there may be muscle interposition; - if left with good alignment, but with a significant gap between the frx frag, these frx go on to atrophic nonunion; Exam - Need to rule out radial nn palsey Acceptable Reduction: (forces displacing the fracture:) - axial malalignment: - upper arm will accommodate deg of anterior angulation & deg of varus; - this amount of angulation would be considered acceptable for patients w/ low to moderate functional demands; - overriding fracture: - bayonet position w/ upto 1 inch of shortening is acceptable; - over-riding displacement is influenced to a considerable degree by muscle contraction, which may have led to hanging cast principle; - note displacing forces: - frx just distal to insertion of deltoid muscle are prone to abduction of proximal fragment & also require special attention;
 - axial malalignment: - upper arm will accommodate deg of anterior angulation & deg of varus; - this amount of angulation would be considered acceptable for patients w/ low to moderate functional demands; - overriding fracture: - bayonet position w/ upto 1 inch of shortening is acceptable; - over-riding displacement is influenced to a considerable degree by muscle contraction, which may have led to hanging cast principle; - note displacing forces: - frx just distal to insertion of deltoid muscle are prone to abduction of proximal fragment & also require special attention;")
42
Humeral Shaft Fracture

43
Humeral Fractures Treatment
Non-operative Acceptable alignment AP anglulation - 20 deg Varus – 30 deg <30mm shortening 70-80% with % union rates Time-consuming and requires cooperative patient Collar and cuff; coaptation splint; hanging cast; functional bracing Weight of forearm provides traction Non Operative Treatment of Humeral Shaft Frx: - note that these injuries are often very painful and that good initial immobilization is required; - long arm splint needs to be applied from shoulder to wrist to fully immobilize the extremity; - although rate of union is generally high with non operative treatment, incidence of mild malunion is high; - in the study by A. Sarmiento MD et al (J Bone Joint Surg [Am] 82-A: , 2000), the researchers were able to follow 620 patients with humeral shaft fractures that were treated with cast bracing; - 465 (75 %) of the fractures were closed, and 155 (25 percent) were open; - non-union: 9 patients (6 %) who had an open fracture and seven (less than 2 %) who had a closed fracture had a nonunion after bracing; - 87 % of the 565 patients for whom AP radiographs were available, the fracture healed in less than 16 deg of varus angulation, and in 81 % of the 546 for whom lateral radiographs were available, it healed in less than 16 deg of anterior angulation; - at the time of brace removal, 98 % of the patients had limitation of shoulder motion of 25 degrees or less; - cast bracing: - can be used for most closed humeral shaft frx; - in most cases, cast braces are applied at days following injury; - forces displacing the fracture: - hanging casts: - may produce frx distraction & may increase risk of nonunion; - references: - Tips of the trade: 41. Modified coaptation splint for humeral shaft fractures. Non-operative: Between 70% and 80% (1) of fractures can be managed non-operatively with an expected union rate of %. Non-operative management is time consuming requiring, a co-operative patient, frequent clinic visits with radiographs, and proficient plaster room technicians. Methods of maintaining reduction include the use of the following: a collar and cuff, a coaptation splint (sugar tong), a hanging cast (3), and a functional brace (4,5) either custom or ready made. The shoulder and less importantly the elbow have a wide arc of normal movement which enables us to place our hand where we wish. However as a result a displacement of 20 degrees anterior angulation, 30 degrees of varus, and 30mm of shortening may be tolerated with little functional deficit (2). Most of the non-operative methods rely on the weight of the forearm / arm providing traction with a patient that is either sitting up or ambulatory. Case Example:
, the researchers were able to follow 620 patients with humeral shaft fractures that were treated with cast bracing; (75 %) of the fractures were closed, and 155 (25 percent) were open; - non-union: 9 patients (6 %) who had an open fracture and seven (less than 2 %) who had a closed fracture had a nonunion after bracing; - 87 % of the 565 patients for whom AP radiographs were available, the fracture healed in less than 16 deg of varus angulation, and in 81 % of the 546 for whom lateral radiographs were available, it healed in less than 16 deg of anterior angulation; - at the time of brace removal, 98 % of the patients had limitation of shoulder motion of 25 degrees or less; - cast bracing: - can be used for most closed humeral shaft frx; - in most cases, cast braces are applied at days following injury; - forces displacing the fracture: - hanging casts: - may produce frx distraction & may increase risk of nonunion; - references: - Tips of the trade: 41. Modified coaptation splint for humeral shaft fractures. Non-operative: Between 70% and 80% (1) of fractures can be managed non-operatively with an expected union rate of %. Non-operative management is time consuming requiring, a co-operative patient, frequent clinic visits with radiographs, and proficient plaster room technicians. Methods of maintaining reduction include the use of the following: a collar and cuff, a coaptation splint (sugar tong), a hanging cast (3), and a functional brace (4,5) either custom or ready made. The shoulder and less importantly the elbow have a wide arc of normal movement which enables us to place our hand where we wish. However as a result a displacement of 20 degrees anterior angulation, 30 degrees of varus, and 30mm of shortening may be tolerated with little functional deficit (2). Most of the non-operative methods rely on the weight of the forearm / arm providing traction with a patient that is either sitting up or ambulatory. Case Example:")
44
Humeral Fractures Treatment
Operative Absolute Indications Failure of closed treatment Associated articular involvement Vascular injuries Ipsilateral forearm fractures Pathological fractures Open fractures Polytrauma Relative Indications Short oblique or transverse fracture in an active individual Body habitus Patient compliance Staff considerations

