Download presentation
Presentation is loading. Please wait.

1
NPLEX Combination Review Emergency Medicine
Paul S. Anderson, ND Medical Board Review Services Copyright MBRS

2
Emergency Childbirth i.e. you would be surprised how common an emergent birth situation occurs on a board exam!

3
Signs that birth is imminent:
Contractions 2-3 minutes apart or less How is the interval timed? Mother feels urge to push with each contraction Crowning

4
Preparation Get mother comfortable (prop with pillows)
Drape abdomen, each leg, as well as under her Wash hands! Get ready for the “catch”

5
Delivery: Head

6
Delivery: Shoulders If possible, clear airway
Head and shoulders rotate naturally

7
Delivery: Chest and Rest of Body

8
Delivery: Catch!

9
Lay baby NEXT to Mother and:
Clear Airway Towel dry and wrap in dry blanket If not breathing (crying) yet, clear airway again, and flick soles of feet If still not breathing, give 2 breaths, check pulse and CPR if needed EMS
 yet, clear airway again, and flick soles of feet. If still not breathing, give 2 breaths, check pulse and CPR if needed. EMS.")
10
Two most important concerns:
Airway & Breathing Preventing heat loss

11
Cutting the cord After drying and breathing has started
Make two ties: 4 inches from baby and 6 inches from baby Cut between

12
Placenta Delivery With infant wrapped up and breathing, and cord cut, place on mother’s abdomen Let placenta deliver passively!

13
Three things have to go to hospital:
Mother Baby Placenta

14
Surprises! (Complications)
See pdf file “Pregnancy and Childbirth” from TVI-CC Twins Prematurity More prone to airway/breathing problems & heat loss Breech Tush and feet appear first Footling breech- arm or leg appears first True obstetrical emergency Nuchal cord – cord around infant’s neck Slip over baby’s head Prolapsed cord – cord comes out first

15
Ectopic Pregnancy Female of child rearing age
Sudden onset of belly pain with no obvious cause Development of shock Treat shock and activate EMS

16
Basic Life Support

17
Remember the Basics: ABC’s rule all DDX and Tx in emergent conditions!
For multiple casualty triage: The dead stay dead. If you have a scene with three injured people and one is pulse-less and breathless – they are last priority. Remember the ‘scene survey’ – if it is not safe to respond don’t!

18
CPR Combines rescue breathing and chest compressions
Revives heart (cardio) and lung (pulmonary) functioning Use when there is no breathing and no pulse Provides O2 to the brain until ACLS arrives
 and lung (pulmonary) functioning. Use when there is no breathing and no pulse. Provides O2 to the brain until ACLS arrives.")
19
How CPR Works Effective CPR provides 1/4 to 1/3 normal blood flow
Rescue breaths contain 16% oxygen (21% - ambient air)
")
20
Start CPR Immediately Better chance of survival
Brain damage starts in 4-6 minutes Brain damage is certain after 10 minutes without CPR

21
Do Not Move the Victim Until CPR is Given and Qualified Help Arrives…
unless the scene dictates otherwise threat of fire or explosion victim must be on a hard surface Place victim level or head slightly lower than body

22
Even With Successful CPR, Most Won’t Survive Without ACLS
ACLS (Advanced Cardiac Life Support) ACLS includes defibrillation, oxygen, drug therapy
 ACLS includes defibrillation, oxygen, drug therapy.")
23
Survey The Scene, then: RAP
R - Responsiveness Tap shoulder and shout “Are you ok?”

24
RAP A - Activate EMS ( if unresponsive)
YOU - call 911 – come back and let me know what they said (another can stay by the phone) You may have to make the call
 You may have to make the call.")
25
P - Position on back RAP All body parts rolled over at the same time
Always be aware of head and spinal cord injuries Support neck and spinal column

26
ABCD Airway Breathing Circulation - Bleeding
Disability (keep this in mind from the beginning) If victim is unconscious but does display vital signs, place on left side
 If victim is unconscious but does display vital signs, place on left side.")
27
Checking Vital Signs A – Airway Open the airway Head tilt chin lift

