Download presentation
Presentation is loading. Please wait.

1
Musculoskeletal Diseases and Disorders: Knee and Patella
PTP 521

2
Fractures Knee Ottawa Rules
A knee x-ray is only required for knee injury patients with any of these findings: age 55 or over isolated tenderness of the patella (no bone tenderness of the knee other than the patella) tenderness at the head of the fibula inability to flex to 90 degrees inability to weight bear both immediately and in the casualty department (4 steps - unable to transfer weight twice onto each lower limb regardless of limping).
 tenderness at the head of the fibula. inability to flex to 90 degrees. inability to weight bear both immediately and in the casualty department (4 steps - unable to transfer weight twice onto each lower limb regardless of limping).")
3
FRACTURES OF THE KNEE AND PATELLA
Fractures of the Distal Femur Classified by location Supracondylar: occur superior to the femoral condyles. Common patterns are comminuted, impaction, linear, with or without displacement

4
Intercondylar: Occurs between the medial and lateral femoral condyles.
Fracture pattern is commonly called a "Y" fracture. Condyles split apart from each other and from the shaft of the femur.

5
Condylar Usually linear and involves only one femoral condyle
Sartoris, Adductors,

6
Fractures of the Proximal Tibia
Most frequent occurrence is at the medial and Lateral tibial plateaus with the lateral plateau most often involved. -difficult to see and treat. Mechanism of injury is a varus or valgus force combined with axial compression. Generally considered to be impaction fractures.

7
Because of the difficulty in viewing the tibial plateau, conventional tomography is
needed in addition to the routine x-rays. A classification system has been developed to identify the 6 most common fracture patterns.

8
Tibial Plateau Fractures
Two systems: book has the Hohl system highlighted very well. Second system is the scharzker method. The web site above has a great representation of the Scharzker classification with a unique way of viewing the CT scans. The cursor can move over the radiograph and the picture below shows the corresponding CT view. These two systems are not very different. Hohl and Scharzker = need to recognize that they are tibial plateau fractures, but then can go look up. Higher they go the more rehab needed, as they get worse.

9
Comparison Hohl Classification Schatzker Classification
Same as Hohl Type I Type III Type II Same as Hohl Type IV Same as Hohl Type V Same as Hohl Type VI Type I Type II Type III Type IV Type V Type VI Main difference between the two classifications is the placement of Type II and Type III which are switched in the two classification types. Be sure you see which classification is being used when dealing with a tibial plateau fracture to understand the bone dysfunction.

10
Hohl System Hohl Type I: nondisplaced vertical split fracture of the lateral tibial plateau caused by a pure valgus force Schatzker Type I: Pure split on lateral side

11
Hohl Type II: a local depression of the lateral tibial plateau caused by a combination of axial and valgus forces Schatzker Type III: Pure central depression - Lateral condyle

12
Hohl Type III: a displaced vertical split fracture with depression at the lateral plateau, caused by a combination of valgus and axial forces and often associated with a proximal fibula fracture. Schatzker Type II: Split with lateral depression

13
Hohl Type IV: a displaced depressed fracture of the medial plateau, caused by varus and axial forces
Schatzker Type IV: fractures of medial condyle

14
Type V: a vertical split fracture of the anterior or posterior aspect of the tibial plateau, caused by axial forces Schatzker Type V: Bicondylar fractures Continuity of metaphysis & diaphysis maintained

15
Hohl Type VI: a displaced, comminuted fracture of both condyles, caused by axial forces, often associated with proximal fibula fractures Schatzker Type VI: Dissociation of metaphysis & diaphysis in addition to plateau

16
Fractures of the Patella
MOI: direct trauma from falls or blows or indirect trauma from tension forces. -change in force, action of muscle. Direct trauma: Patella fractures as it compresses against the femur. Most frequent pattern is a transverse linear fracture line through the mid-region of the bone. Vertically oriented fractures and comminution are also seen. Avulsion fractures of the patella occur as a result of indirect trauma

17
Patellar Fracture Patterns

18
Patella Fractures Patella fractures Lateral view AP view Sunrise view
Patella Alta Avulsion fracture of patella ligament

19
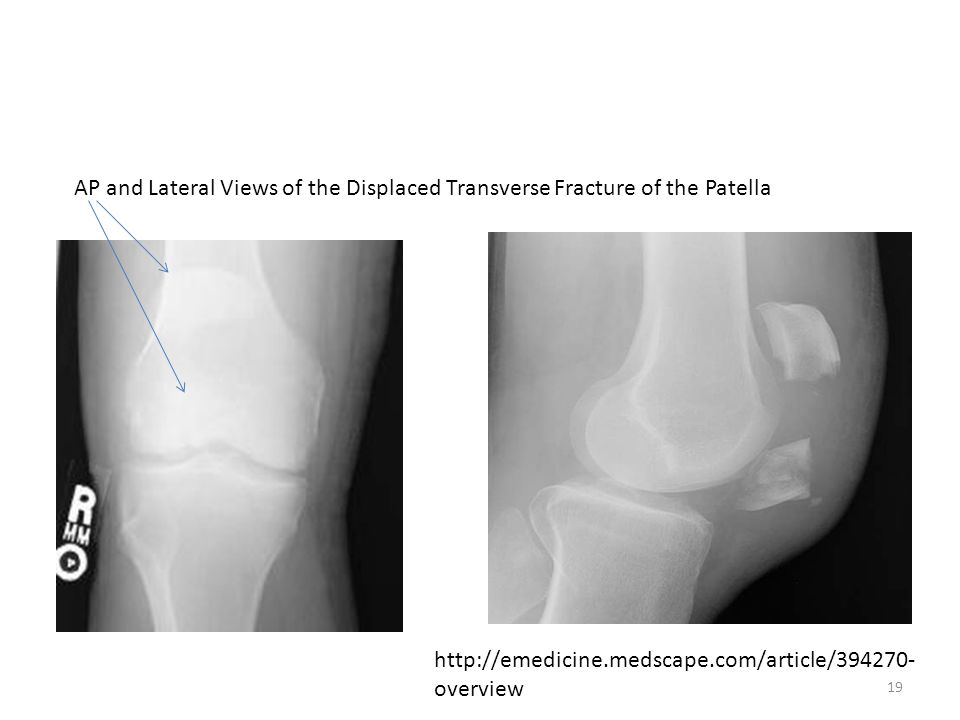
AP and Lateral Views of the Displaced Transverse Fracture of the Patella
20
Sunrise view: MRI On the left is a patella dislocation, high signal intensity on
the lateral side View on the right is a bipartite patella. Can be confused with a fractured patella