45
Humeral Fractures Complications
Radial nerve palsy Most at risk – distal 1/3 fractures Occurs up to 18% of fractures 90% neurapraxias and heal in 3-4 mos Exploration indicated No recovery in 3-4 mos (clinical or EMG) Loss of function with closed reduction Open fractures Holstein-Lewis distal 1/3 spiral fractures A neuromuscular examination of the arm, hand, and wrist can identify radial nerve dysfunction. There may be weakness of the wrist and finger extension muscles (with decreased ability to extend the arm at the elbow), a minor decreased ability to rotate the arm outward (supination), and difficulty lifting the wrist or fingers (extensor muscle weakness). Wrist drop or finger drop may be present, or there may be atrophy (muscle loss) of some of the muscles of the forearm. A detailed patient history may be needed to determine the possible cause of the neuropathy. Rarely, radial nerve dysfunction may be difficult to differentiate from a stroke in the brain. Tests that reveal nerve dysfunction may include: EMG (a recording of electrical activity in muscles) Nerve conduction tests Nerve biopsy Head MRI (to rule out stroke) Tests are guided by the suspected cause of the dysfunction, as suggested by the history, symptoms, and pattern of symptom development. They may include various blood tests, X-rays, scans, or other tests and procedures.
 Loss of function with closed reduction. Open fractures. Holstein-Lewis distal 1/3 spiral fractures. A neuromuscular examination of the arm, hand, and wrist can identify radial nerve dysfunction. There may be weakness of the wrist and finger extension muscles (with decreased ability to extend the arm at the elbow), a minor decreased ability to rotate the arm outward (supination), and difficulty lifting the wrist or fingers (extensor muscle weakness). Wrist drop or finger drop may be present, or there may be atrophy (muscle loss) of some of the muscles of the forearm. A detailed patient history may be needed to determine the possible cause of the neuropathy. Rarely, radial nerve dysfunction may be difficult to differentiate from a stroke in the brain. Tests that reveal nerve dysfunction may include: EMG (a recording of electrical activity in muscles) Nerve conduction tests. Nerve biopsy. Head MRI (to rule out stroke) Tests are guided by the suspected cause of the dysfunction, as suggested by the history, symptoms, and pattern of symptom development. They may include various blood tests, X-rays, scans, or other tests and procedures.")
46
Supracondylar fracture Diagnosis
Supracondylar fractures Most common pediatric elbow fracture (65% of fractures and dislocations of the elbow) Commonly associated with neurovascular injury Discussion: - in children, supracondylar frxs typically remains extra-articular & involves thin bone between coronoid fossa & olecranon fossa of distal humerus; - frx line angles from anterior distal point to posterior prox site; - in adults, supracondylar frx of humerus may be intra-articular; - frx occurs most often around age 6-7 years; - classification: - 2 types: extension type (95%) & flexion type; - gartland classification for extension fractures: - recognizes that anterior cortex fails first w/ resultant posterior displacement of distal fragment; - type I: non-displaced frx; - type II: displaced with intact posterior cortex; - type III: displaced with no cortical contact; - associated injuries: - palpate distal radius for frx (occurs in 5-6%); Clinically a lot of swelling and neurovascular injury (test peripheral pulses and cap refill) - vascular compromise occurs in about 5% of children w/ supracondylar frx; - less than 1% will be complicated by compartment syndrome and the resulting sequelae of Volkmann's contracture; - note that a median nerve palsy, may mask a pending compartment syndrome; - frxs w/ posterolateral displacement of distal fragment are more susceptible to vascular injury, since the medial spike of the proximal humerus can tether the brachial artery; Treatment: - while patient is being worked up, consider applying a continuous pulse ox so the nurses can follow an objective measurement of perfusion; - arteriography may be indicated if circulation is restored following reduction but is somewhat diminished compared to the opposite extremity; - if circulation is not restored by closed reduction, immediate open reduction and surgical exploration of the artery is indicated; - arteriography is not indicated since it provides little additional information and only delays restoration of circulation to the extremity; - morbidity assoc w/ surgical exposure of the artery is low; - procrastination will only increase patient morbidity; - median nerve: - most common neural injury is to anterior-interosseous branch; - in type III frx, upto 50% of pts may show median nerve deficits; - is frequently missed because of lack of sensory changes; - may be seen injured in postero-laterally displaced supracondylar frx & is associated w/ vascular injuries; - nerve is tethered on the medial spike of proximal fragment; - note that a median nerve palsy may mask a pending compartment syndrome; - radial nerve; - may be injured by anterior spike of proximal fragment of humerus w/ supracondylar frx w/ post-medial displacement; - in type III frx, upto 25% of pts may show radial nerve deficits; - most nerve palsies resulting from supracondylar frx are neuropraxias, and therefore will resolve spontaneously; - motor function should recover by 3 months and sensory changes should recover by 6 months; - a mixed palsy (motor loss but no sensory loss) may have a better prognosis than a complete palsy (motor and sensory loss);
 Commonly associated with neurovascular injury. Discussion: - in children, supracondylar frxs typically remains extra-articular & involves thin bone between coronoid fossa & olecranon fossa of distal humerus; - frx line angles from anterior distal point to posterior prox site; - in adults, supracondylar frx of humerus may be intra-articular; - frx occurs most often around age 6-7 years; - classification: - 2 types: extension type (95%) & flexion type; - gartland classification for extension fractures: - recognizes that anterior cortex fails first w/ resultant posterior displacement of distal fragment; - type I: non-displaced frx; - type II: displaced with intact posterior cortex; - type III: displaced with no cortical contact; - associated injuries: - palpate distal radius for frx (occurs in 5-6%); Clinically a lot of swelling and neurovascular injury (test peripheral pulses and cap refill) - vascular compromise occurs in about 5% of children w/ supracondylar frx; - less than 1% will be complicated by compartment syndrome and the resulting sequelae of Volkmann s contracture; - note that a median nerve palsy, may mask a pending compartment syndrome; - frxs w/ posterolateral displacement of distal fragment are more susceptible to vascular injury, since the medial spike of the proximal humerus can tether the brachial artery; Treatment: - while patient is being worked up, consider applying a continuous pulse ox so the nurses can follow an objective measurement of perfusion; - arteriography may be indicated if circulation is restored following reduction but is somewhat diminished compared to the opposite extremity; - if circulation is not restored by closed reduction, immediate open reduction and surgical exploration of the artery is indicated; - arteriography is not indicated since it provides little additional information and only delays restoration of circulation to the extremity; - morbidity assoc w/ surgical exposure of the artery is low; - procrastination will only increase patient morbidity; - median nerve: - most common neural injury is to anterior-interosseous branch; - in type III frx, upto 50% of pts may show median nerve deficits; - is frequently missed because of lack of sensory changes; - may be seen injured in postero-laterally displaced supracondylar frx & is associated w/ vascular injuries; - nerve is tethered on the medial spike of proximal fragment; - note that a median nerve palsy may mask a pending compartment syndrome; - radial nerve; - may be injured by anterior spike of proximal fragment of humerus w/ supracondylar frx w/ post-medial displacement; - in type III frx, upto 25% of pts may show radial nerve deficits; - most nerve palsies resulting from supracondylar frx are neuropraxias, and therefore will resolve spontaneously; - motor function should recover by 3 months and sensory changes should recover by 6 months; - a mixed palsy (motor loss but no sensory loss) may have a better prognosis than a complete palsy (motor and sensory loss);")
47
Supracondylar fractures Diagnosis
Classification Type I - non-displaced Type II - angulated but not translated in the sagittal plane with hinging of the posterior cortex of the humerus Type III - posteriorly displaced with IIIA being posteromedial and type IIIB being posterolateral

48
Supracondylar Fractures Diagnosis
Radiology AP view Baumann’s angle Medial epichondylar epiphyseal angle (MEE) Lateral view Humero- trochlear angle Oblique Baumann’s – 15 MEE – – not accurate < 3 yo HTA – 40 Discussion: - note that accurate AP and Lateral views are essential to judge the reduction; - slightly oblique views can lead to acceptance of malreduction; AP View: - comparison films are usually required to judge amount of relative varus; - generally no more than 4 deg of varus is accepted (as determined on by the Bauman's angle, seen on AP view): - obtain AP radiograph of opposite extremity for comparison; - note that inadequate radiographs may hide a "T" condylar fracture; Lateral View: - insist on true lateral; - normally the anterior humeral line should pass thru ossification center of the lateral condyle (this also holds true for type I frx); - called the anterior humeral line; - w/ type II frx: - anterior humeral line does not transect capitellum; - there should be a radiolucent interval between ossification center of capitellum and the semilunar notch of the olecranon; - any overlap of the capitulum and semilunar notch implies malrotation; - condylar - humeral shaft angle: - needs to be restored inorder to restore full flexion; soft tissue structures: - superficial part of anterior fat pad should be in front of coronoid fossa; - in normal elbow the anterior fat pad should be barely visualized & posterior fat pad should not be seen at all; - look for small radiolucent area between bony rim & moderate opaque shadows of brachialis; - w/ effusion 2nd to type I frx, there will be anterior & superior displacement of anterior fat pad; - Oblique View: - may be useful for diagnosing type I extension frx;
 Lateral view. Humero- trochlear angle. Oblique. Baumann’s – 15. MEE – – not accurate < 3 yo. HTA – 40. Discussion: - note that accurate AP and Lateral views are essential to judge the reduction; - slightly oblique views can lead to acceptance of malreduction; AP View: - comparison films are usually required to judge amount of relative varus; - generally no more than 4 deg of varus is accepted (as determined on by the Bauman s angle, seen on AP view): - obtain AP radiograph of opposite extremity for comparison; - note that inadequate radiographs may hide a T condylar fracture; Lateral View: - insist on true lateral; - normally the anterior humeral line should pass thru ossification center of the lateral condyle (this also holds true for type I frx); - called the anterior humeral line; - w/ type II frx: - anterior humeral line does not transect capitellum; - there should be a radiolucent interval between ossification center of capitellum and the semilunar notch of the olecranon; - any overlap of the capitulum and semilunar notch implies malrotation; - condylar - humeral shaft angle: - needs to be restored inorder to restore full flexion; soft tissue structures: - superficial part of anterior fat pad should be in front of coronoid fossa; - in normal elbow the anterior fat pad should be barely visualized & posterior fat pad should not be seen at all; - look for small radiolucent area between bony rim & moderate opaque shadows of brachialis; - w/ effusion 2nd to type I frx, there will be anterior & superior displacement of anterior fat pad; - Oblique View: - may be useful for diagnosing type I extension frx;")
49
Supracondylar Fracture Treatment
Non-displaced fxs – cast immobilization Displaced fxs – close reduction with percutaneous pinning