28
B – Check For Breathing Look, listen and feel for breathing
No longer than 10 seconds seconds

29
Breathing If the victim is not breathing, give two breaths (1 second or longer) Pinch the nose Seal the mouth with yours If the first two don’t go in, re-tilt and give two more breaths (if breaths still do not go in, suspect choking)
")
30
Breathing: Mouth To Nose (when to use)
Can’t open mouth Can’t make a good seal Severely injured mouth Stomach distension Mouth to stoma (tracheotomy)
")
31
Compressions After giving breaths…
Locate proper hand position for chest compressions Place heel of one hand on center of chest between the nipples OR

32
Compressions Using both hands, give 30 chest compressions
Count 1, 2, 3 … Depth of compressions: 1 .5 to 2 inches For children: ½ to 1/3 of chest depth and use 1 or 2 hands (keep one hand on forehead if possible)
")
33
CPR If the victim starts moving: check breathing
After 30 chest compressions give: 2 slow breaths Continue until help arrives or victim recovers If the victim starts moving: check breathing

34
When Can I Stop CPR? Victim revives Trained help arrives
Too exhausted to continue Unsafe scene Physician directed (do not resuscitate orders) Cardiac arrest of longer than 30 minutes (controversial)
 Cardiac arrest of longer than 30 minutes. (controversial)")
35
Two Partner CPR Rescuer 1: Rescuer 2: Compression rate: 30:2
RAPAB (in charge of airway pulse and breathing) Rescuer 2: place hands for compressions Compression rate: 30:2 Switch off when tired 1 and 2…..4 and change
 Rescuer 2: place hands for compressions. Compression rate: 30:2. Switch off when tired. 1 and 2…..4 and change.")
36
Checking for CPR Effectiveness
Does chest rise and fall with rescue breaths? Have a second rescuer check pulse while you give compressions

37
Why CPR May Fail Delay in starting
Improper procedures (ex. Forget to pinch nose) No ACLS follow-up and delay in defibrillation Only 15% who receive CPR live to go home Improper techniques Terminal disease or unmanageable disease (massive heart attack)
 No ACLS follow-up and delay in defibrillation. Only 15% who receive CPR live to go home. Improper techniques. Terminal disease or unmanageable disease (massive heart attack)")
38
Injuries Related to CPR
Rib fractures Laceration related to the tip of the sternum Liver, lung, spleen

39
Complications of CPR Vomiting Aspiration Place victim on left side
Wipe vomit from mouth with fingers wrapped in a cloth Reposition and resume CPR

40
Stomach Distension Air in the stomach
Creates pressure against the lungs Prevention of Stomach Distension Don’t blow too hard Slow rescue breathing Re-tilt the head to make sure the airway is open Use mouth to nose method

41
Mouth to Mouth Barrier Devices
Masks Shields

42
Choking The tongue is the most common obstruction in the unconscious victim (head tilt- chin lift) Vomit Foreign body Balloons Foods Swelling (allergic reactions/ irritants) Spasm (water is inhaled suddenly)
 Spasm (water is inhaled suddenly)")
43
How To Recognize Choking
Can you hear breathing or coughing sounds? High pitched breathing sounds? Is the cough strong or weak? Can’t speak, breathe or cough Universal distress signal (clutches neck) Turning blue
 Turning blue.")
44
Recognizing Choking #2 A partial airway obstruction with poor air exchange should be treated as if it were a complete airway blockage. If victim is coughing strongly, do not intervene

45
Conscious Choking (Adult Foreign Body Airway Obstruction)
Give 5 abdominal thrusts (Heimlich maneuver) Place fist just above the umbilicus (normal size) Give 5 upward and inward thrusts Pregnant or obese? 5 chest thrusts Fists on sternum If unsuccessful, support chest with one hand and give back blows with the other Continue until successful or victim becomes unconscious
 Place fist just above the umbilicus (normal size) Give 5 upward and inward thrusts. Pregnant or obese 5 chest thrusts. Fists on sternum. If unsuccessful, support chest with one hand and give back blows with the other. Continue until successful or victim becomes unconscious.")
46
If You Are Choking And You Are Alone
Use fist Use corner of furniture Be creative

47
If Victim Becomes Unconscious After Giving Thrusts
Call 911 Try to support victim with your knees while lowering victim to the floor Assess Begin CPR After chest compressions, check for object before giving breaths breaths

