Download presentation
Presentation is loading. Please wait.

1
Dental Trauma Northern ED Registrar Teaching Program Dr Louisa Lee
(Acknowledgement – Dr Tony Skapetis) (References include EM Practice 2003)
 (References include EM Practice 2003)")
2
Not all patients need to go to the
Objectives Be able to describe and classify dental injuries Know how to manage simple avulsion and luxation injuries in the ED Be familiar with the ED Dental Trauma Kit Not all patients need to go to the Royal Dental Hospital!

3
Basic Tooth Anatomy Pulp contains neurovascular supply of tooth that carries nutrients to dentin Enamel has no neurovascular supply connected to pulp – therefore, isolated enamel # shouldn’t elicit pulpal pain (cf dentin – very temperature sensitive) Dentin – makes up most of tooth - Microporous substance consisting of system of microtubules Enamel is white, dentin is creamy yellow Attachment apparatus consists of 2 major subunits & is necessary for maintaining integrity of normal dentoalveolar unit: Gingival subunit = junctional epithelium + gingival tissue Periodontal subunit = periodontal lig, alveolar bone + cementum of root of tooth (periodontal memb = periodontal lig) Periodonal lig holds tooth in place + acts as barrier to surrounding osteoclasts - Any damage osteoclastic activation, eats root away over 1-2/12
 Dentin – makes up most of tooth. - Microporous substance consisting of system of microtubules. Enamel is white, dentin is creamy yellow. Attachment apparatus consists of 2 major subunits & is necessary for maintaining integrity of normal dentoalveolar unit: Gingival subunit = junctional epithelium + gingival tissue. Periodontal subunit = periodontal lig, alveolar bone + cementum of root of tooth (periodontal memb = periodontal lig) Periodonal lig holds tooth in place + acts as barrier to surrounding osteoclasts. - Any damage osteoclastic activation, eats root away over 1-2/12.")
4
How do you describe teeth?

5
Dental Nomenclature FDI Classification (used Australia & worldwide)
If tooth missing, will skip a number

6
Primary (Deciduous) Teeth
Can be hard to distinguish primary from permanent teeth Hints: Permanent tooth usually looks more yellow Age < 6yo – likely all 1° teeth > 12 yo – likely all permanent

8
Mouth of patient who sustained multiple punches to face in a fight.
Avulsed teeth 22, 44, 45 + decoronated 14, 15 + unCx’d crown # (through enamel & dentin) 16, 27, 44, 45, 46, 36
 16, 27, 44, 45, 46, 36.")
9
Descriptive Terminology
Facial – part of tooth seen when a person smiles Labial – facial surface of incisors & canines Buccal – facial surface of molars & premolars Oral – part of tooth that faces the tongue/palate Lingual – toward the tongue, oral surface of mandibular teeth Palatal – toward the palate, oral surface of maxillary teeth Approximal/interproximal – contacting surfaces between 2 adjacent teeth Mesial – interproximal surface facing anteriorly/closest to midline Distal – interproximal surface facing posterior/away from midline Occlusal – biting/chewing surface of molars & premolars Incisal – biting/chewing surface of incisors & canines

10
Lingual (oral) aspects of L lower teeth showing carious cavitated lesions 31, 32, 33
 aspects of L lower teeth showing carious cavitated lesions 31, 32, 33")
11
How do you assess patients presenting with dental trauma?

12
Assessment in Dental Trauma
Airway compromise Associated injuries Facial & mandibular fractures Tongue blade test Soft tissue injuries e.g mucosal, tongue lacerations Brain & C spine injuries Full inspection of oral cavity Percuss with tongue depressor for sensitivity Palpate with fingers/tongue depressor for mobility Missing teeth or pieces of teeth – where are they? Aspirated? Check bite Facial/mandibular #s – may leave tongue unsupported or midface unstable Bleeding from soft tissue injuries may be severe enough to cause airway compromise (esp if spinal precautions) Intubated RMH trauma patient w/ facial injury who was hypoxic – portable CXR found tooth lodged in RMB Bite – teeth should meet symmetrically & evenly when biting Can be difficult to know what is patient’s premorbid dentition & what is acute – use driver’s licence/photo ID/photos from Smartphone to compare
 Intubated RMH trauma patient w/ facial injury who was hypoxic – portable CXR found tooth lodged in RMB. Bite – teeth should meet symmetrically & evenly when biting. Can be difficult to know what is patient’s premorbid dentition & what is acute – use driver’s licence/photo ID/photos from Smartphone to compare.")
13
Some General Principles in Managing Dental Trauma
Identify (account for) all fracture fragments and mobile teeth OPG, CXR may be necessary Note if any mandibular fracture open or closed Give adequate analgesia/anaesthesia Don’t forget tetanus status Pathology only if clinically indicated e.g. coagulopathy, liver failure
 all fracture fragments and mobile teeth. OPG, CXR may be necessary. Note if any mandibular fracture open or closed. Give adequate analgesia/anaesthesia. Don’t forget tetanus status. Pathology only if clinically indicated. e.g. coagulopathy, liver failure.")
14
WHO Classification of Traumatic Injuries
Injuries to hard dental tissues of mouth Dental fractures Injuries to periodontal tissues or supporting tissues of teeth Luxations & Avulsions