50
Suprachondylar fracture Complications
Vascular injury – brachial aa Neurologic deficits – median nerve; possible radial nerve Volkmann’s contracture Cubitus varus Vascular Discussion: - vascular compromise occurs in about 5% of children w/ supracondylar frx; - less than 1% will be complicated by compartment syndrome and the resulting sequelae of Volkmann's contracture; - note that a median nerve palsy, may mask a pending compartment syndrome; - frxs w/ posterolateral displacement of distal fragment are more susceptible to vascular injury, since the medial spike of the proximal humerus can tether the brachial artery; Treatment: - while patient is being worked up, consider applying a continuous pulse ox so the nurses can follow an objective measurement of perfusion; Neuro deficits - median nerve: - most common neural injury is to anterior-interosseous branch; - in type III frx, upto 50% of pts may show median nerve deficits; - is frequently missed because of lack of sensory changes; - may be seen injured in postero-laterally displaced supracondylar frx & is associated w/ vascular injuries; - nerve is tethered on the medial spike of proximal fragment; - note that a median nerve palsy may mask a pending compartment syndrome; - radial nerve; - may be injured by anterior spike of proximal fragment of humerus w/ supracondylar frx w/ post-medial displacement; - in type III frx, upto 25% of pts may show radial nerve deficits; Treatment: - most nerve palsies resulting from supracondylar frx are neuropraxias, and therefore will resolve spontaneously; - motor function should recover by 3 months and sensory changes should recover by 6 months; - a mixed palsy (motor loss but no sensory loss) may have a better prognosis than a complete palsy (motor and sensory loss); Volmann’s Discussion: - type of forearm ischemic contracture resulting from brachial artery injury usually associated w/ supracondylar frx of humerus; - may see loss of motor & sensory function, however, classic involvment is w/ anterior interosseous branch of median nerve; Cubitus varus - cubitus varus is the most common complication following supracondylar frx, - orginally, etilogy of cubitus varus was thought to occur because of growth disturbance of distal humeral epiphysis; - this may be true but is uncommon; current thinking is that it stems from malreduction of frx, with medial displacement, internal rotation, and extension of the distal fragment; - this then permits distal fragment to tilt into varus; - cubitus varus produces a cosmetic deformity but little function deficit; - during reduction, a small amount of medial or lateral displacement or small amount of anterior or posterior angulation may be tolerated, but any malrotation is not acceptable; - rotation is verified under flouro w/ AP view, lateral view, & oblique views; - if reduction is not be obtained, there may be soft-tissue interposition which mandates open reduction;
 may have a better prognosis than a complete palsy (motor and sensory loss); Volmann’s. Discussion: - type of forearm ischemic contracture resulting from brachial artery injury usually associated w/ supracondylar frx of humerus; - may see loss of motor & sensory function, however, classic involvment is w/ anterior interosseous branch of median nerve; Cubitus varus. - cubitus varus is the most common complication following supracondylar frx, - orginally, etilogy of cubitus varus was thought to occur because of growth disturbance of distal humeral epiphysis; - this may be true but is uncommon; current thinking is that it stems from malreduction of frx, with medial displacement, internal rotation, and extension of the distal fragment; - this then permits distal fragment to tilt into varus; - cubitus varus produces a cosmetic deformity but little function deficit; - during reduction, a small amount of medial or lateral displacement or small amount of anterior or posterior angulation may be tolerated, but any malrotation is not acceptable; - rotation is verified under flouro w/ AP view, lateral view, & oblique views; - if reduction is not be obtained, there may be soft-tissue interposition which mandates open reduction;")
51
Humerus Injuries Emergency Care
Sling Ladder splint

52
Elbow Injuries

53
Radial Anatomy Radial head articulates with capitellum
Radial neck tapers to radial tuberosity which is insertion for biceps brachii tendon

54
Ulnar Anatomy Sigmoid/semilunar/ trochlear notch
Anteriorly composed of coronoid process Posteriorly composed of olecranon process Articulates with trochlea of humerus