48
You Enter An Empty Room And Find An Unconscious Victim On The Floor
What do you do? Assess the victim (RAPABC) Give CPR if needed After giving compressions: look for object in throat then give breaths
 Give CPR if needed. After giving compressions: look for object in throat. then give breaths.")
49
CPR for Infants (Under 1 Year of Age)
Same procedures (RAPAB) except: Seal nose and mouth or nose only Give shallow “puffs”
 except: Seal nose and mouth or nose only. Give shallow puffs")
50
CPR: Infants RAPAB Give CPR 30 compressions to 2
Press sternum 1/2 to 1/3 depth of the chest Use middle and ring finger 30 compressions to 2 If alone, resuscitate for 2 minutes then call 911

51
Choking: Conscious Infants
Position with head downward 5 back blows (check for expelled object) 5 chest thrusts (check for expelled object) Repeat
 5 chest thrusts (check for expelled object) Repeat.")
52
Choking: Unconscious Infants
If infant becomes unconscious: RAPAB When the first breaths don’t go in, check for object in throat then try 2 more breaths. If neither set of breaths goes in, suspect choking Begin 30 compressions Check for object in throat (no blind finger sweep) Give 2 breaths
 Give 2 breaths.")
53
Guidelines for Dealing with Children
Get parental consent (implied in emergency) Involve the parent(s)? Talk TO child Try to be close to eye level Don’t lie or surprise!
 Involve the parent(s) Talk TO child. Try to be close to eye level. Don’t lie or surprise!")
55
Child Abuse: Treat and Notify Police or County Protective Services
Wounds in different stages of healing Wounds that suggest defensive posturing Hands and forearms Back, back of head,back of legs “Unusual” explanation

56
Injection Therapies

57
Peripheral Injections

58
Peripheral Injection Complications
Abscess: Post injection infection. Contaminated infusate or “dirty” stick. Antibiotic Tx, Heat, and I&D are possible. Broken needle: Why you don’t bury the needle to the hub. Prevent by pre inspection, and not flexing the needle during use. Hematoma: Leaky veins post injection. Use post injection direct pressure to slow this down. Watch anticoagulant patients. Post treatment pain: Typically from tissue fullness.Movement, Ice, or alternating hot and cold help. Shock / Syncope: Remember, this may be vaso-vagal effect or may be actually due to some component of the injection. Glycemic emergency?: Consider this in those with prior blood sugar problems, as well as high dose Vitamin-C (Hypoglycemic reaction) and Corticosteroid Hyperglycemic reactions) injections. Anaphylaxis: Always possible. If unsure about a medicine, either do not use it, run an interdermal test on it, or premedicate the patient to negate the IgE effects. (See below for treatment)
 and Corticosteroid Hyperglycemic reactions) injections. Anaphylaxis: Always possible. If unsure about a medicine, either do not use it, run an interdermal test on it, or premedicate the patient to negate the IgE effects. (See below for treatment)")
59
Injection Procedures - 1
Injectate Inspect vial for particles / film / cracks etc… Check expiration date Clean stopper with alcohol Syringe / Needle Ample size for total injectate volume Draw with large bore needle Ideally, drawing needle should be different from injecting needle Draw with 21 – 18 gauge for fastest draw (some solutions are thicker than others). Also Filtered needles and “NoCor” needles available. Exceptions are small volume single medicine injections (B12/Insulin…) Drawing up injectate Wash hands Insert needle into vial Inject air to equal volume to be withdrawn (except in DMPS vials) Draw prescribed volume into syringe Remove needle from vial / one handed “soft” re-cap or hemostat change
. Also Filtered needles and NoCor needles available. Exceptions are small volume single medicine injections (B12/Insulin…) Drawing up injectate. Wash hands. Insert needle into vial. Inject air to equal volume to be withdrawn (except in DMPS vials) Draw prescribed volume into syringe. Remove needle from vial / one handed soft re-cap or hemostat change.")
60
Injection Procedures - 2
IM Sites Deltoid Adults and some children over 2 Vastus lateralis (Thigh) Preferred for children under 2 Gluteus maximus (Hip) In adults, larger muscle for larger quantities or thicker solution IM procedure Wash hands / Glove up / Prep patients skin Place injecting needle on syringe / Remove cap from needle Stabilize patient skin with one hand and hold the syringe like a dart or a pencil with the other Enter skin quickly at a 90 degree angle / Stop ½ to 1 cm prior to hub of needle Aspirate** / Inject material slowly, then withdraw the needle Cotton ball to injection site / Dispose of syringe in sharps / Bandage patient
 Preferred for children under 2. Gluteus maximus (Hip) In adults, larger muscle for larger quantities or thicker solution. IM procedure. Wash hands / Glove up / Prep patients skin. Place injecting needle on syringe / Remove cap from needle. Stabilize patient skin with one hand and hold the syringe like a dart or a pencil with the other. Enter skin quickly at a 90 degree angle / Stop ½ to 1 cm prior to hub of needle. Aspirate** / Inject material slowly, then withdraw the needle. Cotton ball to injection site / Dispose of syringe in sharps / Bandage patient.")
61
Subcutaneous injection:

62
Subcutaneous injection-2
In addition to other injection procedures you already know: Pinch up a quantity of skin Inject into the elevated area (SQ) degrees
 degrees.")
63
Intradermal Injection:
Injection site The usual choice of site is the anterior forearm. However, the upper chest, upper arm or shoulder can also be used. Administration of drug or antigen Wash and dry visibly soiled skin. Hold the middle of the patient's forearm in your non-dominant hand, anterior side up. Pull the anterior skin taut with your thumb and forefinger. Insert the needle under the outer layer of the skin at an angle of 10-15°. Slowly administer injection, observing for wheal formation to show medication has entered the dermis. Withdraw needle and wipe skin gently. Do not rub or apply pressure as this may disperse the medication into surrounding tissue.

64
IV Therapy

65
Solution Guidelines: IV Admixtures
Due to potential for phlebitis / vein injury, the following guidelines are common for IV admixtures delivered through peripheral (NOT Central) IV placement: pH: “5-9” (Human blood is pH ) Acidic range: OK to 5 pH or higher Alkaline range: Do not exceed 9 pH Patient comfort max at 6.6 – 7.6
 IV placement: pH: 5-9 (Human blood is pH ) Acidic range: OK to 5 pH or higher. Alkaline range: Do not exceed 9 pH. Patient comfort max at 6.6 – 7.6.")
66
Solution Guidelines: IV Admixtures
Osmolarity: : Low risk of phlebitis : Moderate risk of phlebitis 600 + : % risk of some phlebitis (Gazitua, et al) ** Remember: changing osmolarity (dilution) does not change pH. Both need to be assessed. ** Changes that can be made include: Slow the IV Increased solution (dilution) Buffering additions (Bicarbonate or HCl) Using the largest vein available Watching catheter tip placement
 ** Remember: changing osmolarity (dilution) does not change pH. Both need to be assessed. ** Changes that can be made include: Slow the IV. Increased solution (dilution) Buffering additions (Bicarbonate or HCl) Using the largest vein available. Watching catheter tip placement.")
67
IV – Local Complications
Hematoma: Fragile veins, elderly pt., poor technique. Use small gauge device (catheter whenever possible) Educate high risk patients Pressure bandage Thrombosis: Clot due to endothelial trauma. Technique can play a role (Vein damage). Watch for slow / stopped flow rate. D/C the line, apply ice / pressure. This is rare in short term infusions.
 Educate high risk patients. Pressure bandage. Thrombosis: Clot due to endothelial trauma. Technique can play a role (Vein damage). Watch for slow / stopped flow rate. D/C the line, apply ice / pressure. This is rare in short term infusions.")
68
IV – Local Complications
Phlebitis: Common. Osmolarity, flow rate, catheter size and placement all play a role. Redness / swelling of the vein. Vein may stay “ropy” for some time after (10 – 40 days). Vein may sclerose. 4 Grades of phlebitis Use large vein for hypertonic solutions (ie. not the hand) Buffer solutions Tx.: Prevention, Flush with NS, D/C line, apply ice. Thrombophlebitis: Phlebitis with thrombosis. Same causes. More rare in short infusions. Treatment is the same as for both.
. Vein may sclerose. 4 Grades of phlebitis. Use large vein for hypertonic solutions. (ie. not the hand) Buffer solutions. Tx.: Prevention, Flush with NS, D/C line, apply ice. Thrombophlebitis: Phlebitis with thrombosis. Same causes. More rare in short infusions. Treatment is the same as for both.")
69
IV – Local Complications
Infiltration / Extravasation: Fluid flowing into the subcutaneous tissues. Area becomes swollen, cool, and typically painful. Flow rate slows. STOP infusing and gain access! Light pressure, Ice, Apis (hp) Local infection: Same as abscess formation above.
 Local infection: Same as abscess formation above.")
70
IV – Local Complications
Venous spasm: Smooth muscle in vein wall / autonomic nervous system create spasm. May be due to irritating / hyperosmotic pH unbalanced or COLD solutions. Pain at site that travels up the arm. Slow flow, warm solution, flush line, check (RECHECK) pH, heat on arm, check arm position. Hypersensitivity reactions: Allergic reaction to solution components. See below. LINE FLUSHING PROTOCOLS: Saline: Slow flush through port with flow of IV stopped. No smaller than 10 cc syringe!! Procaine / Lidocaine: 1 or 2% drug (1cc.) in 9 cc NS. SLOW push!!!!
 pH, heat on arm, check arm position. Hypersensitivity reactions: Allergic reaction to solution components. See below. LINE FLUSHING PROTOCOLS: Saline: Slow flush through port with flow of IV stopped. No smaller than 10 cc syringe!! Procaine / Lidocaine: 1 or 2% drug (1cc.) in 9 cc NS. SLOW push!!!!")
71
IV – Systemic Complications
Septicemia: Systemic infection. BAD! Contaminated solution / equipment etc. OBTAIN BLOOD CULTURES! Toxic patient, fever / malaise / N-V-D / etc. Tx with Immune support, ABX etc. Fluid overload: Infusing an ISOTONIC solution too quickly. Watch the elderly and those with compromised kidney function. Edema, Hypertension, Pulmonary edema (SOB & Crackles) Tx: Slow fluid infusion Heat to dilate peripheral circulation O2 administration
 Tx: Slow fluid infusion. Heat to dilate peripheral circulation. O2 administration.")
72
IV – Systemic Complications
Pulmonary edema: Typically in those with CVD or Renal Dz. Fluid overload causes Left heart inability to remove fluid from the lungs. Tx is same as fluid overload. Air embolism: Air infusion that collects in the right side of the heart. Typically associated with electric pumps. “MILL WHEEL MURMUR” may be present. Respiratory, affective, and neurological findings It takes 10 to 60 cc of air to kill a human. If air gets to the right ventricle and up to the Pulmonic valve it will occlude flow to the lungs. Tx: LEFT LATERAL DECUBITUS POSITION! O2. Monitor vitals. EMS transport to ER.

