Download presentation
Presentation is loading. Please wait.

1
PUBERTAL DEVELOPMENT Dr Assunta Albanese St George’s Hospital London

2
FERTILITY AND FINAL HEIGHT
PUBERTY Gonadal maturation with acquisition of secondary sexual characteristics and associated growth spurt FERTILITY AND FINAL HEIGHT

3
PUBERTY Average age of onset: First signs of pubertal maturation:
11.4 years in girls 12.0 years in boys First signs of pubertal maturation: breast budding in girls increase in testicular volume in boys

4
TANNER’S STAGING OF PUBERTY IN GIRLS

6
OVARIAN REGULATION Inhibin Oestrogen Hypothalamus GnRH release
Pituitary gland FSH LH Ovary Inhibin Oestrogen

7
Breast development Libido Body composition Bone mineralization
Oestrogens produced by ovaries induce/ maintain secondary sexual characteristics and sustain germ cell production Breast development Libido Body composition Bone mineralization

8
ASSESSMENT OF OVARIAN FUNCTION
Pubertal staging Hormone levels (LH, FSH, Oestradiol, Inhibin B, progesterone) Pelvic USS
 Pelvic USS.")
9
LH, FSH and E2 and PUBERTAL STAGE in GIRLS

10
Patterns of LH secretion during pubertal development

11
DIAGNOSTIC VALUE OF PELVIC USS
Depend on experience of examiner! Size and shape of uterus and ovarian volume and appearance are a indicator of the degree of pubertal development

12
EVALUATION OF OVARIES AT USS
Shape is oval. If smaller than 1 ml prepubertal. In young adult ~6.5 ml Ovarian follicles can be detected from any age of early infancy onward Follicles increase progressively in size and number after 8.5 yrs. 3-4 small cysts (~ diameter 5 mm) normal at any age
 normal at any age.")
13
EVALUATION OF UTERUS AT USS
Shape depends on the age of child: During neonatal period and infancy drop shaped By 8 yrs tubular form During puberty pear shape Cervix to corpus ratio: 2:1 pre-puberty 1:2 post-puberty Angle between corpus and cervix only seen after puberty Endometrium thickness not seen in prepuberty

14
TANNER’S STAGING OF PUBERTY IN BOYS

16
TESTICULAR REGULATION
Hypothalamus GnRH release Pituitary gland FSH LH Testis Inhibin Testosterone (From the Sertoli cells) (From the Leyding cells)
 (From the Leyding cells)")
17
Testosterone produced by Leyding cells induces/ maintains secondary sexual characteristics and sustain germ cell production Virilization of external genitalia Phallus growth Pubic, axillary, facial hair Libido Erections/ejaculate Voice change Body composition Bone mineralization

18
ASSESSMENT OF TESTICULAR FUNCTION
Pubertal staging Hormone levels (LH, FSH, testosterone, Inhibin B) Sperm count and analysis
 Sperm count and analysis.")
19
LH, FSH and E2 and PUBERTAL STAGE in BOYS