21
Full thickness fissure of the patella articular cartilage

22
Joint effusion Transverse View, fast spin echo T2-weighted fat saturated MR Normal cartilage with joint effusion surrounding it

23
Joint Dysfunctions of the Knee
Rheumatoid Arthritis: discussed under wrist and hand Rheumatoid arthritis. Anteroposterior knee radiograph shows diffuse uniform joint space narrowing. Bone on Bone, uniform narrowing. Jacobson J A et al. Radiology 2008;248:

24
Osteochondritis Dessicans
Definition: avascular necrosis of the condylar epiphysis of the femur Medial femoral condyle involved in 75% of the cases, lateral condyle can also be affected, results in a osteochondral fracture

25
Etiology: traumatic Caused by impingement of the tibial spine on the femoral condyle Or a loss of circulation to the osseous tissue of the epiphyseal plate Or an avulsion of the proximal attachment of the PCL

26
SX: Signs: aching pain in the knee at rest
worse with weight bearing activities insidious onset episodes of knee joint locking Signs: antalgic gait pattern knee joint effusion restriction in range of motion present

27
Radiographs: AP, lateral, and tunnel will show a lesion that appears like a half moon defect on the subchondral bone RX: Decrease or elimination of WB with immobilization

28
Osteonecrosis: Avascular necrosis of the knee occurring in adults,
Typically women age 50 years or more. Medial compartment of the knee and femoral condyle more involved than tibial condyle.

29
Osteoarthritis. Osteoarthritis: joint space narrowing, sclerosis, and osteophyte formation (arrow) predominately involving the medial compartment. OA, more narrowing on one side, and osteophyte formation. Indications: uneven narrowing, osteophyte RA: uniform diminished joint space. Jacobson J A et al. Radiology 2008;248: ©2008 by Radiological Society of North America

30
DJD/OA of the knee Standing AP view of the knee’s
Weight Bearing Important. Typical finding is sharpening of the tibial spines Narrowing of the medial compartment

31
This view shows osteophyte formation on the tibial plateau, medial side
Narrowing of both the medial and lateral compartments, but more on the medial. More advanced OA

32
Patello Femoral OA seen in a lateral view
Patellofemoral compartment narrowing Osteophyte formation on both the superior and inferior aspect of the patella Try bending this knee Patella will have more pain in flexion (stairs) , but relief in extension
 , but relief in extension.")
33
Surgeries: High Tibial Ostotomy
Occurs in patients with unicompartmental osteoarthritis. Usually the medial compartment with a varus deformity noted. New but effective. Patients age is usually under 65 years of age, generally exclude patients with RA or other systemic diseases

34
Indications for Tibial Osteotomy
Best results occur in patients under 50 years of age Body mass index greater than 25 kg per square meter? Isolated medial compartment OA, No lateral thrust at the knee, A varus deformity less than 10 dg Range of motion greater than dg Steve Iserman

35
Contradictions Inflammatory arthritis: RA, Sceriatic Arthritis
Significant ligamentous instability Age greater than 70years Severe patellofemoral arthritis Flexion contracture greater than 15 dg Won’t get good contact, so bone won’t heal properly. Varus deformity greater than 15 dg

36
Technique: wedge resection
Lateral is lower, so more weight bearing on that lateral side..

37
Goal of Surgery: Realign the weight bearing axis so that the pressure on the tibial plateau is shifted laterally into the area of the intercondylar eminence and the tibial spines rather than the medial condyle

38
Unicompartmental replacement
Replace only one part of the knee but maintain the natural joint/bony surfaces on the other part. Used when ACL surgery fails Generally will replace the medial compartment. To function successfully, the anterior cruciate ligament needs to remain intact

39
Total Knee Replacement
Indications: a. Chronically disabling degenerative knee pain b. Failed conservative measures Contradictions: a. Acute infection elsewhere in body b. Charcot arthropathy or absence of sensation in the joint c. Infection within the joint d. Severe spasticity associated with contractures.

40
Relative contra indications
a. Severely demented or bedridden patients (unless needed for transfers) b. Osteoporosis (depends on bone density of femur and tibia) c. Significant peripheral vascular disease (if it won’t heal)
 b. Osteoporosis (depends on bone density of femur and tibia) c. Significant peripheral vascular disease (if it won’t heal)")
41
Prosthetic Devices Classified as constrained, semi-constrained, or minimally constrained constrained: actually hinges, knee doesn't function as a simple hinge though and these prostheses have a high failure rate, reserved for the patients with severe instability problems or severe deformities

42
Semi-constrained Posterior cruciate ligament is absent or taken out as a result of the surgery. This is designed to prevent subluxation or dislocation of the tibiofemoral joint resulting from the absence of the ligaments.

43
Advantages and Disadvantages of the Preserving the PCL
restores more normal knee kinematics more normal stair climbing abilities Disadvantages excessive rollback of femur on tibia if PCL is too tight difficult to reproduce the preoperative joint line ligament length more difficult to balance with the collateral ligaments more difficult to correct large flexion contractures

44
Minimal constrained: Reproduces the anatomical contours of the knee
Relies heavily on soft tissue to provide joint stability Usually done with younger individuals, so can freely do activities.

45
Surgical Preparation

46
TKR Rehab: “joint camp”
Goal of a TKR is to provide patient with a stable, pain-free knee joint with a functional range of motion -Usually there for 4 days or less. Postoperative Problems: knee stiffness which can lead to adhesions=work on flexion. Functional considerations: need at least 90 dg of flexion to be able to do most ADL's and greater than 90 dg's is needed to go from a sitting to a standing position.

47
Patellofemoral Dysfunctions:
Patella Instabilities Patella Dislocation: associated with an excessive lateral pull of the vastus lateralis and IT band MOI: acute trauma or twisting force with a combination of flexing femur, externally rotating femur while foot is planted

48
Subluxation of the Patella: same mechanisms as a dislocation
Patella should mirror the condylar divot. Shifted slightly like seen is a subluxation. Over more would be a dislocation.