73
IV – Systemic Complications
Speed shock: Rapid administration of a Medication / Vitamin or Mineral that causes a sudden rise in the plasma concentration of the substance. i.e. Magnesium pushed too fast causes BP to drop… Dilution, slow pushes, and patient interaction are the best prevention. Catheter embolism: Shearing off of the end of the catheter. It will travel through the venous system and embolize. Save the rest of the catheter. Digital pressure proximal from the site / and-or tourniquet application. Radiological exam / ER visit needed. NOT advancing and retracting the catheter over the needle (even prior to insertion) prior to removal of the needle is key!
 prior to removal of the needle is key!")
74
IV – Systemic Complications
Electrolyte (Macro-mineral) Shift: Administration of Ca / K / Mg individually typically can predispose a patient to a “hyper” state. Patient may show muscle cramping signs, or signs of hyperkalemia. Mg. And Ca. “push” syringes should be kept as antidote May be a side effect of chelation therapy (See chelation notes) Glycemic emergency: Have patients eat during high Vitamin C infusions and EDTA chelation. D5W infusion, or slow push of D50 (5cc D50 in 5 cc sterile water) will reverse.
 Shift: Administration of Ca / K / Mg individually typically can predispose a patient to a hyper state. Patient may show muscle cramping signs, or signs of hyperkalemia. Mg. And Ca. push syringes should be kept as antidote. May be a side effect of chelation therapy (See chelation notes) Glycemic emergency: Have patients eat during high Vitamin C infusions and EDTA chelation. D5W infusion, or slow push of D50 (5cc D50 in 5 cc sterile water) will reverse.")
75
Emergency Protocols Assess ABC’s Etiology:
Airway Breathing Circulation Etiology: Speed shock / Hypersensitivity… What do you really need to treat? EMS or not: Your call. You are the Dr. in charge.