55
Elbow Joint Articulation
- Elbow consists of articulations: Ulnohumeral (elbow flexion/extension) Radiohumeral (forearm pronation/supination) Radioulnar (forearm pronation/supination)
 Radiohumeral (forearm pronation/supination) Radioulnar (forearm pronation/supination)")
56
Elbow Injuries MOI Fall onto outstretched hand (FOOSH) with elbow extended or direct trauma
 with elbow extended or direct trauma")
57
Elbow dislocation Diagnosis
Second to shoulder dislocations Posterior dislocation account for 80-90% Most occur without fracture Posterior dislocations, in which the coronoid process disengages from the trochlea and moves posteriorly (figure 1), account for more than 90% of dislocations (2). Whether the elbow dislocates posteromedially or posterolaterally, the injury and treatment are the same Discussion: - elbow dislocation is the second most common major joint dislocation; - dislocation is usually closed and posterior; - elbow dislocations without fracture are termed "simple." - dislocations are classified according to direction of dislocation, namely posterior, posterolateral, posteromedial, lateral, medial, or divergent; - in dealing w/ elbow dislocations, it is key to determine whether the dislocation is simple or complex; stability of elbow: - primary stabilizers - ulnohumeral articulation - coronoid: clinical experience suggests 50% intact coronoid requirement for stability with or without ligamentous integrity - olecranon contribution to stability inversely correlated with resection amount: >30% articular surface of olecranon needed for stability - MCL is the main stabilizer of the elbow joint - consists of anterior oblique ligament, posterior oblique ligament; - MCL provides 54% valgus stability, while osseous articulation provides 33%; - secondary stabilizers - radiohumeral articulation (most important) - capsule: greatest role in extension of elbow, insignificant role (<10%) in flexion - musculature (dynamic) - ref: Morrey BF, An KN: Articular and ligamentous contributions to the stability of the elbow joint. Am J Sports Med 1983;11: pathoanatomy: simple dislocation: - rupture of capsule, rupture of MCL, lateral ligamentous structures, rupture of flexor pronator mass to a variable extent, injury to the brachialis muscle; - rupture of brachial artery has been reported; mechanism: - dislocations of elbow usually result from fall onto extended elbow. - anatomic morphology of semilunar notch may predispose to elbow dislocation; - central angle of semilunar notch is sig large in group of pts who had dislocation of the elbow compared to normals; Exam Exam: - vascular injury: - closed dislocations are rarely assoc w/ vascular injury, whereas open &/or ant dislocations are commonly assoc w/ such injury; - in open dislocations, brachial artery is disrupted by forcible hyperextension (median nerve injury is commonly associated with such injuries); - references: - Closed elbow dislocation and brachial artery damage. [Review] - neuro injury: - neuropraxia is occurs in 20%, usually involving ulnar or median n (AIN branch); - ulnar nerve palsy may occur up to 14% of adult elbow dislocations, and the occurance of ulnar nerve palsy is much higher in pediatric dislocations w/ an associated medial epicondyle frx; - most neurologic deficits are transient, but entrapment of median nerve w/ elbow joint after manipulation is more common in pediatric dislocations; - references: - Median nerve palsy after posterolateral elbow dislocation. - bony displacement: - when nl elbow is extended, olecranon process & medial & lat form 3 points on straight line, & when nl elbow is flexed to 90 deg in lateral view, olecranon is aligned vertically w/ epicondyles; - tip of the olecranon is, however, definitely posterior to the plane of the epicondyles; - in post dislocation, olecranon process is displaced backward from its normal position in relation to humerus, & one can palpate the concavity of the semilunar notch; - increasing degree of elbow flexion exaggerates the prominence of the olecranon process - Very important to examine whole upper extremity for evaluation of Essex-Lopresti lesion at wrist or associated fractures Clinically they present with swelling and obvious deformity. Neurovascular exam – pulses and cap refill. Ulnar nerve neuropraxia. Essential to get pre and post reduction films to assess for fracture
, account for more than 90% of dislocations (2). Whether the elbow dislocates posteromedially or posterolaterally, the injury and treatment are the same. Discussion: - elbow dislocation is the second most common major joint dislocation; - dislocation is usually closed and posterior; - elbow dislocations without fracture are termed simple. - dislocations are classified according to direction of dislocation, namely posterior, posterolateral, posteromedial, lateral, medial, or divergent; - in dealing w/ elbow dislocations, it is key to determine whether the dislocation is simple or complex; stability of elbow: - primary stabilizers - ulnohumeral articulation - coronoid: clinical experience suggests 50% intact coronoid requirement for stability with or without ligamentous integrity - olecranon contribution to stability inversely correlated with resection amount: >30% articular surface of olecranon needed for stability - MCL is the main stabilizer of the elbow joint - consists of anterior oblique ligament, posterior oblique ligament; - MCL provides 54% valgus stability, while osseous articulation provides 33%; - secondary stabilizers - radiohumeral articulation (most important) - capsule: greatest role in extension of elbow, insignificant role (<10%) in flexion - musculature (dynamic) - ref: Morrey BF, An KN: Articular and ligamentous contributions to the stability of the elbow joint. Am J Sports Med 1983;11: pathoanatomy: simple dislocation: - rupture of capsule, rupture of MCL, lateral ligamentous structures, rupture of flexor pronator mass to a variable extent, injury to the brachialis muscle; - rupture of brachial artery has been reported; mechanism: - dislocations of elbow usually result from fall onto extended elbow. - anatomic morphology of semilunar notch may predispose to elbow dislocation; - central angle of semilunar notch is sig large in group of pts who had dislocation of the elbow compared to normals; Exam. Exam: - vascular injury: - closed dislocations are rarely assoc w/ vascular injury, whereas open &/or ant dislocations are commonly assoc w/ such injury; - in open dislocations, brachial artery is disrupted by forcible hyperextension (median nerve injury is commonly associated with such injuries); - references: - Closed elbow dislocation and brachial artery damage. [Review] - neuro injury: - neuropraxia is occurs in 20%, usually involving ulnar or median n (AIN branch); - ulnar nerve palsy may occur up to 14% of adult elbow dislocations, and the occurance of ulnar nerve palsy is much higher in pediatric dislocations w/ an associated medial epicondyle frx; - most neurologic deficits are transient, but entrapment of median nerve w/ elbow joint after manipulation is more common in pediatric dislocations; - references: - Median nerve palsy after posterolateral elbow dislocation. - bony displacement: - when nl elbow is extended, olecranon process & medial & lat form 3 points on straight line, & when nl elbow is flexed to 90 deg in lateral view, olecranon is aligned vertically w/ epicondyles; - tip of the olecranon is, however, definitely posterior to the plane of the epicondyles; - in post dislocation, olecranon process is displaced backward from its normal position in relation to humerus, & one can palpate the concavity of the semilunar notch; - increasing degree of elbow flexion exaggerates the prominence of the olecranon process - Very important to examine whole upper extremity for evaluation of Essex-Lopresti lesion at wrist or associated fractures. Clinically they present with swelling and obvious deformity. Neurovascular exam – pulses and cap refill. Ulnar nerve neuropraxia. Essential to get pre and post reduction films to assess for fracture.")
58
Elbow dislocation Treatment
Immediate reduction vs splint and refer Children should be splinted; increase incidence of fractures Need for radiographs After relocation Assess neurovascular status Assess joint stability Rehab early Parvin's Method of Closed Reduction: - pt lies prone on stretcher, & physician applies gentle downward traction on the wrist for a few minutes; - as olecranon begins to slip distally, MD lifts up gently on arm; - alternatively MD may guide reduction of olecranon w/ opposite hand; - longitudinal traction followed by flexion of the elbow usually succeeds in obtaining a congruent reduction. Immediate reduction depends on physician expertise and the need for radiographs and sedation. Advantages of immediate reduction are pain relief and restoration of CMS staus. Remove the patient from the field of action. Place the patient supine or prone (I prefer prone, figure 2) on an exam table or other stable surface with the injured arm flexed about 90° over the edge. Correct any medial or lateral translation of the proximal ulna. Grasp the wrist of the patient's injured arm and apply traction and slight supination to the forearm to distract and unlock the coronoid process from the olecranon fossa. Countertraction on the brachium by an assistant can help. With the other hand, apply pressure to the olecranon while pronating the arm to complete the reduction. An obvious "clunk," along with restoration of normal joint contour, indicates reduction. Assessment of Stability: - passive ROM to w/in 20 deg of full extension w/o subluxation implies a stable reduction; - in 58 traumatic dislocations, closed reduction failed in 10% of cases. - Post Op Vascular Check: - during reduction, the brachial artery, median and ulnar nerves are most vulnerable, and can be entrapped with manipulation; - loss of pulse does not preclude attempted closed reduction, however, if arterial flow is not reestablished after reduction, and the hand is poorly perfused, the patient should be prepared for immediate arterial reconstruction with saphenous vein grafting; - if perfusion of the forearm and hand has been poor because of delayed treatment, volar fasciotomy should be performed to reduce the chance of Volkmann's contracture; Non Operative Treatment: - stable articulation will allow for early flexion & extension if valgus stress is prevented after reduction; - no one has demonstrated a benefit from operative repair of MCL in simple dislocations; - best Rx results are obtained w/ early protected ROM begun before 2 wks; - if there is increased stability in pronation, then the elbow should be placed in a cast brace with the elbow in pronation; - final clinical outcome for simple dislocations of the elbow is dramatically affected by the duration of immobilization; - recurrent dislocation is unusual; - mild loss of extension is common, prolonged immobilization over two wks is assoc w/ greater flexion contracture;
 on an exam table or other stable surface with the injured arm flexed about 90° over the edge. Correct any medial or lateral translation of the proximal ulna. Grasp the wrist of the patient s injured arm and apply traction and slight supination to the forearm to distract and unlock the coronoid process from the olecranon fossa. Countertraction on the brachium by an assistant can help. With the other hand, apply pressure to the olecranon while pronating the arm to complete the reduction. An obvious clunk, along with restoration of normal joint contour, indicates reduction. Assessment of Stability: - passive ROM to w/in 20 deg of full extension w/o subluxation implies a stable reduction; - in 58 traumatic dislocations, closed reduction failed in 10% of cases. - Post Op Vascular Check: - during reduction, the brachial artery, median and ulnar nerves are most vulnerable, and can be entrapped with manipulation; - loss of pulse does not preclude attempted closed reduction, however, if arterial flow is not reestablished after reduction, and the hand is poorly perfused, the patient should be prepared for immediate arterial reconstruction with saphenous vein grafting; - if perfusion of the forearm and hand has been poor because of delayed treatment, volar fasciotomy should be performed to reduce the chance of Volkmann s contracture; Non Operative Treatment: - stable articulation will allow for early flexion & extension if valgus stress is prevented after reduction; - no one has demonstrated a benefit from operative repair of MCL in simple dislocations; - best Rx results are obtained w/ early protected ROM begun before 2 wks; - if there is increased stability in pronation, then the elbow should be placed in a cast brace with the elbow in pronation; - final clinical outcome for simple dislocations of the elbow is dramatically affected by the duration of immobilization; - recurrent dislocation is unusual; - mild loss of extension is common, prolonged immobilization over two wks is assoc w/ greater flexion contracture;")
59
Elbow fracture Radial head – 30% Olecrenon – 20%
Coronoid fractures – 10 to 15% of elbow dislocations

60
Elbow fat pads Look for fat pad sign!!!!
Norell (1) first associated a radiographic posterior fat-pad sign with elbow trauma in His theory that a posterior fat-pad sign would be present with various arthropathies was later confirmed. Bledsoe and Izenstark (2) described the anterior fat-pad sign in 1959. The anterior fat pad is a summation of the radial and coronoid fat pads. The shape is determined by the brachial muscle in extension and by intrinsic surface tension, bone, capsule, and intra-articular volume in flexion. The shape of the posterior fat pad, located in the olecranon fossa, is determined by the triceps tendon and anconeus muscle during flexion. The posterior fat pad is more mobile in extension, and the shape is defined by surface tension, bone, capsule, and intra-articular volume. Standard x-rays of the elbow include an anteroposterior view with the elbow extended and a true lateral view with the elbow flexed to 90° and the forearm neutral. The fat pads are best visualized in the lateral view. In a positive anterior fat-pad sign, the fat pad is displaced ventrally and superiorly, changing the inferior margin from convex to concave. This configuration, an exaggeration of its normal appearance, resembles a ship's sail ("sail sign"). A false-negative anterior fat-pad sign can be seen with insufficient effusion, poor positioning, extracapsular fracture, and capsular rupture. When the posterior fat-pad sign is positive, the extension of the synovial capsule with the elbow in 90° of flexion displaces the fat pad superiorly and dorsally. A false-positive posterior fat-pad sign can occur with the elbow in extension and is caused by olecranon process displacement and posterior capsule laxity. A paradoxical positive posterior fat-pad sign can occur with extra-articular processes. Neoplasia or hemorrhage from a supracondylar humeral fracture may elevate the periosteum and displace the proximal half of the posterior fat pad dorsally.
 first associated a radiographic posterior fat-pad sign with elbow trauma in His theory that a posterior fat-pad sign would be present with various arthropathies was later confirmed. Bledsoe and Izenstark (2) described the anterior fat-pad sign in The anterior fat pad is a summation of the radial and coronoid fat pads. The shape is determined by the brachial muscle in extension and by intrinsic surface tension, bone, capsule, and intra-articular volume in flexion. The shape of the posterior fat pad, located in the olecranon fossa, is determined by the triceps tendon and anconeus muscle during flexion. The posterior fat pad is more mobile in extension, and the shape is defined by surface tension, bone, capsule, and intra-articular volume. Standard x-rays of the elbow include an anteroposterior view with the elbow extended and a true lateral view with the elbow flexed to 90° and the forearm neutral. The fat pads are best visualized in the lateral view. In a positive anterior fat-pad sign, the fat pad is displaced ventrally and superiorly, changing the inferior margin from convex to concave. This configuration, an exaggeration of its normal appearance, resembles a ship s sail ( sail sign ). A false-negative anterior fat-pad sign can be seen with insufficient effusion, poor positioning, extracapsular fracture, and capsular rupture. When the posterior fat-pad sign is positive, the extension of the synovial capsule with the elbow in 90° of flexion displaces the fat pad superiorly and dorsally. A false-positive posterior fat-pad sign can occur with the elbow in extension and is caused by olecranon process displacement and posterior capsule laxity. A paradoxical positive posterior fat-pad sign can occur with extra-articular processes. Neoplasia or hemorrhage from a supracondylar humeral fracture may elevate the periosteum and displace the proximal half of the posterior fat pad dorsally.")
61
Elbow Fat Pads

