Download presentation
Presentation is loading. Please wait.

1
Basic Human Needs Sleep

2
Sleep Proper rest & sleep are as important to good health as good nutrition and adequate exercise Amount of sleep required varies among individuals Physical & emotional health on the ability to fulfill these basic human needs

3
Sleep Without proper amounts of rest & sleep, the ability to concentrate, make judgments, & participate in daily activities decreases & irritability increases

4
Functions of Sleep Theories
Associated with healing & restoration Quality of sleep important to health promotion

5
Physiology of Sleep Sleep-cyclical physiological process that alternates with longer periods of wakefulness Sleep-wake cycle influences & regulates physiological function & behavioral responses

6
Circadian Rhythms Cyclical rhythms are part of everyday life
Most familiar rhythms is the 24 hr day-night cycle known as diurnal or circadian rhythm Menstrual cycle-infradian rhythm

7
Circadian Rhythm Influence the pattern of major biological and behavioral functions Body temperature, heart rate, blood pressure, hormone secretion, sensory acuity & mood depend on the maintenance of the 24 hr cycle

8
Circadian Rhythms Affected by: light, temperature, external factors (work schedules, social activities) Biological clock- synchronize sleep cycle, individualized to person, different people function best at different times of the day

9
Sleep Regulation Sleep involves a sequence of physiological states (stages of sleep) maintained by highly integrated central nervous system activity that is associated with all body systems (C-V, endocrine, nervous, respiratory)
 maintained by highly integrated central nervous system activity that is associated with all body systems. (C-V, endocrine, nervous, respiratory)")
10
Sleep Regulation Each sequence can be identified by specific physiological responses and brain activity patterns Current theory indicates sleep is thought to be an active mutliphase process Major sleep center-hypothalamus Control & regulation of sleep may depend on the interrelationship between 2 cerebral mechanisms that intermittently activate & suppress the brain’s higher centers to control sleep & wakefulness

11
Reticular Activating System
Located in upper brain stem Believed to contain special cells that maintain alertness & wakefulness RAS receives visual, auditory, pain, and tactile sensory stimuli Activity from the cerebral cortex(thoughts, emotions) also stimulate RAS
 also stimulate RAS.")
12
Reticular Activating System
Wakefulness results from neurons in the RAS that release catecholamines such as norepinephrine

14
Bulbar Synchroninizing Region (BSR)
Sleep may be produced by the release of seretonin from specialized cells in the Raphe sleep system of the pons & medulla also known as the BSR Whether a person remains awake or falls asleep depends on a balance of impulses received from higher centers (thoughts), peripheral sensory receptors (sound, light) and the Limbic system (emotions)
, peripheral sensory receptors (sound, light) and the Limbic system (emotions)")
15
Falling Asleep As people try and fall asleep, they close their eyes and assume a relaxed position, stimuli to RAS decline. If the room is quiet & dark, activation to RAS declines further At some point BSR takes over, causing sleep

16
Stages of Sleep Measured by EMG, EEG, EOG
Normal sleep involves 2 phases: NREM (Nonrapid eye movement) REM (Rapid eye movement)
 REM (Rapid eye movement)")
18
NREM Sleep NREM-sleeper progresses through 4 stages during a typical 90 min sleep cycle Progresses from stage 1-4 Sleep becomes increasingly deep Lighter sleep- stages 1-2 Deeper sleep- stages 3-4 REM sleep is the phase at the end of each 90 minute cycle

20
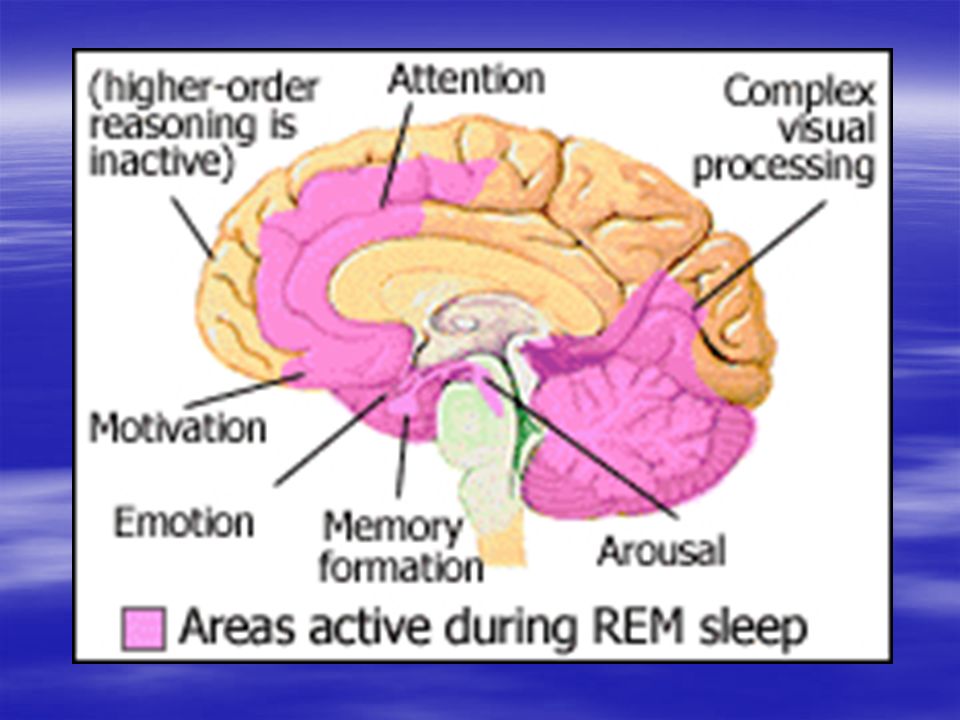
REM Sleep Vivid, full color dreaming
Typified by autonomic response by rapidly, moving eyes, fluctuating heart & respiratory rates and increased or fluctuating BP Very difficult to arouse sleeper Duration of REM sleep increases with each cycle, averages about 20 min