76
Emergency Protocols Respond First assure ABC’s stable
Response based on supposed etiology Syncope Speed Shock Glycemic emergency Anaphylaxis MI Other

77
Emergency: Syncope Patient in Trendelenberg position
NOTE: Some hospitals no longer include in their standard protocols. DO NOT D/C THE I.V. LINE!!! Slow (stop) infusion rate Talk to them (if conscious) Have them move their feet
 infusion rate. Talk to them (if conscious) Have them move their feet.")
78
Emergency: Syncope Smelling salts if unconscious Cover with blanket
Watch for “re-entry” seizure activity Reassure them and others present Continue infusion if warranted

79
Emergency: Speed Shock
Trendelenberg position in some cases STOP the infusion – do not D/C the line! Infuse NS Treat acute symptoms of the overdose Administer antidote if necessary

80
Fluid overload: Infusing an ISOTONIC solution too quickly.
Watch the elderly and those with compromised kidney function. Edema, Hypertension, Pulmonary edema (SOB & Crackles) Tx: Slow fluid infusion Heat to dilate peripheral circulation O2 administration
 Tx: Slow fluid infusion. Heat to dilate peripheral circulation. O2 administration.")
81
IV Fluid Dynamics Isotonic Hypotonic Hypertonic Increases volume
Effect on intravascular compartment (blood) Increases volume Dehydrates – moves fluid to cells Greatly increases volume – dehydrates cells Fluid overload potential Incr. in Ki / Li patients, and the elderly Moderate potential [ D5W] No High potential D5W (without other additives) starts Isotonic but can act hypotonic if the patient metabolizes the sugar quickly.
 Increases volume. Dehydrates – moves fluid to cells. Greatly increases volume – dehydrates cells. Fluid overload potential. Incr. in Ki / Li patients, and the elderly. Moderate potential. [ D5W] No. High potential. D5W (without other additives) starts Isotonic but can act hypotonic if the patient metabolizes the sugar quickly.")
82
Glycemic Emergency Hyper: Hypo:
Ie. Steroid injection / D5 – D50 too fast Watch and wait if appropriate with patient recumbent Administer NS or ½ NS Insulin (SQ or IV) if appropriate Hypo: Prevention Watch High dose Vitamin C, EDTA… D5W administration or “50/50 mix” D50 & Water Administer IV in a D5 base if patient is a recurrent reactor
 if appropriate. Hypo: Prevention. Watch High dose Vitamin C, EDTA… D5W administration or 50/50 mix D50 & Water. Administer IV in a D5 base if patient is a recurrent reactor.")
83
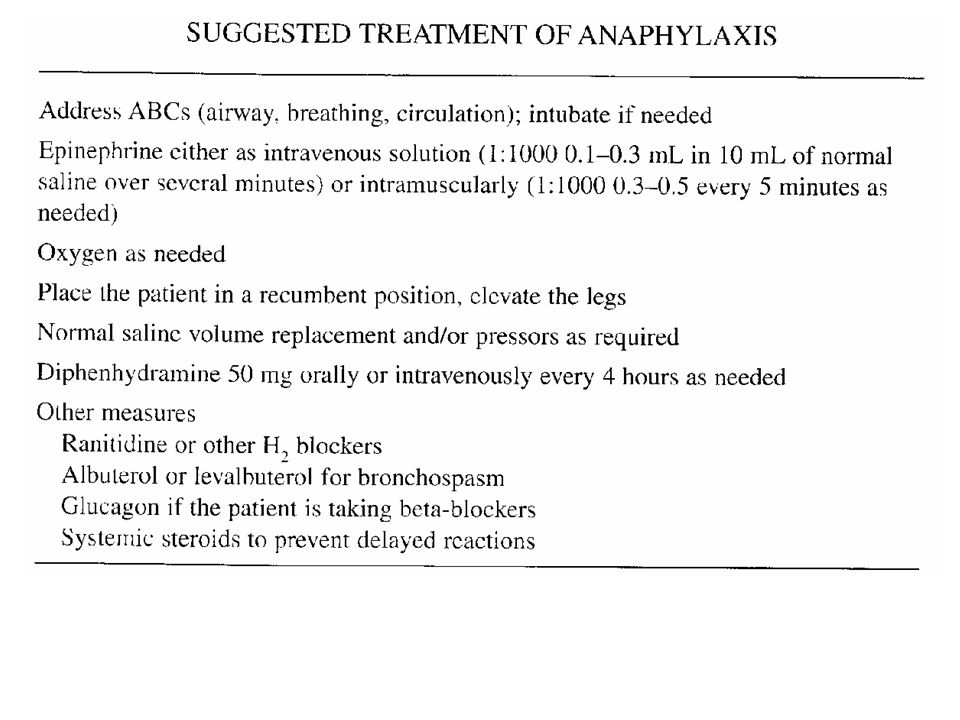
Emergency: Anaphylaxis See also emergency handout.
Initial Sn / Sx: Apprehension / urticaria / edema / throat sensation Severe cases: Hypotension LOC Mydriasis Incontinence Convulsion Sudden Death STOP the infusion but DO NOT D/C THE LINE!!! Change Bag and Line to NS infusion and run in

