Download presentation
Presentation is loading. Please wait.

1
Section A: Applied Anatomy and Physiology
11. Structure and function of the respiratory system

2
Syllabus Structure of the nasal passages, trachea, bronchii, bronchioles, and alveoli Lobes of the lung and pleural membrane Mechanics of breathing at rest and during exercise Respiratory muscles, to include: diaphragm, external intercostals, sternocleidomastoid, pectoralis minor, internal intercostals, and abdominal muscles Control of ventilation Definitions, values and measurement of respiratory volumes at rest and during exercise Effect of exercise on respiratory volumes and pulmonary ventilation Gaseous exchange, partial pressures and tissue respiration The effect of altitude on the respiratory system

3
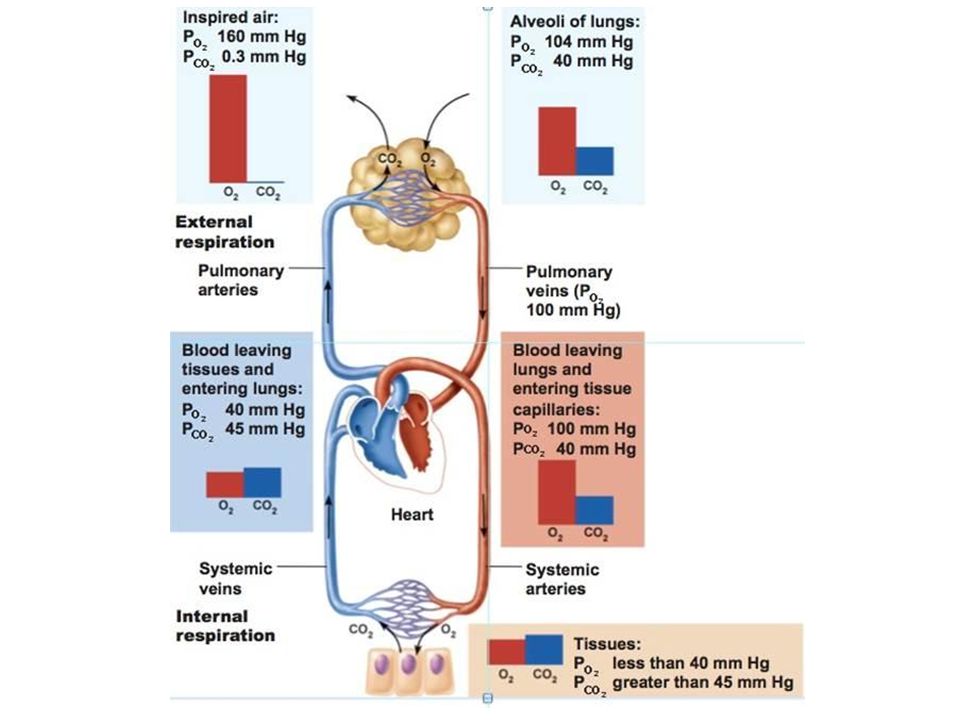
External Respiration Involves the movement of gases into and out of the lungs. The exchange of gases between the lungs and blood is known as pulmonary diffusion.

4
Nasal Passages Nasal cavity is divided by a cartilaginous septum that forms the passages. Interior structures aid the process by: Mucous membranes and blood capillaries moisten and warm the inspired air Ciliated epithelium filters and traps dust particles Small bones (chonchae) increase the surface area to improve efficiency
 increase the surface area to improve efficiency.")
5
Oral Pharynx and Larynx
Air entering the larynx passes over the vocal chords and into the trachea Swallowing – the larynx is drawn upwards and forwards against the base of the epiglottis (preventing entry of food)
")
7
Trachea Approx. 10cm in length and lies in front of the oesophagus.
Composed of 18 ‘rings’ of cartilage, which are also lined by a mucous membrane and ciliated cells. Extends from larynx and directs air into the right and left primary bronchi.