20
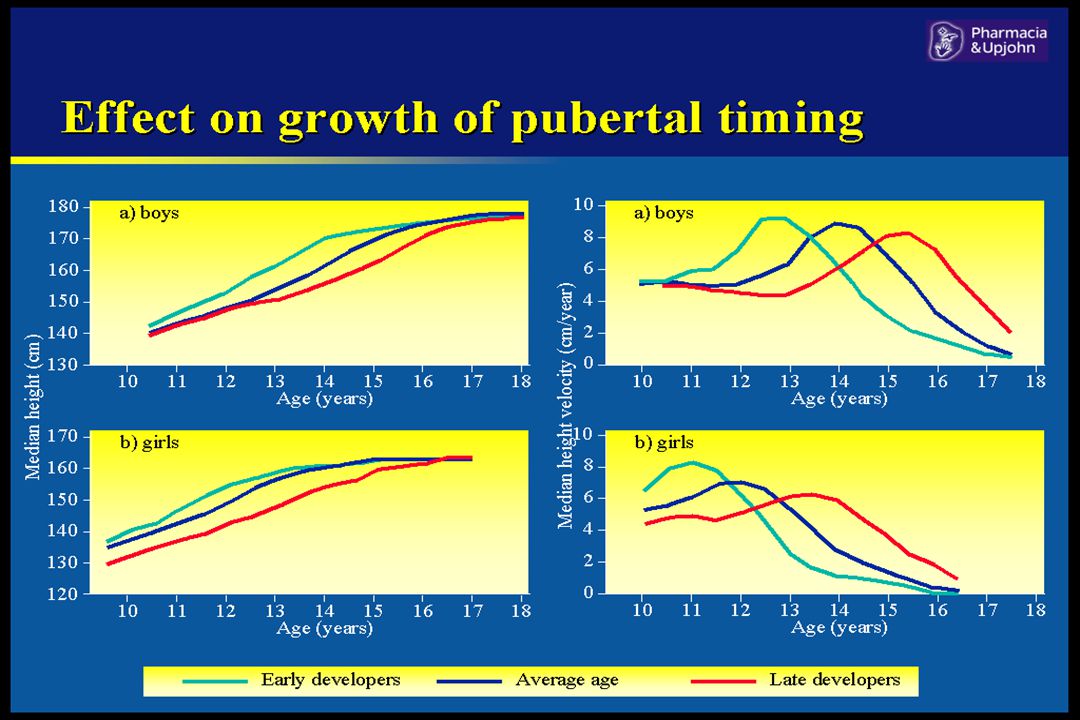
"CONSONANCE" OF PUBERTY Close relationship between secondary sexual characteristics and pubertal growth spurt In girls the pubertal growth spurt occurs early in puberty, (B2-3) In boys the pubertal growth spurt occurs late in puberty, (G3-4, 10 ml testicular volume)
 In boys the pubertal growth spurt occurs late in puberty, (G3-4, 10 ml testicular volume)")
24
DELAYED PUBERTY Onset of puberty after: 13.4 yrs in girls
13.8 yrs in boys

25
CONCERNS RAISED BY DELAYED PUBERTY
Possibly sinister underlying cause Fear that puberty will never occur Emotional and psychosocial upset of immaturity, specially when associated with short stature Long term sequelae: ? Reduced bone mineralization

26
CLASSIFICATION OF DELAYED SEXUAL MATURATION
CDGP Secondary delay: Chronic systemic illness Steroid treatment Psychosocial growth disturbance Anorexia

27
Hypogonadotrophic hypogonadism
Isolated gonadotrophin deficiency Multiple pituitary hormone deficiency Secondary to CNS tumours or cranial irradiation Hypergonadotrophic hypogonadism Klinefelter’s and Turner’s Syndromes Primary or secondary gonadal failure Dysmorphic syndromes Noonan’s syndrome, Prader-Willi, etc

28
DELAYED PUBERTY Absence of a clear pattern of pulsatile gonadotrophin secretion Pre-pubertal LH and FSH levels Development of secondary sexual characteristics Normal "Consonance" Bone age delay Final height is not impaired except if severe degree of delay

29
CONCLUSION A good understanding of normal puberty is necessary to fully assess disorders of growth and puberty The commonest disorders of precocious/delayed puberty are idiopathic Psychological disturbances is the commonest indication for intervention

30
Precocious Puberty Early Puberty Onset of puberty before:
8 yrs in girls 9 yrs in boys Early Puberty Onset of puberty between: 8 - 9 yrs in girls yrs in boys

31
CLASSIFICATION OF PRECOCIOUS SEXUAL MATURATION
Gonadotrophin-Dependent (True precocious puberty) Gonadotrophin-Independent (Pseudo precocious puberty) Variants of Precocious Sexual Maturation
 Gonadotrophin-Independent (Pseudo precocious puberty) Variants of Precocious Sexual Maturation.")
32
GONADOTROPHIN-DEPENDENT
Central precocious puberty Idiopathic Secondary to CNS abnormalities Congenital anomalies (hydrocephalus) Tumours Acquired (infections, surgery, irradiation) Primary hypothyroidism
 Tumours. Acquired (infections, surgery, irradiation) Primary hypothyroidism.")
33
CENTRAL PRECOCIOUS PUBERTY
SEXUAL DIMORPHISM Usually idiopathic in girls (90% or more) Almost always secondary to lesions in CNS in boys
 Almost always secondary to lesions in CNS in boys.")
34
GONADOTROPHIN-DEPENDENT
Pulsatile gonadotrophin secretion, especially overnight LH : FSH ratio > 1 Gonadal activation with sex steroid production Development of secondary sexual characteristics Normal "Consonance" Bone age acceleration Final height impairment