84
Emergency: Anaphylaxis
Patient in Trendelenberg position Assess ABC’s Airway must be patent – insert airway if needed If patient not breathing, administer ‘Ambu’ or Rescue breaths Assess peripheral (emergency) blood pressure Radial pulse = AT LEAST 80 Systolic Femoral pulse = AT LEAST 70 Systolic Carotid pulse = AT LEAST 60 Systolic
 blood pressure. Radial pulse = AT LEAST 80 Systolic. Femoral pulse = AT LEAST 70 Systolic. Carotid pulse = AT LEAST 60 Systolic.")
85
Emergency: Anaphylaxis
Treat: BENEDRYL: 50 mg (1ml) IV stat Note: this is not normally done before Epi. Epinephrine: KNOW THE CONCENTRATION!!!!!! 1:1000 is IM / SQ and Intratrachial ONLY!! Use 0.3 to 1 cc IM / SQ Immediately if this is the type you have 1:10,000 is the IV form IV administer 3 cc and wait. May give all 10 cc. Oxygen High Concentration (~15 L / min) by mask. (3 L / min in COPD)
 IV stat. Note: this is not normally done before Epi. Epinephrine: KNOW THE CONCENTRATION!!!!!! 1:1000 is IM / SQ and Intratrachial ONLY!! Use 0.3 to 1 cc IM / SQ Immediately if this is the type you have. 1:10,000 is the IV form. IV administer 3 cc and wait. May give all 10 cc. Oxygen High Concentration (~15 L / min) by mask. (3 L / min in COPD)")
86
Emergency: Anaphylaxis
Steroids – Stabilize cytokine storm: mg (2.5 to 5 cc) Solu-Cortef 100 – 500 mg Solu-Medrol mg Calcium Gluconate - To reverse hypocalcemia: up to 10 ml (1G) / 2 min X3 then 1G in 500 ml NS Magnesium Sulfate For spasm or Calcium overdose: 1G / 1-2 min. then 5G in 250 –500 NS Albuterol / Aminophylline: Limited help / use if you have.
 Solu-Cortef 100 – 500 mg. Solu-Medrol mg. Calcium Gluconate - To reverse hypocalcemia: up to 10 ml (1G) / 2 min X3 then 1G in 500 ml NS. Magnesium Sulfate. For spasm or Calcium overdose: 1G / 1-2 min. then 5G in 250 –500 NS. Albuterol / Aminophylline: Limited help / use if you have.")
87
Osmolarity Osmolarity: The concentration of solute in a volume of solution Osmolarity of human body fluids mOsm/L (Average 290) Tonicity of solutions infused Isotonic: 250 – 375 mOsm/L Hypotonic: Below 250 mOsm/ml Hypertonic: Above 375 mOsm/L
 Tonicity of solutions infused. Isotonic: 250 – 375 mOsm/L. Hypotonic: Below 250 mOsm/ml. Hypertonic: Above 375 mOsm/L.")
88
Osmolarity – Solution Dynamics
Isotonic: 250 – 375 mOsm/L Normal Saline (0.9% Sodium Chloride / NS) 5% Dextrose in Water (D5W) Ringer’s Lactate (Balanced electrolyte solution) Do not cause fluid shifts (between compartments) so they may cause circulatory overload (over expanded vascular compartment and dilution of the cellular component of the blood)
 5% Dextrose in Water (D5W) Ringer’s Lactate (Balanced electrolyte solution) Do not cause fluid shifts (between compartments) so they may cause circulatory overload (over expanded vascular compartment and dilution of the cellular component of the blood)")
89
Osmolarity – Solution Dynamics
Hypotonic: Below 250 mOsm/L 0.45% Sodium Chloride (1/2 NS) Lowers plasma osmolarity, so fluid leaves blood compartment and goes to cellular compartment. Hydrates cells / Lowers serum Sodium Can cause hypotension
 Lowers plasma osmolarity, so fluid leaves blood compartment and goes to cellular compartment. Hydrates cells / Lowers serum Sodium. Can cause hypotension.")
90
Osmolarity – Solution Dynamics
Hypertonic: Above 375 mOsm/L D10 and D20 infusions Most vitamin / Mineral infusions given (May be 500 to mOsm/L) Shift fluid into the plasma compartment – can cause circulatory overload IRRITATING TO THE VEIN WALLS MAY BE PAINFUL Give at slow rate: 1 to 5 ml/min.
 Shift fluid into the plasma compartment – can cause circulatory overload. IRRITATING TO THE VEIN WALLS. MAY BE PAINFUL. Give at slow rate: 1 to 5 ml/min.")
91
Osmolarity - Calculation
{[(Volume) X (mOsm/ml)] / (Volume)} X 1000 Example: Component: Volume, ml mOsm/ml (Volume X mOsm/ml) Ascorbic acid, 500 mg/ml Sodium Bicarbonate, 8.4% Sterile Water for injection ================================================================== Totals ////////// Solution Osmolarity = {[890.0] / 410.0} X 1000 = So this would be a very hyperosmolar solution…
 X (mOsm/ml)] / (Volume)} X Example: Component: Volume, ml mOsm/ml (Volume X mOsm/ml) Ascorbic acid, 500 mg/ml Sodium Bicarbonate, 8.4% Sterile Water for injection ================================================================== Totals 410 ////////// Solution Osmolarity = {[890.0] / 410.0} X 1000 = So this would be a very hyperosmolar solution…")
92
Base IV Solutions - 1 Dextrose in Water
D5W: 5% Dextrose in Water. ISOTONIC. 1.5 to 2 liters / day average. Good for mixing solutions in. Used in cancer therapies. D10/20/50: Lowers Potassium. HYPERTONIC. Glucose support. Sodium Chloride 0.45% HYPOTONIC 0.9% ISOTONIC 3% / 5% HYPERTONIC