15
Ellis Classification of Dental Fractures
X Although often cited in emergency literature, many dentists & OMFS surgeons don’t use this classification

16
Injuries to the hard dental tissues of the mouth
Crown infraction Incomplete # of the enamel without loss of tooth structure Uncomplicated crown # Crown # without pulp exposed Complicated crown # Crown # with pulp exposed Uncomplicated crown-root # Crown # extending below gum line & involving root, but not exposing the pulp Complicated crown-root # Crown # extending below gum line & involving root, but also exposing the pulp i.e. # is complicated if pulp is exposed Forget Ellis classification – WHO classification simpler & more practical UnCx’d crown # can be through enamel +/- dentin How do you know if pulp is exposed? Will see a pink dot in the # or have bleeding from the tooth May have severe pain (but may have no pain if neurovasc supply of tooth disrupted)
")
17
Complicated crown # of tooth 21

18
Dental Fractures It’s all about the pulp!
Goal of ED treatment = maintain pulp viability (avoid pulp necrosis) & avoid pulp contamination ED Rx aimed at sealing dentinal tubules ASAP to prevent pulp contamination/infection (↑ risk with ↑ delay to Rx) - may prevent need for endodontic (root canal) treatment Pulpal necrosis can occur any time after trauma, ∴ serial F/U w/ dentist recommended Delayed # care & poor gingival health ↑ risk of pulp necrosis
 & avoid pulp contamination. ED Rx aimed at sealing dentinal tubules ASAP to prevent pulp contamination/infection. (↑ risk with ↑ delay to Rx) - may prevent need for endodontic (root canal) treatment. Pulpal necrosis can occur any time after trauma, ∴ serial F/U w/ dentist recommended. Delayed # care & poor gingival health ↑ risk of pulp necrosis.")
19
Uncomplicated Crown Fractures
Through enamel only: Not an emergency Pulp necrosis unlikely (0-3%) File down sharp edges with nail file Non urgent dental follow up
 File down sharp edges with nail file. Non urgent dental follow up.")
20
Uncomplicated Crown Fractures
Dentin Exposed: Risk of pulp necrosis 1-7% Analgesia Tooth block Cover exposed dentin with CaOH or GIC Soft diet Prophylactic antibiotics Dental review within hours Cover exposed dentin to prevent pulpal contamination infection Dentist can still rebuild tooth afterwards w/ modern composites Surface of tooth must be dry before application to ensure adherence (have pat bite into gauze pads while prepping) CaOH will dry within minutes No need to cover if pat sees dentist within 24-48/24 Soft diet to prevent dislodgement of dressing Pencillin/amoxycillin/clindamycin