49
Factors which predispose a patient to subluxation or dislocation:
1) Q angle greater than 20 dg 2) Excessive external rotation of tibia (in prone) 3) Increased internal rotation of the femur (stand behind and look at medial hamstrings coming at you that’s IR of femur) 4) Patella alta –(high patella) considered most important, tape measure=if length of patella is shorter than distance from the posterior apex to tibia tuberosity. 5) Shallow trochlear groove 6) Small flat patella 7) Atrophy of vastus medialis (hold patella, then do a quad set, see where it is pulled, usually lateral) 8) Muscle imbalance/weakness relative to the vastus lateralis
 Q angle greater than 20 dg. 2) Excessive external rotation of tibia (in prone) 3) Increased internal rotation of the femur (stand behind and look at medial hamstrings coming at you that’s IR of femur) 4) Patella alta –(high patella) considered most important, tape measure=if length of patella is shorter than distance from the posterior apex to tibia tuberosity. 5) Shallow trochlear groove. 6) Small flat patella. 7) Atrophy of vastus medialis (hold patella, then do a quad set, see where it is pulled, usually lateral) 8) Muscle imbalance/weakness relative to. the vastus lateralis.")
50
SX and Signs SX: Signs: onset occurs with sudden activity valgus
external rotation force Signs: Hemarthrosis -bleeding into joint. tenderness to palpate apprehension to lateral patella joint movement

51
Chondromalacia Patella
Patellofemoral tracking dysfunctions: new term (to make it seem less chronic) Progressive softening, fibrillation and finally degeneration of the articular cartilage on the underside of the patella -Seen with younger girls (13-15) Overuse syndrome with altered patellar biomechanics occurring.
 Progressive softening, fibrillation and finally degeneration of the articular cartilage on the underside of the patella. -Seen with younger girls (13-15) Overuse syndrome with altered patellar biomechanics occurring.")
52
Chondromalacia= SX: retropatellar pain described as aching with sitting. Signs: + movie goers sign (forced into full knee flexion for a long period of time), + full knee flexion test (takes 30 to 60 seconds for achy pain to start)
, + full knee flexion test (takes 30 to 60 seconds for achy pain to start)")
53
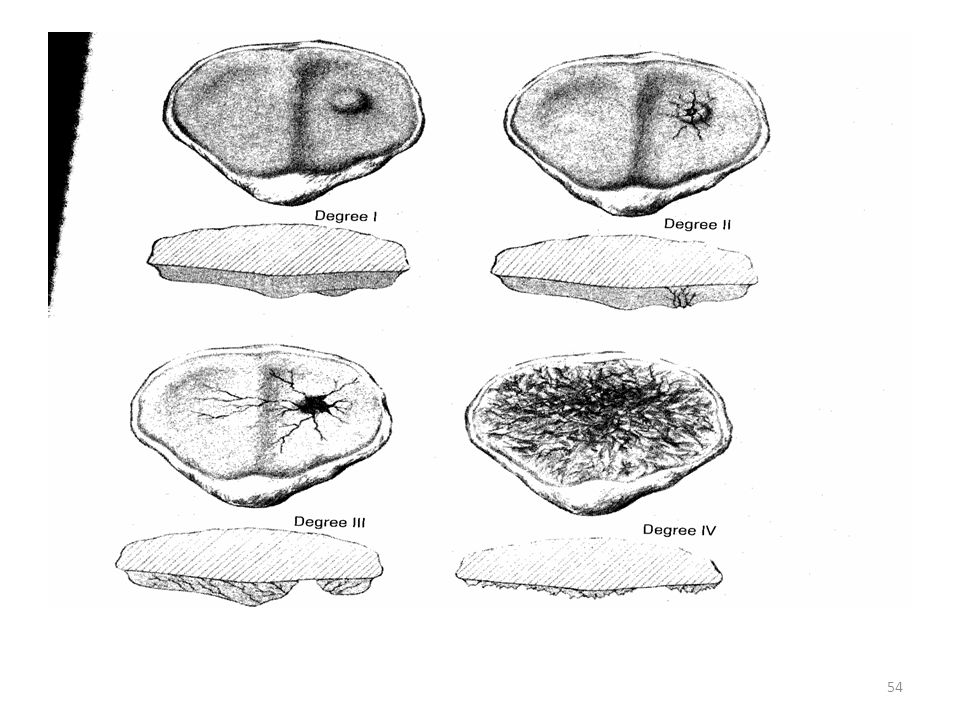
Stages: I - IV I: swelling and softening of the cartilage
II: fissuring w/in the softened areas III: fasciclations of articular cartilage almost to level of subchondral bone IV: destruction of cartilage w/ subchondral bone exposed Histologically Stage IV is virtually indistinguishable from DJD

55
Larsen-Johansson's Disease
Necrosis of the patella poles occurs in children 8-13 years of age etiology unkown, insidious onset

56
SX and Signs SX: pain with resisted extension of the knee, pain with kneeling, pain with activity Signs: swelling and tenderness to palpation over the inferior pole of the patella X-ray: may or may not show fragmentation of the bone near the affected pole

57
Musculotendinous Dysfunctions of the Knee
Osgood Schlatter's Disease: Tibial Apophysisitis -inflammation of the tibial tuberosity, which goes bone growth. Develops when the epiphysis undergoes the transition from cartilage to bone. Develops in the patella tendon/bone insertion -more cosmetic, then chronic pain.

58
Osgood Schlatters Disease
Traction on the patella ligament results in microfractures. The body tries to heal itself and an outgrowth of the tibial tuberosity occurs. Occurs in males more than females, ages 12-14 During a growth period Differential Diagnosis: Mechanical dysfunction, mimics patellar tendonitis or patellofemoral pain syndrome

59
SX and Signs Sx: Signs: pain in the region of the tibial tubercle
related to activity particularly sports pain relieved by rest hurts to kneel Signs: swelling over the tibial tubercle tenderness to palpation over the tibial tubercle

60
Radiographs: lateral view may show irregular ossification or fragmentation of the tibial tubercle
RX: Rest, may try bracing to give patella tendon some assist Avoid resisted knee extension activities until the pain has gone away. Time is usually 6-8 weeks, may cast Surgery – rare *Issue how to keep kid from running and jumping when pain in minimum.

61
Tendonitis Patella tendonitis or jumper's knee: SX: Signs:
pain during activity, pain after activity, pain with sitting for a long period of time tenderness noted at inferior pole of patella Signs: tenderness to palpation, pain with resisted knee extension swelling over the patella tendon region pain with passive stretch

62
Quadriceps Tendonitis
Superior pole of the patella at the tendon junction. Occurs in sports that require a lot of running and jumping or acceleration - deceleration activities like soccer or basketball SX: pain during activity pain after activity Signs: tenderness to palpate over the superior pole of the patella pain with resisted knee extension pain with passive stretch of the quadriceps

63
Iliotibial Tract Tendonitis
Friction between the underlying structures and the iliotibial tract, occurs in runners or patients whose occupation or hobbies lead to a tight iliotibial tract. SX: pain with activity pain over the lateral thigh closer to the knee Signs: + Ober's test pain with resisted abduction tenderness to palpate over the lateral epicondyle

64
Popliteus tendonitis Develops with excessive downhill running, excessive squatting activities -X-cross country, squatting.