35
GONADOTROPHIN-INDEPENDENT
Adrenal disorders Tumours secreting sex steroids Congenital adrenal hyperplasia Gonadal disorders Ovarian cyst/tumours secreting sex steroids Leydig cell tumour Exogenous sex steroids McCune-Albright Syndrome Testotoxicosis

36
GONADOTROPHIN-INDEPENDENT
Sex steroid production from gonads or adrenal gland or exogenous source Suppressed LH and FSH levels Secondary sexual characteristics or virilization Growth acceleration Bone age acceleration with final height impairment

37
McCune - Albright Syndrome
Fibrous dysplasia of skull and long bone "Cafe-au lait" patches with serrated edges Autonomous endocrine overactivity : Precocious puberty Hyperthyroidism Hypercortisolism Pituitary adenomas secreting GH/ PRL Hyperparathyroidism

38
McCune - Albright Syndrome
Precious puberty mainly described in girls First phase: intermittent periods of breast development and vaginal bleeding (gonadotrophin independent) Second phase: Central precocious puberty (gonadotrophin dependent)
 Second phase: Central precocious puberty (gonadotrophin dependent)")
39
McCune - Albright Syndrome
Gene mutation for the a-subunit of the G protein, which stimulate cAMP formation Activation of receptors that operate with a cAMP-dependent mechanism The somatic mutation occurs early in embriogenesis

40
TESTOTOXICOSIS Occurs in boys, familiar, Autosomic Dominant
Normal "Consonance" Extreme degree of virilization compared to the testicular enlargement Prepubertal values of FSH and LH Failure to respond to GnRH analogue treatment Due to a mutation of LH receptor with constant activation of the G protein even without ligand

41
VARIANTS OF PRECOCIOUS SEXUAL MATURATION
Isolated premature thelarche Isolated menarche Premature adrenarche Unclassified forms

42
ISOLATED PREMATURE THELARCHE
Isolated cyclic breast enlargement, usually < 2 yrs old Absence of other signs of puberty Absence of behavioural problems Normal growth and bone maturation Predominant FSH pulsatility Development of follicular ovarian cysts

44
PREMATURE PUBARCHE Usually begins at around 6-8 years of age
Early appearance of pubic hair, with or without axillary hair Puberty usually occurs at a normal time Slight growth spurt and advance in bone maturation Final height prognosis is not compromised

45
PREMATURE PUBARCHE Increased adrenal production of sex hormones Gonadotrophin secretion is prepubertal Clitoral virilization in girls and phallic enlargement in boys together with excessive bone age maturation should suggest excessive production of sex hormones due to CAH or an adrenal tumour

46
DELAYED PUBERTY Onset of puberty after: 13.4 yrs in girls
13.8 yrs in boys

47
CONCERNS RAISED BY DELAYED PUBERTY
Possibly sinister underlying cause Fear that puberty will never occur Emotional and psychosocial upset of immaturity, specially when associated with short stature Long term sequelae: ? Reduced bone mineralization

48
CLASSIFICATION OF DELAYED SEXUAL MATURATION
CDGP Secondary delay: Chronic systemic illness Steroid treatment Psychosocial growth disturbance Anorexia

49
Hypogonadotrophic hypogonadism
Isolated gonadotrophin deficiency Multiple pituitary hormone deficiency Secondary to CNS tumours or cranial irradiation Hypergonadotrophic hypogonadism Klinefelter’s and Turner’s Syndromes Primary or secondary gonadal failure Dysmorphic syndromes Noonan’s syndrome, Prader-Willi, etc

50
DELAYED PUBERTY Absence of a clear pattern of pulsatile gonadotrophin secretion Pre-pubertal LH and FSH levels Development of secondary sexual characteristics Normal "Consonance" Bone age delay Final height is not impaired except if severe degree of delay

51
CONCLUSION A good understanding of normal puberty is necessary to fully assess disorders of growth and puberty The commonest disorders of precocious/delayed puberty are idiopathic Psychological disturbances is the commonest indication for intervention

Similar presentations