62
Elbow Fractures Treatment
Radial Head Non-displaced (type I) sling and or splint until no pain Displaced (type II) Longer immobilization (1-2 weeks) removal of bone fragments if necessary Comminuted (Type III) Surgery to remove bone fragments Repair ligament damage Discussion: - radial head frx is most common type of elbow fracture in adults; - frx of the radial head occurs primarily in adults, whereas fractures of the radial neck are more common in children; - frx of the radial head and neck of the radius generally results from a hard fall on an outstretched hand; - impact of fall drives head of radius axially onto capitulum of humerus; - the high frequency of frx in the anterolateral aspect of radial head occurs as a result of lack of subchondral bone under the anterolaterl aspect of the radial head; - because the anterolateral aspect of radial head does not articulate w/ sigmoid fossa, frx in the region are amenable to fixation w/ small screws; associated injuries: - frx of the capitellum - distal radius frx - dislocation of the distal RU joint (Essex Lopresti Fracture) - valgus instability (MCL rupture) - probably more common than is reported; - indications for repair of the MCL will be determined based on stability of the elbow thru a functional range of motion; - rupture of the triceps tendon - elbow dislocation: - terrible triad: RHF + MCL + coronoid process frx; Dx and Exam: - dx of a radial head fracture may be difficult; - pain, effusion in the elbow, & tenderness on palpation directly over radial head are typical manifestations; - if frx is displaced, click or crepitus over radial head is detected w/ supination; - if elbow ROM is limited, then aspirate and inject several cc of lidocaine, and then re-examine; - check for blocks to flexion-extension as well as supination-pronation; - wrist tenderness with ROM is common;
 sling and or splint until no pain. Displaced (type II) Longer immobilization (1-2 weeks) removal of bone fragments if necessary. Comminuted (Type III) Surgery to remove bone fragments. Repair ligament damage. Discussion: - radial head frx is most common type of elbow fracture in adults; - frx of the radial head occurs primarily in adults, whereas fractures of the radial neck are more common in children; - frx of the radial head and neck of the radius generally results from a hard fall on an outstretched hand; - impact of fall drives head of radius axially onto capitulum of humerus; - the high frequency of frx in the anterolateral aspect of radial head occurs as a result of lack of subchondral bone under the anterolaterl aspect of the radial head; - because the anterolateral aspect of radial head does not articulate w/ sigmoid fossa, frx in the region are amenable to fixation w/ small screws; associated injuries: - frx of the capitellum - distal radius frx - dislocation of the distal RU joint (Essex Lopresti Fracture) - valgus instability (MCL rupture) - probably more common than is reported; - indications for repair of the MCL will be determined based on stability of the elbow thru a functional range of motion; - rupture of the triceps tendon - elbow dislocation: - terrible triad: RHF + MCL + coronoid process frx; Dx and Exam: - dx of a radial head fracture may be difficult; - pain, effusion in the elbow, & tenderness on palpation directly over radial head are typical manifestations; - if frx is displaced, click or crepitus over radial head is detected w/ supination; - if elbow ROM is limited, then aspirate and inject several cc of lidocaine, and then re-examine; - check for blocks to flexion-extension as well as supination-pronation; - wrist tenderness with ROM is common;")
63
Elbow Fractures Treatment
Olecrenon Fracture Non-displaced (type I) Sling, splint and or cast for 3-4 weeks Follow by x-ray for dislocation of fracture Displaced (type II) ORIF Comminuted (Type III) Discussion: low energy olecranon fractures: - most commonly occur in elderly patients, and result from indirect trauma; - fracture and results from a sudden pull of both the triceps and brachialis muscles; - frx begins at midpoint of trochlear notch and extends distally to enter semilunar notch; - amount of frx displacement is influenced by the pull of the triceps muscle as well as any disruption of triceps aponeurosis or periosteum; - high energy fractures: - olecranon fractures in younger patients are more often high energy injuries, resulting from direct trauma; - often there is associated comminution or concomitant ulnar shaft frx; Physical Exam: - because all frx of the olecranon process have some intra-articular component, there is generally a hemorrhagic effusion of elbow joint; - this results in pain and swelling over the olecranon; - inability to extend the elbow actively against gravity is a key finding; - it indicates the discontinuity of the triceps mechanism; - the presence or absence of this sign determines the plan of Rx:
 Sling, splint and or cast for 3-4 weeks. Follow by x-ray for dislocation of fracture. Displaced (type II) ORIF. Comminuted (Type III) Discussion: low energy olecranon fractures: - most commonly occur in elderly patients, and result from indirect trauma; - fracture and results from a sudden pull of both the triceps and brachialis muscles; - frx begins at midpoint of trochlear notch and extends distally to enter semilunar notch; - amount of frx displacement is influenced by the pull of the triceps muscle as well as any disruption of triceps aponeurosis or periosteum; - high energy fractures: - olecranon fractures in younger patients are more often high energy injuries, resulting from direct trauma; - often there is associated comminution or concomitant ulnar shaft frx; Physical Exam: - because all frx of the olecranon process have some intra-articular component, there is generally a hemorrhagic effusion of elbow joint; - this results in pain and swelling over the olecranon; - inability to extend the elbow actively against gravity is a key finding; - it indicates the discontinuity of the triceps mechanism; - the presence or absence of this sign determines the plan of Rx:")
64
Elbow Fractures Treatment
Coronoid Fracture Type 1 Immobilization for 2 weeks Type 2 Displaced or humeroulnar joint instability may consider ORIF Type 3 ORIF Discussion: - coronoid helps to resist posterior elbow subluxation; - at least 50% of the coronoid must be present for the ulno-humeral joint to have normal function (ie for joint to be stable); - associated w/ elbow dislocation in upto 40%; - Classification and Treatment: - type I: frx of the tip of the coronoid process; - type II: frx or comminution constitutes about half of coronoid; - treated w/ early motion if no instability is present; - type III: frx or comminution constitues more than half of coronoid; - almost always involves dislocation (see below); - fractures near the coronoid base are associated w/ increased instability due to loss of the stabilizing function of the coronoid itself as well as loss of the insertion of the anterior band of the MCL and anterior joint capsule; - Radiographs: - opening angle: - angle formed by lines drawn from the tip of the olecranon to coronoid and a line drawn down the axis of the ulna; - Dislocation + Coronoid Process Frx: Classification; - frx is due to avulsion by brachialis when elbow is hyperextened; - type I: avulsion of the tip of the coronoid process; - type II: involving less than 50% of the process - for above types closed reduction and early motion is recommended; - fixation of frx fragments may not guarantee stability; - consider external fixation distraction device; - type III: frag involving > 50% of process - almost always associatted w/ posterior dislocation; - assoc w/ high redislocation rate & requires ORIF - there will be assoc valgus instability since MCL inserts onto the fracture fragment; - if frx pattern is not amenable to rigid fixation, is an indication for an external fixation distraction device; - left untreated, the worst of all scenarios may develop: ie, an unstable eblow joint which is also stiff and painful; - in the report by Closkey et al, elbows of cadavera were tested before and after fracture of the coronoid process to assess the stabilizing contribution of the coronoid process under axial loading; - there was no significant difference, at any flexion position, in posterior axial displacement between the intact elbows and the elbows in which 50 percent or less of the coronoid process was fractured (type I and type II) (p = 0.43); - there were significant differences, across all flexion positions, in posterior axial displacement between the intact elbows and the elbows in which more than 50 percent of the coronoid process was fractured (type III) (p = 0.006); - in response to axial load, elbows with a fracture involving more than 50 percent of the coronoid process displace more readily than elbows with a fracture involving 50 percent or less of the coronoid process, especially when the elbow is flexed 60 degrees and beyond; - fixation technque: - anterior approach: - Huston suture passer is passed thru small drill holes thru the coronoid process and ulna which allow passage of heavy non absorable suture for fixation; - ref: The Role of the Coronoid Process in Elbow Stability. A Biomechanical Analysis of Axial Loading* RF. Closkey MD. J Bone Joint Surg [Am] 82-A: , 2000
; - associated w/ elbow dislocation in upto 40%; - Classification and Treatment: - type I: frx of the tip of the coronoid process; - type II: frx or comminution constitutes about half of coronoid; - treated w/ early motion if no instability is present; - type III: frx or comminution constitues more than half of coronoid; - almost always involves dislocation (see below); - fractures near the coronoid base are associated w/ increased instability due to loss of the stabilizing function of the coronoid itself as well as loss of the insertion of the anterior band of the MCL and anterior joint capsule; - Radiographs: - opening angle: - angle formed by lines drawn from the tip of the olecranon to coronoid and a line drawn down the axis of the ulna; - Dislocation + Coronoid Process Frx: Classification; - frx is due to avulsion by brachialis when elbow is hyperextened; - type I: avulsion of the tip of the coronoid process; - type II: involving less than 50% of the process - for above types closed reduction and early motion is recommended; - fixation of frx fragments may not guarantee stability; - consider external fixation distraction device; - type III: frag involving > 50% of process - almost always associatted w/ posterior dislocation; - assoc w/ high redislocation rate & requires ORIF - there will be assoc valgus instability since MCL inserts onto the fracture fragment; - if frx pattern is not amenable to rigid fixation, is an indication for an external fixation distraction device; - left untreated, the worst of all scenarios may develop: ie, an unstable eblow joint which is also stiff and painful; - in the report by Closkey et al, elbows of cadavera were tested before and after fracture of the coronoid process to assess the stabilizing contribution of the coronoid process under axial loading; - there was no significant difference, at any flexion position, in posterior axial displacement between the intact elbows and the elbows in which 50 percent or less of the coronoid process was fractured (type I and type II) (p = 0.43); - there were significant differences, across all flexion positions, in posterior axial displacement between the intact elbows and the elbows in which more than 50 percent of the coronoid process was fractured (type III) (p = 0.006); - in response to axial load, elbows with a fracture involving more than 50 percent of the coronoid process displace more readily than elbows with a fracture involving 50 percent or less of the coronoid process, especially when the elbow is flexed 60 degrees and beyond; - fixation technque: - anterior approach: - Huston suture passer is passed thru small drill holes thru the coronoid process and ulna which allow passage of heavy non absorable suture for fixation; - ref: The Role of the Coronoid Process in Elbow Stability. A Biomechanical Analysis of Axial Loading* RF. Closkey MD. J Bone Joint Surg [Am] 82-A: ,")
65
Elbow dislocation or fracture Emergency Care
Immobilize Sling Posterior elbow splint using ladder splint or SAM splint ice