65
Inert Tissue Dysfunctions of the Knee
Ligament Medial Collateral Ligament a. MOI: valgus force applied to the lateral aspect of the knee with the foot fixed, knee in extension b. Less common MOI: knee in slight flexion (less than 90 dg), or twisting motion occurs
, or twisting motion occurs.")
66
Symptoms and Signs SX: Signs: mild tenderness at medial joint line
swelling Signs: Grade I, II, or III laxity with valgus stress, AROM is painful near the end of extension edema present point tender at adductor tubercle and/or medial joint line ALWAYS check it in the position that it was injured in, also before inflammation or after it goes down.

67
Stress Test Analysis Mild medial laxity with valgus stress,
Knee in full extension: damage to posterior oblique ligament and capsular ligament Gross instability at full extension: check ACL and PCL to make sure they are tight Empty end feel or indistinct end feel: secondary restraints are holding the knee, ligament is grade III

68
Medial Collateral Ligament
Ligaments turn up as BLACK Coronal Images used to evaluate MCL tears Proton density coronal image – arrows Show ligament as thin, well defined, low signal intensity from medial femoral condyle to the medial tibial metaphysis

69
Lateral Collateral Ligament
MOI: Varus force from the medial side of the knee. Isolated injuries are rare because of ligament's location posterior to the axis of the knee joint. Not as commonly injured, as very stable. Usually injured as a torsional overload that also affects the cruciate ligaments

70
Sx and Signs SX: lateral knee pain Signs:
varus laxity in extension and flexion numbness or tingling if nerve root is involved: common peroneal

71
Oblique orientation, low signal structure – white arrow
Inserts onto fibular head Avulsion fracture of the fibular head may be seen on plain film radiographs with a LCL injury

72
LCL and MCL tear LCL is outside the capsule,
A tear in the LCL does not Cause as much effusion as A MCL tear. You will not see An increased signal intensity Around the ligament as you do in an MCL tear. See figure to the right.

73
Anterior Cruciate Ligament:
MOI: combination of valgus and external rotation forces applied to the knee while foot is in a closed pack position Less common MOI: excessive internal rotation and hyperextension combination non contact injury in which sudden limb deceleration is accompanied by a contraction of the quads producing damaging force moments Commonly the MOI for woman.

74
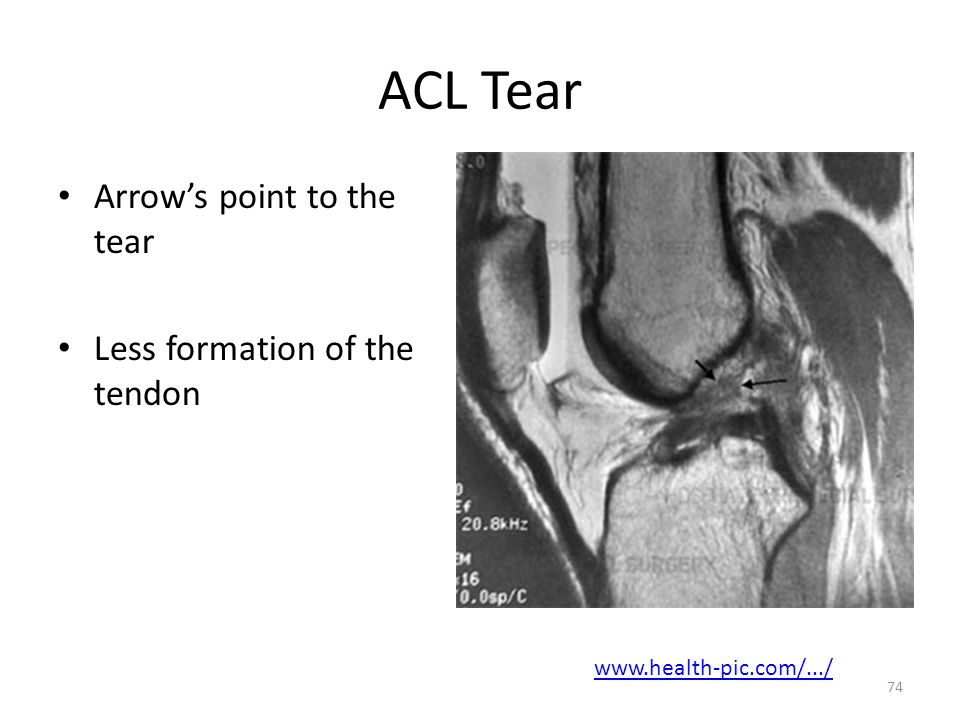
ACL Tear Arrow’s point to the tear Less formation of the tendon
75
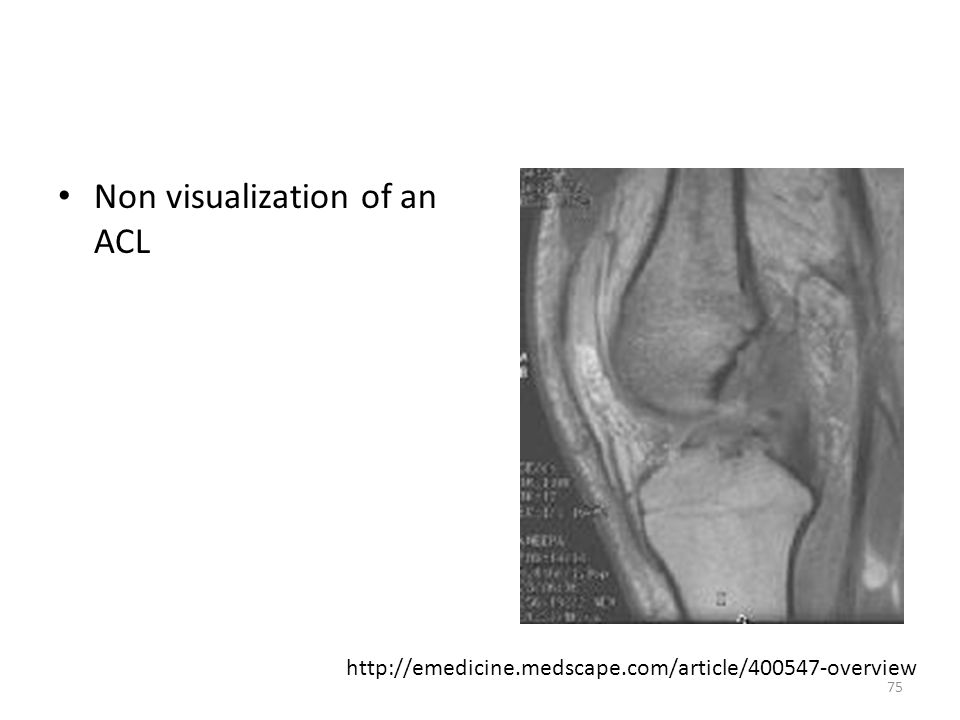
Non visualization of an ACL
76
Triad of images showing an ACL tear Top left: T2 Sagittal view
Top right: T2 coronal view Bottom: T1 coronal view,