11
Bronchi and Bronchioles
Trachea divides into right and left bronchi, which further subdivide into lobar bronchi Three feeding the lobes of the right lung Two feeding the lobes of the left lung Further subdivision of these form bronchioles Bronchioles enable the air to pass into the alveoli via the alveolar ducts

12
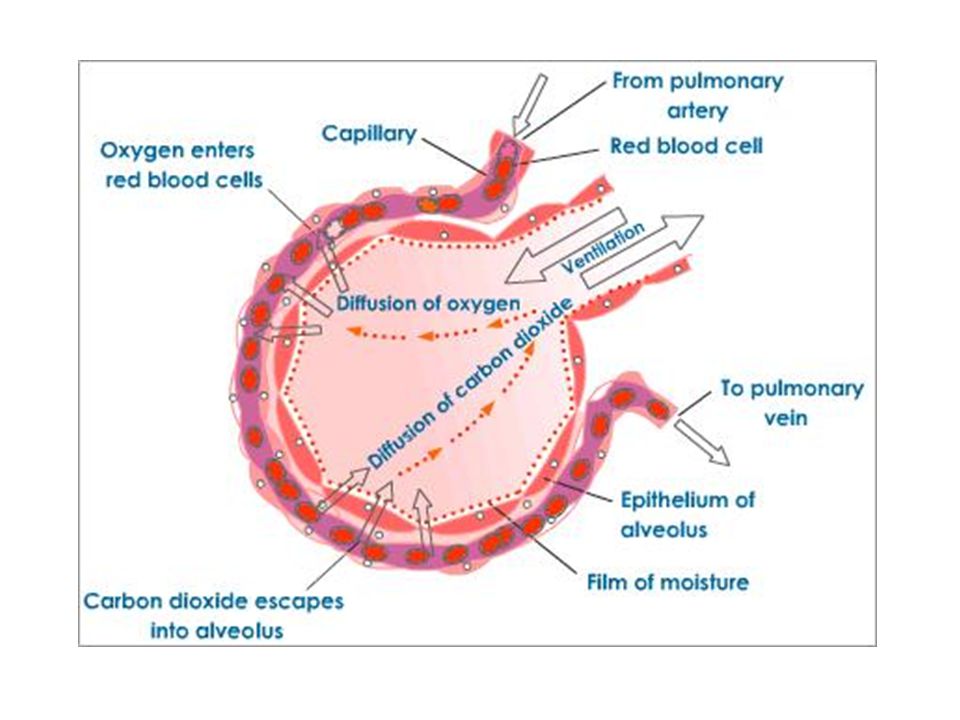
Alveoli Responsible for the exchange of gases between the lungs and the blood The alveolar wall are extremely thin, are lined by a film of water Essential for dissolving oxygen from inspired air Alveoli walls also contain elastic fibres further increasing surface area Surrounding each alveolus is an extensive capillary network

15
Mechanics of Breathing

18
Breathing Lungs are surrounded by pleural sacs containing pleural fluid, which reduces friction Sacs are attached to both the lungs and the thoracic cage, which enables the lungs to inflate and deflate as the chest expands and flattens

20
Inspiration Active Occurs as a result of contraction of;
External intercostals Diaphragm As the chest expands through these muscular contractions, the surface tension created by the film of pleural fluid causes the lungs to be pulled outwards

21
Inspiration During Exercise
Additional muscles; Sternocleidomastoid Scalenes Pectoralis major

22
Expiration Generally a passive process
During exercise, the process becomes more active; The internal intercostals Abdominals Latissimus dorsi

25
Respiratory Regulation
Controlled by nervous system Basic rhythm is governed and co-ordinated by the respiratory centre (medulla) Inspiration generally lasts up to 2 seconds after which impulses cease and expiration occurs by elastic recoil of lungs
 Inspiration generally lasts up to 2 seconds after which impulses cease and expiration occurs by elastic recoil of lungs.")
26
Factors Controlling Rate of Breathing
Chemoreceptors CO2 levels Proprioceptors and Mechanoreceptors Stretch receptors Hering-Breur reflex (prevents overinflation) Thermoreceptors Temperature of blood Baroreceptors State of lung inflation
 Thermoreceptors. Temperature of blood. Baroreceptors. State of lung inflation.")
27
Neural Control The respiratory centre in the medulla of the brain controls breathing. It is made up of two main areas: The inspiratory centre is responsible for the rhythmic cycle of inspiration and expiration The expiratory centre is inactive during quiet ventilation. When the rate and depth of breathing increases (detected by stretch receptors in the lungs) the expiratory centre inhibits the inspiratory centre and stimulates expiratory muscles.
 the expiratory centre inhibits the inspiratory centre and stimulates expiratory muscles.")
29
Cont. In most circumstances the neural control of breathing is involuntary The resp centre sends out impulses via the phrenic and intercostal nerves to the respiratory muscles The muscles are stimulated for a short period, causing insipration Then when the stimulus stops, expiration occurs