66
Wrist Injuries

67
Anatomy of the wrist

68
Wrist fracture Incidence of fracture is 2x for snowboarding vs. skiing
With loss of balance, the natural tendency is to break fall with outstretched hand (FOOSH)
")
69
Wrist fracture (distal radial)
Most common - Distal radius or Colles fracture Silver fork deformity General Discussion: - frx was described by Abraham Colles in 1814, originally described as low energy extra articular frx of distal radius occuring in elderly individuals; - frx is typically dorsally displaced and angulated; Neurological Exam: - be sure to examine the AIN, PIN, and median nerve at the wrist; - Carpal tunnel syndrome; - evaluate the strength of the APB; - injury from contact with bone spicules; - is most frequent complication in most series; - in the series by Trumble et al 1998, 4 out of 73 patients showed paresthesias of the median nerve, and in each case symptoms resolved within 4 days without surgery; Vascular: (Allen's Test) Tendon: - EPL; Misc: - ulnar styloid Pain: - radial head / elbow pain: - Pronator Quadratus Tear: - potential area of enlargement at wrist is made by relationship between flexor tendons & their synovial digital sheaths & fascia covering pronator quadratus; - this potential sheath can be enlarged by hemorrhage, edema, or from a torn pronator quadratus occuring from colles frx;
 Tendon: - EPL; Misc: - ulnar styloid Pain: - radial head / elbow pain: - Pronator Quadratus Tear: - potential area of enlargement at wrist is made by relationship between flexor tendons & their synovial digital sheaths & fascia covering pronator quadratus; - this potential sheath can be enlarged by hemorrhage, edema, or from a torn pronator quadratus occuring from colles frx;")
70
Wrist Fracture (distal radial) Median nerve assessment (ant interosseous)
normal abnormal

71
Wrist fracture mechanism:
- fracture is also caused by a forced dorsiflexion of the wrist; - occurs in pts > 50 years of age who fall on out stretched hand; - dorsal surface undergoes compression while volar surface undergoes tension;

72
Colles Fracture Treatment
classification: - Frykman Classification - Melone Classification - Universal Classification - associated injuries: - TFCC tear - according to the report by Richards et al 1997 et, TFCC tears occurred in 53% of extra-articular distal radius fractures vs 35% of intra-articular fractures;

73
Colles Fracture Treatment

74
Colles Fracture Treatment

75
Colles Fracture Treatment
Closed reduction and immobilization in cast Stable fractures Examine for carpal tunnel syndrome before and after application Avoid palmar flexion and ulnar deviation (Cotton-Loder position) Percutaneous pinning External Fixators ORIF
 Percutaneous pinning. External Fixators. ORIF.")
76
Scaphoid fracture Diagnosis
Discussion: - surface of scapoid is largely covered by articular cartilage, & only narrow area of its neck, & even smaller distal portion, are accessible to blood vessels; - frxs across scaphoid may destroy blood supply to its proximal part; - scaphoid represents floor of anatomic snuff box; - scaphoid spans both carpal rows and therefore has less mobility than other carpals; - scaphoid is principal bony block to dorsiflexion of hand & wrist & is suscepible to frx during fall on outstretched hand; - scaphoid (navicular): the most frequently fractured carpal bone (frx occurs in tubercle, waist, or proximal 1/3); History and Exam: - fracture of the scaphoid is suspected w/ fall on an outstretched hand; Dull deep pain in the wrist after a fall onto an outstretched hand particularly if hand radially deviated. Commonly misdiagnosed as a “sprained wrist.” Most common among young men and not see often in children – the physes fails first.76
: the most frequently fractured carpal bone (frx occurs in tubercle, waist, or proximal 1/3); History and Exam: - fracture of the scaphoid is suspected w/ fall on an outstretched hand; Dull deep pain in the wrist after a fall onto an outstretched hand particularly if hand radially deviated. Commonly misdiagnosed as a sprained wrist. Most common among young men and not see often in children – the physes fails first.76.")
77
Scaphoid fracture - snuff box tenderness (see clinical differential diagnosis:) - scaphoid impaction syndrome - tenderness to palpation over scaphoid tuberosity and/or proximal pole just distal to Lister's tubercle; - limitation of wrist flexion and extension; - tenderness w/ axial compression of thumb toward the snuff box; - tenderness as pt supinates forearm against resistance; - radial & ulnar deviation results in pain on radial side of wrist; - forced dorsiflexion usually elicts significant tenderness;