77
Anterior Cruciate Ligament
Repair: sew the tear. Replacement: take out old, but in a new.

78
SX and Signs SX: Patient reports a "pop" at time of injury
Knee swelling within one hour after injury Hemarthrosis within 12 hours Signs: + Lachman's + pivot shift test + anterior drawer test Hamstring muscle spasm: can give a false negative as they protect any movement from anterior drawer. Inability to fully weight bear on affected side Weakness and knee giving way are frequent occurrences

79
Chronic problem Frequent episodes of knee giving out. Pain and effusion with specific activities that stress knee such as cutting and pivoting RX: depends on the degree of tear, Will generally wait 2-3 weeks until the swelling has decreased before going in and assessing the ligament MRI is diagnostic as is arthroscopic surgery Surgery: Type of graft used will depend upon the physician. Great controversy in the literature regarding the graft type.

80
Patella - Tendon Graft:
Central third of the patella tendon is taken to use as a graft, so quads will be affected. Considered to be 57% as strong as original ACL at 3 months and 87% as strong at 12 months. At first will decrease in strength, but eventually will remodel and become stronger. Some take the tendon from the opposite side, as will have balance out, but now will have issues on both side.

81
Two type of Patella Tendon grafts:
Injured leg. Have to deal with two injuries then, a decrease in the quad mechanism and the ACL repair Second is taken from the uninvolved leg. Gives a strong patella tendon on the ACL side but a weaker tendon on the opposite side (Shelbourne Procedure)
")
82
Semitendinosus and Gracilis Grafts
Provide weaker initial fixation and have a more prolonged and variable rate of fixation into the bone than does the central third patella grafts. Used when there is a significant incidence of patellofemoral and anterior knee pain associated with the injury Weakening the hamstring.

83
These tendons can be removed, doubled over, and then used to replace the ACL.
These tendons are easier to harvest than the patellar tendon, they require smaller drill holes in the femur and the tibia for fixation, and they do not predispose patients to patellar tendinitis.

84
Types of Grafts

85
ACL Patella Tendon Graft Surgery

86
Allografts: Cadaver grafts
Indications: Failed autograft surgery Significant patellofemoral arthrosis Narrow patella tendon Patients who don't want to use their own tissue 3 areas of concern: 1. Immune reaction 2. Potential disease transmission 3. Remodeling and effect on mechanical properties

87
Posterior Cruciate Ligament
MOI: anteromedial blow to the flexed knee or a fall onto the knee with foot and ankle plantarflexed Common component is the posteriorly directed force on the proximal tibia which pushes the tibial plateau posterior on the femoral condyles

88
PCL: All three images should be used, sagittal, coronal and axial
T1 Coronal Image Darker arrow is the PCL and is a lower intensity signal than the ACL Lighter arrow is the ACL

89
Sagittal View Proton dense sagittal image
Insertion site (arrows) is posterior to the tibia articulating surface
 is posterior to the tibia articulating surface.")
90
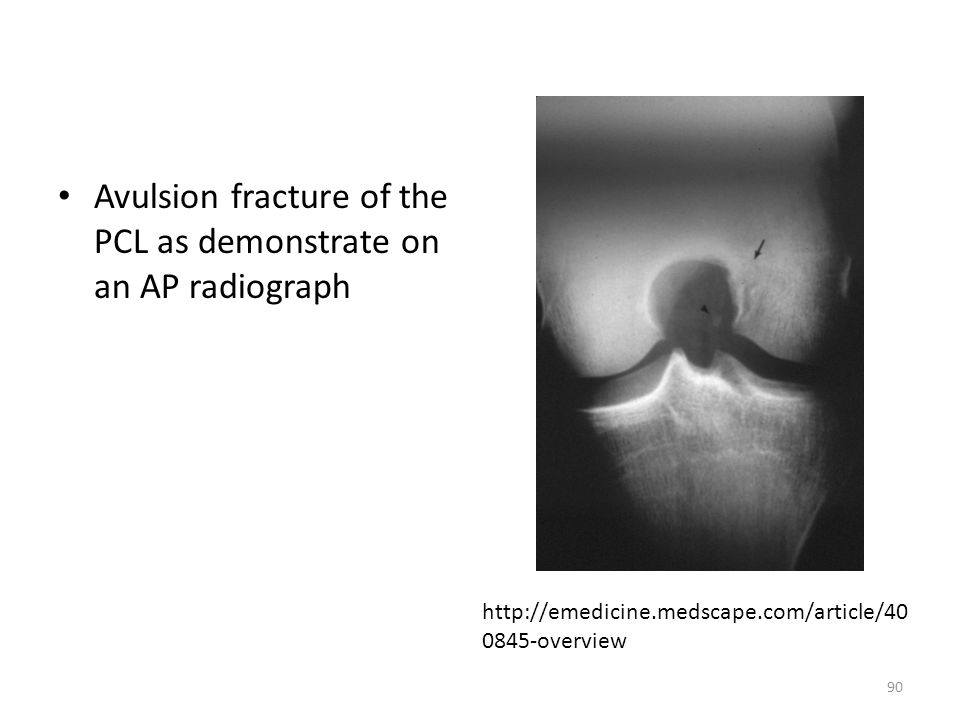
Avulsion fracture of the PCL as demonstrate on an AP radiograph
91
Interstitial tear of the PCL A: proton density sagittal image
B: T2-weighted sagittal image

92
Mid substance tear of the PCL- large arrow
Proton dense-weighted sagittal view Intact PCL proximally, tear, edema noted mid PCL Ligament of Humphrey – small arrow

93
SX and Signs: Signs: Sx: ROM is usually WNL Difficulty weight bearing
Painful on end range flexion Extensor lag present (tibia drops below the femur) + posterior drawer test + tibial sag test + hughston test Sx: Difficulty weight bearing Painful Instability with stairs and inclines Recurrent swelling
 + posterior drawer test. + tibial sag test. + hughston test. Sx: Difficulty weight bearing. Painful. Instability with stairs and inclines. Recurrent swelling.")
94
Surgery Surgery is controversial if only PCL is ruptured, Grade I PCL injuries with less than 5 mm of increased posterior translation of the tibia are managed non-operatively.