30
Other factors influencing the neural control of breathing include:
A large drop in oxygen tension. This is monitored by chemoreceptors in the aorta and carotid arteries and results in an increase in the rate and depth of breathing. A rise in blood pressure, monitored by baroreceptors in the aorta and carotid arteries, resulting in a decrease in ventilation rate Proprioceptors in the muscles responding to movement stimulate the respiratory centre, increasing the rate and depth of breathing The respiratory centre can also be affected by higher centres in the brain, e.g. emotional influences

31
Chemical Control The respiratory centre responds mainly to changes in the chemistry and temperature of the blood The most significant factor is a lowering in pH This occurs when there is an increase in the amount of CO2 being produced by the cells The increase is detected by the respiratory centre (in the brain) It results in an increase in the rate and depth of breathing A rise in body temperature will cause an increase in the rate but not the depth of breathing
 It results in an increase in the rate and depth of breathing. A rise in body temperature will cause an increase in the rate but not the depth of breathing.")
32
Reminder Pulmonary diffusion – gaseous exchange at the lungs
Its functions Replenish oxygen Remove carbon dioxide

33
Partial Pressure of Gases
Central to understanding of gaseous exchange is the concept of partial pressure “the individual pressure that the gas exerts when it occurs in a mixture of gases” The pressure is proportional to its concentration Partial pressures added together = total pressure of gas

34
Composition of Air Nitrogen = 79% Oxygen = 20.9%
Carbon dioxide = 0.03% The percentages are obviously the relative concentrations!

35
Calculating Partial Pressure

38
Effect of Altitude

39
Effect of Altitude With altitude there is a decrease in atmospheric pressure BUT the percentages of gases within the air remain identical to those found at sea level It is the partial pressure of the gases that changes in direct proportion to an increase in altitude

40
Effect of Altitude cont.
E.G. – at rest the pO2 of arterial blood is approx 100mmHg, while in the resting muscles and tissues it is 40mmHg. The difference between the two indicates the pressure gradient. The pO2 of arterial blood at an altitude of 8000ft drops to 60mmHg, while that in the muscles remains at 40mmHg!

41
Altitude Training The principle:
With an increase in altitude, the partial pressure of oxygen in the atmosphere decreases by about a half, causing the body to adapt by INCREASING RED BLOOD CELL MASS AND HAEMOGLOBIN LEVELS to cope with a lower pO2

42
Altitude Training It is widely used by endurance athletes to enhance their oxygen-carrying capacity Recent evidence: Living at altitude and training at sea level produces the greatest endurance performance Can increase the oxygen-carrying capacity of the blood by up to 150%

43
Altitude Training Disadvantages: Expensive Can cause altitude sickness
Due to lack of oxygen , training at higher intensities is difficult Any benefits are soon lost on return to sea level

44
Oxyhaemoglobin Dissociation Curve

45
Transport of Oxygen Each molecule of haemoglobin can combine with 4 molecules of oxygen The amount of oxygen that can combine with haemoglobin is determined by the partial pressure of oxygen High pO2 = complete saturation Low pO2 = saturation decreases

46
Transport of Oxygen and Dissociation
Hb is totally saturated at the lungs (alveoli) As the pO2 is reduced, Hb saturation decreases accordingly. This is largely due to the increased acidity of the blood (decrease in blood pH), caused by an increase in CO2 or LA and the increase in body temperature, which causes a shift to the right in the haemoglobin saturation curve.
 As the pO2 is reduced, Hb saturation decreases accordingly. This is largely due to the increased acidity of the blood (decrease in blood pH), caused by an increase in CO2 or LA and the increase in body temperature, which causes a shift to the right in the haemoglobin saturation curve.")
47
The Release of Oxygen from Haemoglobin
At rest The pO2 in the alveoli is approx 100mmHg 100% saturation In resting muscle and tissue the pO2 is 40mmHg 75% saturation Means that 25% of the oxygen picked up at the lungs is released into the muscle to help in energy production