78
Scaphoid Fracture Acute non-displaced, distal and horizontal
Thumb spica cast Displaced or prox, vertical fractures ORIF Increased incidence of avascular necrosis Discussion: - classification: complete fractures tend to fall into distinct categories; - about 1/9 scaphoid fractures will be incomplete; - complete fractures tend to fall into distinct categories; - tubercle frx - these fractures may often be mistaken for dorsal sulcus frx, since collapse at the frx site reduces its length on the PA film, which falsely makes it appear more distal; - transverse waist frx - proximal pole frx - dorsal sulcus frx (oblique in the plane of the dorsal sulcus): - these frx occur in the line of the dorsal sulcus (which is 45 deg to the surgical waist); - frx line starts at the dorsal apex of the ridge adjacent to the lunate and runs obliquely; - these fractures may often be mistaken for dorsal sulcus frx, since collapse at the frx site reduces its length on the PA film, which falsely makes it appear more distal; - this type of frx pattern is unstable and often leads to the humpback deformity; - any displacement that is shown at frx site indicates significant instability, making internal fixation rx of choice; - note that increased fracture obliquity is associated w/ increase scaphoid instability; - on both PA and lateral views note whether there is any carpal instability, which might represent trans-scaphoid perilunate dislocation; Determining the location, stability and orientation of the fracture predicts treatment and outcome. Distal fractures and horizontal fractures generally heal well and can be managed with immobilization in a thumb spica cast. Prox and vertical fractures have the most morbidity and require open reduction – prox portion more avascular.
: - these frx occur in the line of the dorsal sulcus (which is 45 deg to the surgical waist); - frx line starts at the dorsal apex of the ridge adjacent to the lunate and runs obliquely; - these fractures may often be mistaken for dorsal sulcus frx, since collapse at the frx site reduces its length on the PA film, which falsely makes it appear more distal; - this type of frx pattern is unstable and often leads to the humpback deformity; - any displacement that is shown at frx site indicates significant instability, making internal fixation rx of choice; - note that increased fracture obliquity is associated w/ increase scaphoid instability; - on both PA and lateral views note whether there is any carpal instability, which might represent trans-scaphoid perilunate dislocation; Determining the location, stability and orientation of the fracture predicts treatment and outcome. Distal fractures and horizontal fractures generally heal well and can be managed with immobilization in a thumb spica cast. Prox and vertical fractures have the most morbidity and require open reduction – prox portion more avascular.")
79
Prevention of Wrist Injury
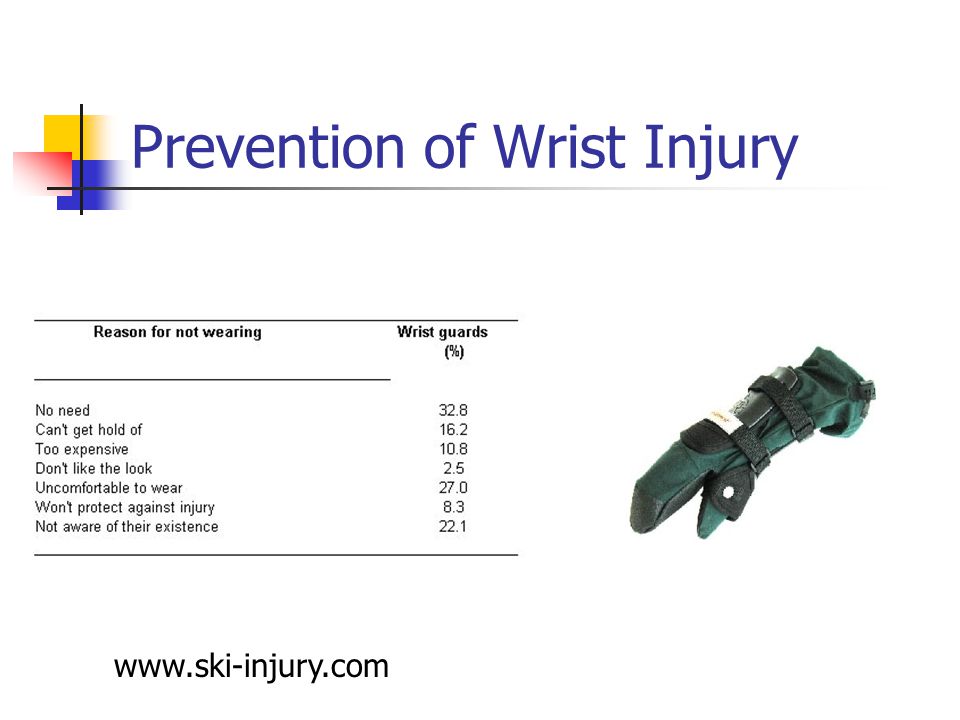
80
Wrist fracture Emergency Care
Padded splint Including the elbow is not essential in distal injuries Splint in the “position of function”, ie., fingers cupped around a gauze roll held in the palm Sling can be used to steady extremity to aid in patient comfort

81
Hand/Finger Injuries

82
Gamekeeper’s or skier’s thumb
thumb forced away like from a ski pole Disruption or sprain to the ulnar collateral ligament (MCP joint) Splint including thumb (thumb spica) Exam: - exam should begin w/ normal uninjured thumb; - note the stability of the uninjured MPJ joint as well as its ROM; - look for a supination deformity of the joint (which may be associated w/ palmar subluxation of the joint); stability: - this is generally performed in conjunction w/ x-rays; - local anesthetic block is required for patient comfort; - gamekeeper's frx is a contra-indication to stress testing (but stress testing can procede with non displaced avulsion fractures); - stability is documented w/ stress radiographs; palpation: - determine point of maximum tenderness, noting that generally the ligament tears distally off the proximal phalanx; - palpation of torn ligament ends may identify displaced collateral rupture (ie, Stener lesion); - ref: Injuries of the ulnar collateral ligament of the thumb metacarpophalangeal joint. Biomechanical and prospective clinical studies on the usefulness of valgus stress testing Discussion: - involves injury to ulnar collateral ligament of thumb MCP joint, causing instability at that joint; - the orignal description refered to a chronic injury brought on by chronic stretch of the ulnar collateral ligament; - ulnar collateral ligament nearly always separates from the base of first phalanx of the thumb; - it frequently becomes lodged between adductor pollicis aponeurosis and its its normal position (Stener Lesion); - a spectrum of ulnar instability may exist, depending on whether there is additional injury to the adductor aponeurosis, and volar plate; - Stener Lesion: - occurs when torn distal edge of collateral ligament displaces superficial and proximal to the to adductor aponeurosis; - proximal margin of aponeurosis slides distal to insertion of ligament; - creation of Stener lesion requires significant radial deviation of phalanx (? up to 60 deg) along w/ combined tears of the proper and accessory collateral ligaments inorder for the ligament to be displaced above the adductor aponeurosis; - ruptured end of ligament is no longer in contact w/ its area of insertion of the phalanx, & therefore healing can not occur; - reference: Displacement of the ruptured ulnar collateral ligament of the MP joint of the thumb: A clinical and anatomical study. B. Stener JBJS 44-B. 1962, p Gamekeeper's Fracture: - even slightly displaced Gamekeeper's fractures tend to do well with immobilization; - in the study by JE Kuz et al JHS 1999, 30 patients w/ gamekeeper's fracture were treated nonoperatively; - none of these 30 patients were dissatisfied with the outcome; - 3 patients showed instability on stress testing; - there was a 25% nonunion rate; - patients with residual symptoms tended to have larger bone fragments with greater initial rotation; - conservative indications for surgery include: frxs with more than 30% of the joint surface, and significant displacement/malrotation; - avoid stress testing of these fractures since it can lead to fracture displacement; - references: - Bony skier's thumb injuries. JB Husband and Sa McPherson. CORR. Vol 327. p Jun. - Grade III avulsion fracture repair on the UCL of the proximal joint of the thumb. RS Bovard et al. Orthopaedic Review. Vol 23(2) 1994 Feb. p Skier's thumb - the significance of bony injuries. B Hintermann et al. Am. J. Sports Med. Vol 21(6). p Nov-Dec. - Outcome of avulsion fractures of the ulnar base of the proximal phalanx of the thumb treated nonsurgically. JE Kuz MD et al. J. Hand Surg. Vol 24-A p
 Splint including thumb (thumb spica) Exam: - exam should begin w/ normal uninjured thumb; - note the stability of the uninjured MPJ joint as well as its ROM; - look for a supination deformity of the joint (which may be associated w/ palmar subluxation of the joint); stability: - this is generally performed in conjunction w/ x-rays; - local anesthetic block is required for patient comfort; - gamekeeper s frx is a contra-indication to stress testing (but stress testing can procede with non displaced avulsion fractures); - stability is documented w/ stress radiographs; palpation: - determine point of maximum tenderness, noting that generally the ligament tears distally off the proximal phalanx; - palpation of torn ligament ends may identify displaced collateral rupture (ie, Stener lesion); - ref: Injuries of the ulnar collateral ligament of the thumb metacarpophalangeal joint. Biomechanical and prospective clinical studies on the usefulness of valgus stress testing. Discussion: - involves injury to ulnar collateral ligament of thumb MCP joint, causing instability at that joint; - the orignal description refered to a chronic injury brought on by chronic stretch of the ulnar collateral ligament; - ulnar collateral ligament nearly always separates from the base of first phalanx of the thumb; - it frequently becomes lodged between adductor pollicis aponeurosis and its its normal position (Stener Lesion); - a spectrum of ulnar instability may exist, depending on whether there is additional injury to the adductor aponeurosis, and volar plate; - Stener Lesion: - occurs when torn distal edge of collateral ligament displaces superficial and proximal to the to adductor aponeurosis; - proximal margin of aponeurosis slides distal to insertion of ligament; - creation of Stener lesion requires significant radial deviation of phalanx ( up to 60 deg) along w/ combined tears of the proper and accessory collateral ligaments inorder for the ligament to be displaced above the adductor aponeurosis; - ruptured end of ligament is no longer in contact w/ its area of insertion of the phalanx, & therefore healing can not occur; - reference: Displacement of the ruptured ulnar collateral ligament of the MP joint of the thumb: A clinical and anatomical study. B. Stener JBJS 44-B. 1962, p Gamekeeper s Fracture: - even slightly displaced Gamekeeper s fractures tend to do well with immobilization; - in the study by JE Kuz et al JHS 1999, 30 patients w/ gamekeeper s fracture were treated nonoperatively; - none of these 30 patients were dissatisfied with the outcome; - 3 patients showed instability on stress testing; - there was a 25% nonunion rate; - patients with residual symptoms tended to have larger bone fragments with greater initial rotation; - conservative indications for surgery include: frxs with more than 30% of the joint surface, and significant displacement/malrotation; - avoid stress testing of these fractures since it can lead to fracture displacement; - references: - Bony skier s thumb injuries. JB Husband and Sa McPherson. CORR. Vol 327. p Jun. - Grade III avulsion fracture repair on the UCL of the proximal joint of the thumb. RS Bovard et al. Orthopaedic Review. Vol 23(2) 1994 Feb. p Skier s thumb - the significance of bony injuries. B Hintermann et al. Am. J. Sports Med. Vol 21(6). p Nov-Dec. - Outcome of avulsion fractures of the ulnar base of the proximal phalanx of the thumb treated nonsurgically. JE Kuz MD et al. J. Hand Surg. Vol 24-A p")
84
Gamekeeper’s thumb with fracture
Gamekeeper's Fracture: - even slightly displaced Gamekeeper's fractures tend to do well with immobilization; - in the study by JE Kuz et al JHS 1999, 30 patients w/ gamekeeper's fracture were treated nonoperatively; - none of these 30 patients were dissatisfied with the outcome; - 3 patients showed instability on stress testing; - there was a 25% nonunion rate; - patients with residual symptoms tended to have larger bone fragments with greater initial rotation; - conservative indications for surgery include: frxs with more than 30% of the joint surface, and significant displacement/malrotation; - avoid stress testing of these fractures since it can lead to fracture displacement;