95
Surgical Reconstruction
Surgical reconstruction is recommended for isolated PCL disruption that result in 10 mm if increased posterior tibial translation. Also used with PCL injuries combined with injury to other ligamentous structures

96
Inert Structure Dysfunctions
Meniscus: Medial meniscus is more frequently injured than the lateral meniscus. (similar to SLAP lesions of the GH) Location of the tear will dictate the response to injury a. periphery: good repair, vascular, get a fibrocartilage scar tissue b. central portion, avascular, poor repair
 Location of the tear will dictate the response to injury a. periphery: good repair, vascular, get a fibrocartilage scar tissue b. central portion, avascular, poor repair")
97
Tears: MOI: traumatic, occurs in the 13 to 40 year olds,
occurs with activity that may or may not be contact related non-contact: acceleration or deceleration stresses combined with a sudden change in direction, squatting or twisting produces a longitudinal or transverse vertical tear

98
Types of Tears www.health.allrefer.com Stoller, D. Pocket Radiologist
Medial torn more often, then lateral Stoller, D. Pocket Radiologist

99
Types of Tears

100
Vertical Longitudinal Tears
Most frequent, Medial 2.5:1 greater incidence than lateral meniscus peripheral tear Greater than 1 cm in length Unstable with stress Causes symptoms Treat with surgery short, less than 5mm, full thickness to partial thickness stable, rarely cause symptoms, no surgery

101
Meniscal Tears: Longitudinal Tears
Axial illustration of a full-thickness longitudinal tear of the posterior horn. The meniscus is viewed from above in (a), sagittal in (b), and coronal in (c). A = anterior, L = lateral, M = medial, and P = posterior. Bowtie will be black in later veiw.
, sagittal in (b), and coronal in (c). A = anterior, L = lateral, M = medial, and P = posterior. Bowtie will be black in later veiw.")
102
Longitudinal Tear of the Meniscus
Coronal T2 image (with fat suppression) shows a displaced fragment (arrow) of medial meniscus into the intercondylar notch of the knee. Also known as a bucket handle tear share?id= %253APhoto%253A28117
 shows a displaced fragment (arrow) of medial meniscus into the intercondylar notch of the knee. Also known as a bucket handle tear. share id= %253APhoto%253A")
103
Vertical Transverse tears
Radial tears, less common, almost always the middle third of the lateral meniscus Stable less than 5 mm Surgery if it causes symptoms

104
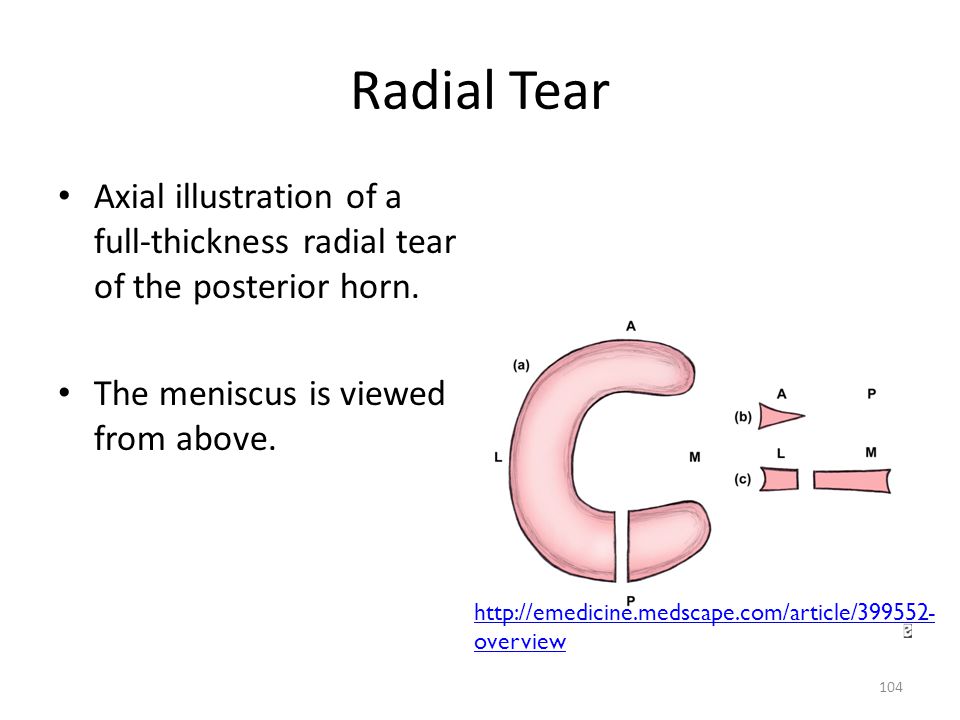
Radial Tear Axial illustration of a full-thickness radial tear of the posterior horn. The meniscus is viewed from above.
105
Degenerative tears Horizontal cleavage or flap tear.
Increase incidence in age over 40, No specific injury or minor degree of stress can cause the tear. Can occur in either meniscus, associated with degeneration of the articular cartilage After age 40, will often have a horizontal splitting as a result of bending, squatting, turning and twisting over the years. Horizontal lesion seen in people over age of 55, not always symptomatic. More common in the medial meniscus, usually occurs at the junction of the middle and posterior one-third

106
Horizontal Tear of Posterior Horn
Axial illustration of a full-thickness horizontal tear of the posterior horn. The meniscus is viewed from above. Not the same as the radial tear, goes through the substance of the meniscus in a horizontal, not vertical line