22
Sleep Once person falls asleep, person usually passes through 4-6 complete sleep cycles per night Each cycle consisting of 4 stages of NREM sleep and a period of REM sleep Pattern- NREM stages 1-4 followed by a reversal of stages, 4,3,2, ending with a period of REM sleep Reach REM sleep 90 minutes into sleep cycle

23
Functions of Sleep Allows body to rest, slows vitals, preserves cardiac function, decrease in muscle tone Sleep restores biological processes Body conserves energy during sleep (Lowers metabolic rate) REM sleep important for cognitive restoration, memory storage, & learning, during sleep brain filters information about the day’s activities
 REM sleep important for cognitive restoration, memory storage, & learning, during sleep brain filters information about the day’s activities.")
25
Functions of Sleep Loss of REM sleep can lead to feelings of confusion & suspicion Prolonged sleep loss affects mood, motor performance, memory & equilibrium Sleep deprivation-results in traffic accidents, home, work related accidents

26
Dreams Dreams occur in NREM & REM More vivid & elaborate in REM
Important to the consolidation of long-term memory

27
Physical Illness Affect on Sleep
Any illness resulting in pain, physical discomfort(SOB) or mood problems (anxiety, depression) can result in sleep problems Respiratory disease often interferes with sleep (COPD & orthopnea) Nocturia disrupts sleep cycle Restless leg syndrome
 or mood problems (anxiety, depression) can result in sleep problems. Respiratory disease often interferes with sleep (COPD & orthopnea) Nocturia disrupts sleep cycle. Restless leg syndrome.")
28
Sleep Disorders Insomnia Parasomnias
Sleep Disorders Associated with Medical or Psychiatric Disorder Hypersomnias Circadian Rhythm Sleep Disorders Sleep-Related Movement Disorders Refer to P &P pg Box 42-3

29
Parasomnias Undesirable behaviors that occur predominately during sleep More common in children Arousal disorders Sleep-wake transition disorder Parasomnia associated with REM sleep Other Parasomnias

30
Insomnia Symptom experienced by clients who have a chronic difficulty falling asleep, frequent awakenings from sleep and/or a short sleep or non-restorative sleep C/O excessive daytime sleepiness

31
Insomnia May be transient due to emotional stress, family, work, or school problem, or loss of a loved one May be associated with poor sleep hygiene, habits and practices associated with sleep

32
Sleep Apnea Lack of airflow through nose & mouth for periods of 10 seconds or longer during sleep 3 Types- Central, Obstructive, Mixed Most common type-Obstructive Sleep Apnea (OSA)
")
33
Obstructive Sleep Apnea
Relaxation of muscles & structures of oral cavity during sleep Upper airway becomes obstructed Person still attempts to breathe resulting in loud snorting & snoring sounds Deviated septum, nasal polyps, enlarged tonsils can predispose you to OSA Results in severe interference with deep sleep and EDS

36
Obstructive Sleep Apnea
18 million in U.S. Causes a serious decline in oxygen level Risk for cardiac dysrythmias, heart failure, pulmonary hypertension, stroke, HTN Most common im men, the obese, and postmenopausal women

37
Sleep Apnea Treatment Weight loss Sleeping on side CPAP Bi-PAP

40
Central Sleep Apnea Involves dysfunction in the brains respiratory control center Impulse to breathe temporarily fails Nasal airflow & chest wall movement cease, O2 sat falls Seen in brain stem injury, muscular dystrophy, encephalitis Bipap mask

41
Narcolepsy Dysfunction of the mechanisms that regulate sleep & wake states Excessive daytime sleepiness Fall asleep uncontrollably during day at inappropriate times REM sleep within 15 minutes May be genetic

42
Sleep Deprivation Occurs as a result of dyssomnias
Causes include: illness, emotional stress, medications, environmental disturbances, shift work Nurses at risk, patients at risk

43
Symptoms of Sleep Deprivation
Blurred vision Clumsiness Slow response Decreased reasoning Decreased visual alertness Arrhythmias Confusion Disorientation Irritability Sleepiness Agitation Decreased motivation

44
Normal Sleep Requirements
Neonates Infants Toddlers Preschool School age Teens Young adults Middle Adults Older Adults

45
Factors Affecting Sleep
Drugs & Substances Lifestyle Usual sleep patterns & excessive daytime sleepiness Emotional stress Environment Exercise & fatigue Diet

46
Nursing Process Assessment
Sleep assessment Description of sleep problems Usual sleep pattern Current life events Emotional & mental status Bedtime routines & environment Behaviors of sleep deprivation: “ICU Syndrome”

47
Nursing Diagnosis Anxiety Ineffective Breathing Pattern
Sleep Pattern Disturbance Alteration in Sensory Perception Ineffective Coping Acute Confusion Fatigue

48
Implementation Environmental controls Promoting bedtime routines
Promoting Comfort Establishing periods of rest & sleep Stress Reduction Bedtime snacks Pharmacological agents

49
Pharmacological Agents
Hypnotics-induce sleep Sedatives- produce a calming effect Long term use can disrupt sleep Benzodiazepines- Xanax, Valium, Ativan, Dalmane, Restoril, Halcion, Versed, Librium, Serax Non-Benzo Hypnotics: Ambien, Lunesta, Rozerem Barbiturates: Seconal, Nembutal OTC Sleep aids

Similar presentations
















>")



, Assoc MAPS>")
 Necessary for Physical and Mental Health $50 Billion / Year in Lost Productivity Occupies 1/3 of our Lives.>")