48
The Release of Oxygen from Haemoglobin
During exercise The pO2 in the alveoli remains at approx 100mmHg 100% saturation In working muscles the pO2 can be greatly reduced, up to 15mmHg 25% saturation Means that 75% of the oxygen picked up at the lungs is released into the muscle to help meet the extra energy demands

49
The Bohr Shift Increased oxygen released to tissues!

50
Gas Exchange at Muscles and Tissues
High pO2 in arterial blood and relatively low pO2 in muscles causes a pressure gradient High pCO2 in tissues and low pCO2 in arterial blood causes a movement of CO2 in opposite direction Production of CO2 stimulates the dissociation of oxygen from haemoglobin Myoglobin has a much higher affinity for oxygen than haemoglobin

51
a-VO2 difference The arterial-venous oxygen difference is the difference in oxygen content of the blood in the arteries and the veins. It is a measure of the amount of oxygen consumed by the muscles

52
Lung Volumes LUNG VOLUME DEFINITION TYPICAL REST VALUE
CHANGE DURING EXERCISE Tidal volume (TV) Volume inspired or expired per breath 500ml Increase Inspiratory reserve volume Maximal volume inspired following end of resting inspiration 3100ml Decrease Expiratory reserve volume Maximal volume expired following end of resting expiration 1200ml Residual volume (RV) Volume of air remaining in the lungs at the end of maximal expiration Remains the same
 Volume inspired or expired per breath. 500ml. Increase. Inspiratory reserve volume. Maximal volume inspired following end of resting inspiration. 3100ml. Decrease. Expiratory reserve volume. Maximal volume expired following end of resting expiration. 1200ml. Residual volume (RV) Volume of air remaining in the lungs at the end of maximal expiration. Remains the same.")
53
Lung Capacities LUNG CAPACITIES DEFINITION TYPICAL REST VALUE
CHANGES DURING EXERCISE Inspiratory capacity (TV + IRV) Maximum volume of air inspired from resting expiratory levels 3600ml Increase Vital capacity (TV + IRV + ERV) The maximum volume forcibly expired following maximal inspiration 5000ml Slight decrease Total lung capacity (VC + RV) The volume of air that is in the lungs following maximal inspiration 6000ml Minute ventilation (TV * f) The volume of air inspired or expired per minute 7500ml Dramatic increase
 Maximum volume of air inspired from resting expiratory levels. 3600ml. Increase. Vital capacity (TV + IRV + ERV) The maximum volume forcibly expired following maximal inspiration. 5000ml. Slight decrease. Total lung capacity (VC + RV) The volume of air that is in the lungs following maximal inspiration. 6000ml. Minute ventilation (TV * f) The volume of air inspired or expired per minute. 7500ml. Dramatic increase.")
55
Minute Ventilation TIDAL VOLUME (TV) * FREQUENCY (BREATHS/MIN)
REST 500ml * 15 = 7.5L / min MAXIMAL WORK 4,000ml * 50 = 200L / min

56
Adaptive Responses of Respiratory System to Training
SMALL INCREASES IN LUNG VOLUMES Result from increased strength in respiratory muscles IMPROVED TRANSPORT OF RESPIRATORY GASES Increased amount of RBC’s (haemoglobin) Increased blood plasma reduces viscosity ENHANCED GASEOUS EXCHANGE AT THE ALVEOLI AND TISSUES Increased capillary density GREATER UPTAKE OF OXYGEN BY THE MUSCLES Increased myoglobin and mitochondrial density Increase in a-VO2 difference
 Increased blood plasma reduces viscosity. ENHANCED GASEOUS EXCHANGE AT THE ALVEOLI AND TISSUES. Increased capillary density. GREATER UPTAKE OF OXYGEN BY THE MUSCLES. Increased myoglobin and mitochondrial density. Increase in a-VO2 difference.")
Similar presentations
























 bronchioles.>")