107
Posterior Horn Tear: Horizontal
Fat-suppressed proton density-weighted sagittal images reveal a horizontal tear of the posterior horn of the medial meniscus (arrows), extending to the tibial surface. See the Bowtie, with a white slip indicating a tear.
, extending to the tibial surface. See the Bowtie, with a white slip indicating a tear.")
108
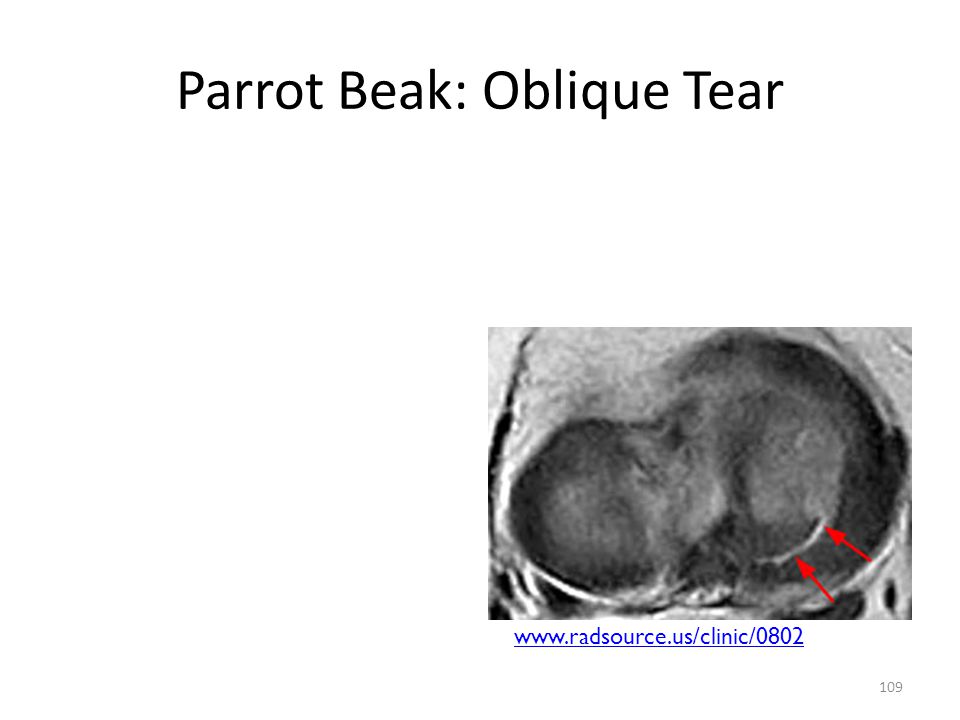
Flap tear Axial illustration of an oblique (parrot beak) tear of the posterior horn. The meniscus is viewed from above. In B, image 1 is most lateral, image 2 is middle, and image 3 is most medial. In C, image 1 is most anterior, image 2 is middle, and image 3 is most posterior.

109
Parrot Beak: Oblique Tear
110
SX and Signs Signs: Change in WB status
Minimal swelling may be noted with girth measurements McMurray's or Apley's test are positive Springy end feel SX: Pain at time of injury Persists and interferes with WB activity Recurrent episodes with minor stress Baker's cyst Knee is giving way

111
RX: surgery Link between an absent meniscus and OA.
Indications for surgery: Vertical tears Tears near the periphery of the meniscal substance Generally intact meniscal body Total tissue defect less than 2 cm

112
Synovial Plica Remnant of 3 embryonic pouches of synovial membrane which remain in the knee as excessive synovial material. Medial plica is the most symptomatic . Will tighten during knee flexion and cause a change in the normal mechanics of the patellofemoral joint.

113
Example: like a fine lace curtain
Probably causes no symptoms, Although the elastic edge may bow-string over the bone of the femur when the leg bends and straightens Should there be an injury affecting the plica, however, the edge can thicken and then cause regular symptoms of a 'catching' pain at particular joint positions.

114
Examples of Synovial Plica

115
SX and Signs: Sx: Similar to patellofemoral pain syndromes.
Pain in the medial aspect of the knee joint Clicking Intermittent locking sensation on medial side Generalized weakness Reports of joint instability Classic symptom is an inability to sit for prolonged periods of time Signs: must rule out meniscus and ligamentous injuries, bone injuries, radiographs, MRI, CT scans

116
RX Conservative treatment with NSAIDS Modalities Exercise
May use transverse friction massage

117
Bursitis Prepatellar Bursitis: injury through direct trauma or chronic irritation such as prolonged kneeling.

118
SX and Signs SX: Signs: Localized pain and swelling in the bursa
Tenderness to palpation Signs: Swelling of the bursa Warm to touch Redness Slight loss of knee flexion Strong but painful resisted knee extension

119
RX: Pain and edema control Anti-inflammatories Modalities in treatment
May inject corticosteroids or drain bursa

120
Bakers Cyst: Definition: any form of synovial herniation or bursitis involving the posterior aspect of the knee. Often occurs in conjunction with an intra-articular derangement at the knee such as a meniscal tear or ACL injury a. SX: mass behind the knee that may or may not be tender b. Signs: well defined, edematous mass on the posterior aspect of the knee c. When present, must rule out an internal derangement.

121
Images of Baker’s Cyst www3.americanradiology.com

122
Pes Anserine Bursitis Definition: follows a traumatic injury or unaccustomed WB exercise SX: Medial knee pain Aching at rest Swelling may be present on medial aspect of knee Signs: Tenderness to palpation Pain with resisted flexion

123
Common Imaging Anteroposterior View Lateral View
Sunrise View of the Patella Tunnel View of the Knee MRI Meniscus Imaging ACL Imaging PCL Imaging

124
RADIOGRAPHIC EXAMINATION OF THE KNEE AND PATELLA
Anteroposterior view: Important to do weight bearing if possible. Either way, you should note if the x-rays were taken in standing or while lying supine.

125
Alignment: Identify the following structures
distal femur medial and lateral condyles the proximal tibia fibula the patella superimposed over the distal femur

126
Look at joint space for the tibia and femur, well defined in both medial and lateral views

127
Normal knee: slight valgus alignment
Medial and lateral joint spaces should be equal Femoral condyles should be aligned with the tibial plateaus Increase in valgus or a varus mal-alignment will increase stress on medial or lateral compartment, resulting in sclerosing of the femoral condyle and tibial plateau

128
Anteroposterior view:
1 One of these is WB and one is N WB – how can you tell? Look at the medial joint line on right leg especially 2

129
AP: Bone Density Abnormal bone density: may see Osteochondral defects (OCD) on medial or lateral condyles of the femur Blue arrow points to a radioluscent cresent area on the knee: osteochondral dissecans

130
Cartilage Clear, wide joint space
Abnormal for there to be diminished space Generally, one condyle is involved first, then both in advanced stages of OA Bone on bone – absence of meniscus

131
Lateral View: Views the patellofemoral joint in profile, knee is flexed anywhere's from 20 dg to 45 dg and the beam is directed from a medial to lateral direction.