 CaOH will dry within minutes. No need to cover if pat sees dentist within 24-48/24. Soft diet to prevent dislodgement of dressing. Pencillin/amoxycillin/clindamycin.")
21
Complicated Crown Fractures
True dental emergency Pulp necrosis 10-30% Analgesia Avoid OTC topical analgesics Control haemorrhage Cover exposed pulp & dentin Liquid diet Antibiotics Urgent dental review (<24 hours) Which teeth are affected? Teeth 11, 21 & 22 High Ro pulp necrosis even w/ appropriate Rx – true dental emergency Topical analgesics - - > sterile abscess & soft tissue irritation May need to control haemorrhage by pat biting on cophenylcaine-soaked gauze Cover exposed pulp w/ CaOH cover this + remaining dentin w/ GIC Dental review within 24 hours Most pats will need root canal Rx (e.g. pulpectomy)
 Which teeth are affected Teeth 11, 21 & 22. High Ro pulp necrosis even w/ appropriate Rx – true dental emergency. Topical analgesics - - > sterile abscess & soft tissue irritation. May need to control haemorrhage by pat biting on cophenylcaine-soaked gauze. Cover exposed pulp w/ CaOH cover this + remaining dentin w/ GIC. Dental review within 24 hours. Most pats will need root canal Rx (e.g. pulpectomy)")
22
Subluxations & Avulsions
(Wobbly & Dislodged Teeth)
")
23
Injuries to periodontal tissues or supporting tissues of teeth
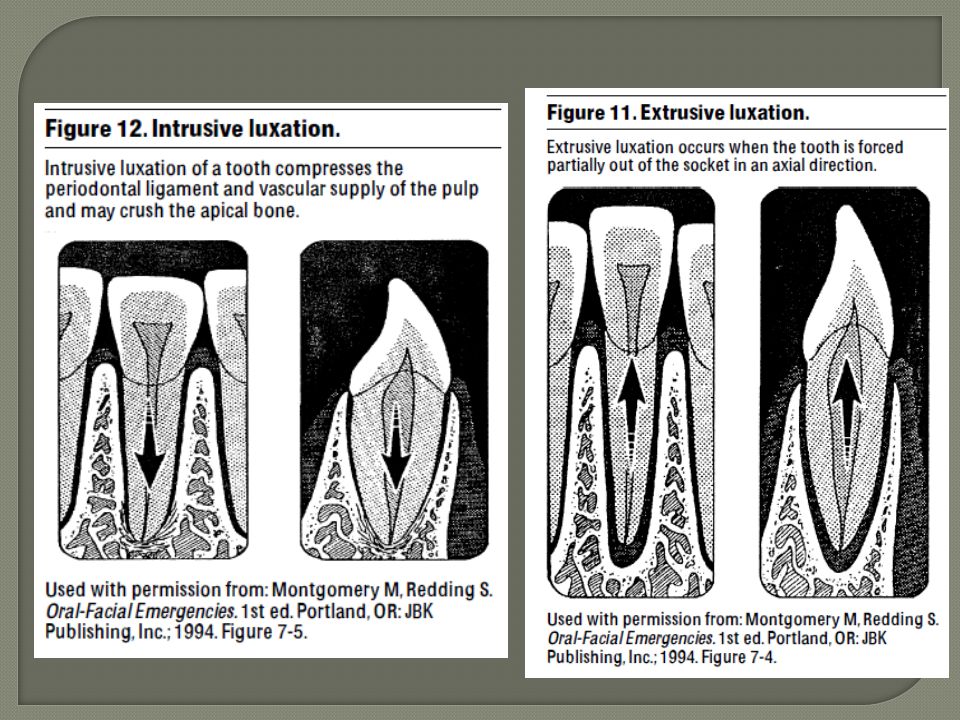
Concussion – injury to supporting structures without abnormal loosening/displacement Subluxation – tooth loosening without displacement Intrusive luxation – tooth is pushed into socket, towards gum Extrusive luxation – tooth is pushed away from socket but not yet avulsed Avulsion – complete dislodgement from socket Concussion – clinical tenderness to percussion but no mobility (∴ splinting not indicated) - Rx – NSAIDs, soft diet, dental r/v Intrusive luxation – most serious type of luxation + poorest outcomes (highest Ro pulp necrosis & root resorption) - sig. damage to alveolar socket (often w/ ass. alveolar #) + periodontal lig - don’t bother Rx’ing if >24/24 delay in Px Other injuries not listed - isolated root #, lateral luxation
 - Rx – NSAIDs, soft diet, dental r/v. Intrusive luxation – most serious type of luxation + poorest outcomes (highest Ro pulp necrosis & root resorption) - sig. damage to alveolar socket (often w/ ass. alveolar #) + periodontal lig. - don’t bother Rx’ing if >24/24 delay in Px. Other injuries not listed - isolated root #, lateral luxation.")
26
Extrusive luxation of teeth 11 & 12 (also some lateral luxation mesially)
")
27
Extrusion of tooth 11 with uncomplicated crown #