85
Gamekeeper’s thumb Treatment
Short arm immobilizer with thumb splica Main complication is inability to heal Surgery (<2-3 weeks old) Gross radiologic instability Palpable torn ligament ends (Stener lesion) Reassessment reveal unstable joint
 Gross radiologic instability. Palpable torn ligament ends (Stener lesion) Reassessment reveal unstable joint.")
86
Conclusion Falls, collisions and direct blows cause injury to the upper extremities Humerus Elbow Wrist Hand/fingers Remember general comments “Zone of injury” Life-threatening injuries first (ABCs)
")
87
Conclusion Patients will self-splint the extremity
Internal rotation, elbow flexed, adducted to body Injuries close to joints can involve neurovascular bundle Assess CMS ARMS Appearance and alignment, radial pulse, motor and MOI, sensation

88
Conclusion Accurate assessment and rapid transport critical (60” rule)
Immobilize in the position found Sling and swathe is good immobilizer for upper extremity injuries Every patient should be advised to seek the care of a physician regardless of injury, especially if symptoms persist > 24 hrs.

89
Thank -You

90
Distal Humerus Anatomy
Medial epicondyle proximal to trochlea – attachment site for UCL and flexor/pronator ms. Lateral epicondyle proximal to capitellum – attachment site for RCL, extensor/supinator ms. Radial fossa – accommodates margin of radial head during flexion Coronoid fossa – accepts coronoid process of ulna during flexion

91
Distal Humerus – Posterior
Olecranon fossa accepts olecranon process of ulna during extension

92
Bony Alignment With elbow extended, straight line between medial/lateral epicondyles and tip of olecranon process’ With elbow flexed, isosceles triangle connects these points

93
Carrying Angle/Cubitus Valgus
Formed by long axis of humerus and midline of forearm Male norms – degrees Female norms – degrees Larger angles are considered abnormal

Similar presentations

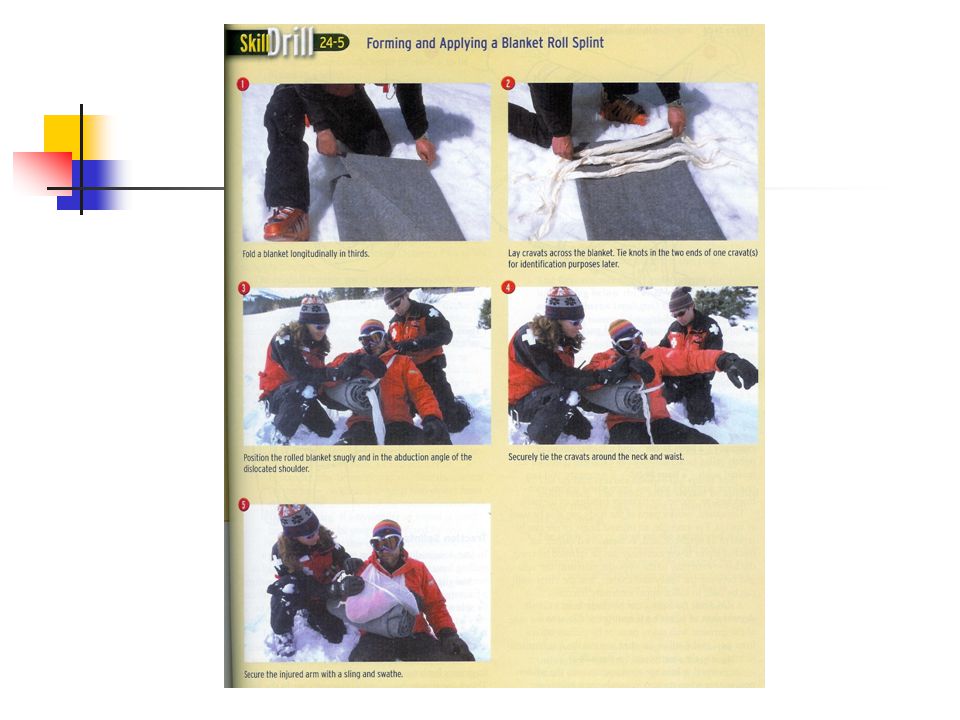
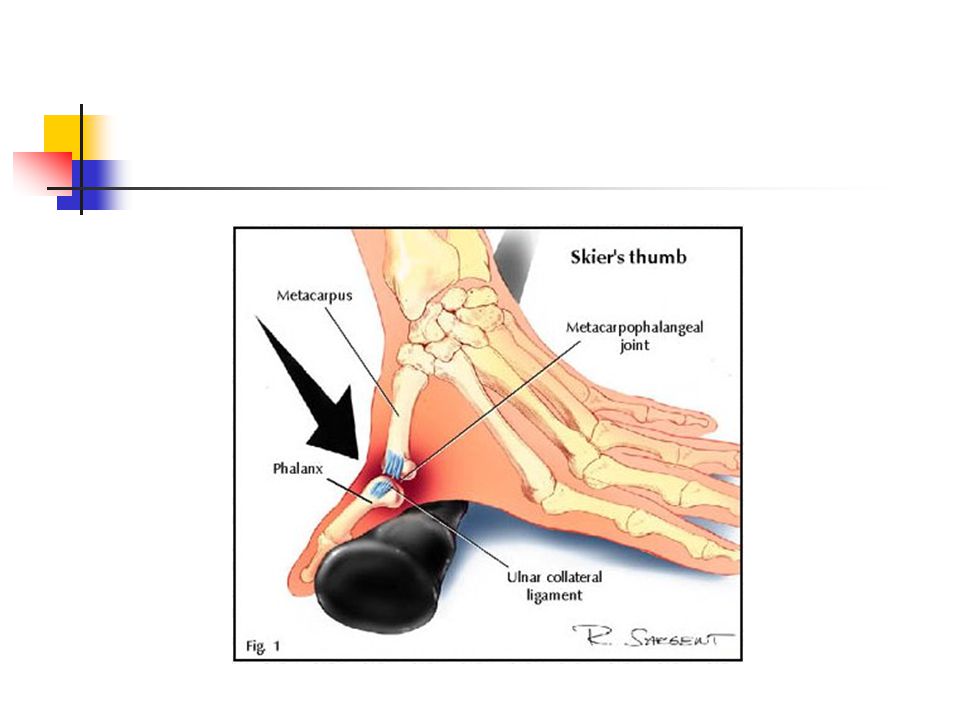












 Lecture 3 Myology of the Elbow.>")



![What am I?. What am I? Articulations of the humerus, radius, and ulna Articulations of the humerus, radius, and ulna. [ olecranon process ] Medial.](/14/4241906/big_thumb.jpg "What am I?. What am I? Articulations of the humerus, radius, and ulna Articulations of the humerus, radius, and ulna. [ olecranon process ] Medial.>")