132
Look for the relationship of the patella to the femur, can determine patella alta or patella baja

133
Insall-Salvati Index: PLR = PL/TL
The length of the patella ligament is measured from its attachment at the patellar apex to the tibial tuberosity (TL) and should equal the length of the patella (PL) from the superior to the inferior poles. Variance greater than 20% indicates an abnormal patella position.
 and should equal the length of the patella (PL) from the superior to the inferior poles. Variance greater than 20% indicates an abnormal patella position.")
134
Lateral: Bone Density Increase in density as the condyles are superimposed on each other Medial condyle is larger and extends distally further than the lateral condyle Patella should be consistent in density

135
Sunrise View or Skyline View
Patella appears to be the sun, rising over the horizon Axial view of the Patellofemoral joint: Gives the articular surfaces of the patella and femur. Medial and lateral facets of the patella are visible Alignment of the patella in relation to the femur – lateral, medial etc.

136
Note the sulcus angle of the femur:
normal value of 138 degrees +/- 6 degrees shallow sulcus angles (greater degree within the angle) have been associated with recurrent patellar dislocations.
 have been associated with recurrent patellar dislocations.")
137
Note the congruence angle which helps to define the position of the patella within the inercondylar sulcus. Normal value is -6 degrees. Congruence value of +16 has been associated with lateral patellar subluxation

138
To measure the congruence angle: Find the highest point of the medial (B)and lateral (C) condyle and the lowest point of the intercondylar sulcus (A) The angle BAC, is the sulcus angle. Bisect the sulcus angle to establish the zero reference line, AO. Find the lowest point on the articular edge of the patella (D) Project line AD. The angle DAO is the congruence angle. All values medial to the zero reference line AO are designated as minus and those lateral as plus. Mean= -6 Degrees, standard deviation = 11 degrees.
 Project line AD. The angle DAO is the congruence angle. All values medial to the zero reference line AO are designated as minus and those lateral as plus. Mean= -6 Degrees, standard deviation = 11 degrees.")
139
Other Common Views: Axial or Tunnel view of Intracondylar fossa: Taken in a prone position, will view the intercondylar fossa, and the posterior aspects of the knee joint. x-ray beam is projected in a posterior to anterior direction 1,2 are intercondylar eminences 3,4 are tibial plateaus

140
MRI Knee joint MRI is one of the most frequently requested imaging study in musculoskeletal radiology Comprehensive, non-invasive view of the meniscus, ACL, PCL, medial and lateral collateral ligaments Sensitivity and Specificity of 90-95% for the meniscus and almost 100% for the cruciate ligaments. (Helms, 2009)
")
141
Images Sagittal Sequences give the most information on the knee
Short TE will help with imaging the meniscus Fast Spin Echo – proton density (FSE-PD) do not produce acceptable images of the knee Fat suppression Makes the MRI image easier to view Allows the Meniscal tears to stand out easier than without the suppression.
 do not produce acceptable images of the knee. Fat suppression. Makes the MRI image easier to view. Allows the Meniscal tears to stand out easier than without the suppression.")
142
MRI Ligaments and Meniscus: image black whether it’s a T1 or T2 image.
This MRI shows the meniscus as to triangular black blocks just under the femur. The patella ligament (tendon) images black from patella to tibial tubercle.
 images black from patella to tibial tubercle. id=152.")
143
Meniscus A fat-suppressed proton density-weighted axial image through the knee Demonstrates the C-shaped menisci. Note the symmetrical shape of the lateral meniscus (red outline) and the asymmetry of the medial meniscus (blue outline), where the posterior horn (asterisk) is significantly larger than the anterior horn.
 and the asymmetry of the medial meniscus (blue outline), where the posterior horn (asterisk) is significantly larger than the anterior horn.")
144
Sagittal fat-saturated proton density–weighted image:
Concave superior meniscal surface (arrows), which improves contact with the femoral epicondyles, and a flat undersurface, which improves contact with the tibial plateau. The periphery (outer edges) is thicker than the central portion (arrowhead), allowing for firm attachment to the joint capsule. Normal bow-tie appearance of the meniscal body.
, which improves contact with the femoral epicondyles, and a flat undersurface, which improves contact with the tibial plateau. The periphery (outer edges) is thicker than the central portion (arrowhead), allowing for firm attachment to the joint capsule. Normal bow-tie appearance of the meniscal body.")
145
Coronal fat-saturated proton density–weighted image: Posterior slice
Posterior horns of the medial and lateral menisci. The posterior horn of the medial meniscus (left arrow) is thicker than the posterior horn of the lateral meniscus (right arrow). The medial portion of the posterior horn of the lateral meniscus (ie, the meniscus on top of the fibula) is directed upward obliquely, from a lateral to medial direction. This is its normal course.
 is thicker than the posterior horn of the lateral meniscus (right arrow). The medial portion of the posterior horn of the lateral meniscus (ie, the meniscus on top of the fibula) is directed upward obliquely, from a lateral to medial direction. This is its normal course.")
146
Transverse (Intermeniscal) Ligament
Axial fat-saturated proton density–weighted image Transverse (intermeniscal) ligament (arrows) connecting the anterior portions of the medial and lateral menisci
 ligament (arrows) connecting the anterior portions of the medial and lateral menisci.")
147
The ligament of Wrisberg
Coronal proton density–weighted image originating from the posterior medial horn of the medial meniscus and passing obliquely upwards (arrow) to attach to the posterolateral aspect of the medial femoral epicondyle
 to attach to the posterolateral aspect of the medial femoral epicondyle.")
148
Coronal fat-saturated proton density–weighted image of the mid knee
Normal appearance of the body of the medial and lateral menisci. The apices (inner portions) are the thinnest part of the meniscus and are more central in the knee joint. The periphery, meniscal bases, outer portion (arrow and arrowhead) is the thickest part and contains the blood vessels supplying the meniscus.
 are the thinnest part of the meniscus and are more central in the knee joint. The periphery, meniscal bases, outer portion (arrow and arrowhead) is the thickest part and contains the blood vessels supplying the meniscus.")
149
ACL and PCL: Normal Again, the ligaments will Image darker on the MRI.
Note the orientation of fibers When determining the Structure These two images are taken At different depths in order To see the ligaments this clearly

150
ACL: Normal Views

Similar presentations