28
Management of Luxations
Local anaesthetic Finger reduction & splinting Do NOT manipulate primary teeth Soft diet Dental review hours Manipulation may create more periodontal membrane damage (+ risk of injury to underlying permanent tooth) If leave primary tooth alone, permanent tooth likely to re-erupt into N position
 If leave primary tooth alone, permanent tooth likely to re-erupt into N position.")
29
Dental Avulsions Involving Primary Teeth
Never reimplant a primary tooth For near avulsions, if the tooth is interfering with bite or risk of being swallowed/aspirated, extract it Primary teeth are not replaced because they can fuse to the alveolar bone and potentially cause craniofacial abnormalities or infection, and they may prevent normal eruption of the permanent teeth. (EM Practice)
")
30
Dental Avulsions Involving Permanent Teeth
Time is tooth! You lose 1% chance of successful replant for every minute out of socket Within 30 minutes ideal, OK to try up to 3/24 Storage medium is 2nd most important factor Milk (not flavoured or soy) or saline best Never let the tooth dry out No replanting if alveolar ridge fracture present Key to successful reimplantation = survival of periodontal lig ff that remain attached to root of avulsed tooth Periodontal cells die within 60/60 if not placed in appropriate storage medium or left to dry out ~77% of periodontal memb cells still alive after 3/24 in milk (milk found to preserve periodontal lig for at least 8-12 hours) Time to storage media is very important – 5-10 mins outside storage media can cause dessication & death of periodontal memb cells Saline only good for 2 hours as contains no nutrients Saliva preferable to water, but not desirable to store in mouth (may swallow & aspirate, saliva has low osmolality + bacterial flora)
 or saline best. Never let the tooth dry out. No replanting if alveolar ridge fracture present. Key to successful reimplantation = survival of periodontal lig ff that remain attached to root of avulsed tooth. Periodontal cells die within 60/60 if not placed in appropriate storage medium or left to dry out. ~77% of periodontal memb cells still alive after 3/24 in milk (milk found to preserve periodontal lig for at least 8-12 hours) Time to storage media is very important – 5-10 mins outside storage media can cause dessication & death of periodontal memb cells. Saline only good for 2 hours as contains no nutrients. Saliva preferable to water, but not desirable to store in mouth (may swallow & aspirate, saliva has low osmolality + bacterial flora)")
31
Management of Dental Avulsions
Local anaesthetic Handle tooth from crown Do NOT touch root surface Irrigate socket with saline & check for bone fragments from socket wall Rinse tooth using tap water or saline Insert into socket ASAP Check occlusion Splint with GIC ADT if appropriate Soft diet Antibiotics Doxycycline 100mg BD for 7/7 (Penicillin V if < 12 yo) Chlorhexidine (0.1%) mouthwash BD for 7/7 Non urgent Dental review (<2 weeks) Never handle root if possible as will damage periodontal lig cells (also don’t wipe root as will remove periodontal lig – rinse off any debris w/ saline) Preparation of dental socket plays little role in success/failure of reimplantation When retrieving tooth, drain milk/storage medium off 1st (to avoid accidental handling of root) Early improper reimplantation holds higher success rate cf delayed reimplantation You can’t make the situation worse! Chlorhex to reduce bacterial load in mouth Doxy inhibits osteoclastic activity
 Chlorhexidine (0.1%) mouthwash BD for 7/7. Non urgent Dental review (<2 weeks) Never handle root if possible as will damage periodontal lig cells (also don’t wipe root as will remove periodontal lig – rinse off any debris w/ saline) Preparation of dental socket plays little role in success/failure of reimplantation. When retrieving tooth, drain milk/storage medium off 1st (to avoid accidental handling of root) Early improper reimplantation holds higher success rate cf delayed reimplantation. You can’t make the situation worse! Chlorhex to reduce bacterial load in mouth. Doxy inhibits osteoclastic activity.")
34
Dental Blocks Tooth block (Supraperiosteal infiltration)
Front teeth 25G needle Rule of 2s – 2mm penetration, 2ml volume of 2% lignocaine Infraorbital nerve block Upper front teeth (up to tooth 5) Also good for suturing facial & lip lacerations 23G needle Intra-oral approach or direct infiltration Inferior alveolar nerve block Mandibular back teeth Alternative to 2% lignocaine = 0.5% bupivacaine/ropivacaine Insert needle into greatest concavity of mucobuccal fold (sulcus) related to tooth & inject parallel to long axis of tooth (direct needle towards apex of tooth)
 Also good for suturing facial & lip lacerations. 23G needle. Intra-oral approach or direct infiltration. Inferior alveolar nerve block. Mandibular back teeth. Alternative to 2% lignocaine = 0.5% bupivacaine/ropivacaine. Insert needle into greatest concavity of mucobuccal fold (sulcus) related to tooth & inject parallel to long axis of tooth (direct needle towards apex of tooth)")
35
Using GIC 1 level teaspoon of powder to 1 drop of liquid
Mix with a tongue depressor Do NOT mix with metal (will stain GIC) Setting time 2-3 minutes use GIC on pad as guide Maintain tooth position with finger pressure until GIC sets GIC = glass ionomer cement Base + catalyst Splints best when applied on both facial & oral surfaces Teeth need to be dry for application to stick Apply dressing into grooves between teeth as well as adjacent teeth
 Setting time 2-3 minutes. use GIC on pad as guide. Maintain tooth position with finger pressure until GIC sets. GIC = glass ionomer cement. Base + catalyst. Splints best when applied on both facial & oral surfaces. Teeth need to be dry for application to stick. Apply dressing into grooves between teeth as well as adjacent teeth.")
36
The End!! Any questions or comments?

Similar presentations




















>")
. All rights reserved. No part of this product may be reproduced or transmitted.>")