93
Base IV Solutions - 2 Dextrose and Sodium Chloride D5 and 0.9%NaCl
ISOTONIC 2.5 % or 5% Dextrose and 0.2% or 0.45 % NaCl HYPERTONIC Sterile Water (HYPOTONIC) Good for mixing high osmolarity solutions. NEVER infuse alone. RBC Lysis results. Electrolyte Solutions (ISOTONIC) *Check for incompatibilities with additives. Ringer’s: Electrolyte replenisher. For dehydration. Ringer’s Lactate: “Hartmann’s solution”. Very similar to the ECF electrolytes. Do not use in Addison’s or liver disease where lactate metabolism is impaired.
 Good for mixing high osmolarity solutions. NEVER infuse alone. RBC Lysis results. Electrolyte Solutions (ISOTONIC) *Check for incompatibilities with additives. Ringer’s: Electrolyte replenisher. For dehydration. Ringer’s Lactate: Hartmann’s solution . Very similar to the ECF electrolytes. Do not use in Addison’s or liver disease where lactate metabolism is impaired.")
94
Chelation Issues

95
Chelation: Cautions and contraindications
Medications: Calcium channel blockers and EDTA will have additive cardiac blockade effects. (Ca-EDTA less so than Na-EDTA – but both are a concern) Magnesium also has added Ca-Blockade. Use with caution, and titrate the dose slowly in patients on Ca-Blocking meds.
 Magnesium also has added Ca-Blockade. Use with caution, and titrate the dose slowly in patients on Ca-Blocking meds.")
96
Chelation: Cautions and contraindications
Renal insufficiency Mild to Moderate: Lower dose, and treat no more than once weekly. Severe: Contraindicated. Liver disease Monitor closely in patients with mild to moderate Liver enzyme elevation Severe Liver disease is a contraindication. Active Hepatitis B&C are relative contraindications. Anticoagulation Pro-times must be monitored closely as EDTA may change clotting time. Congestive heart failure All cardiac parameters must be monitored closely. Baseline EKG etc. Calcium levels should be assessed every four weeks Pregnancy Contraindicated

97
Airway Management Anaphylaxis Shock

98
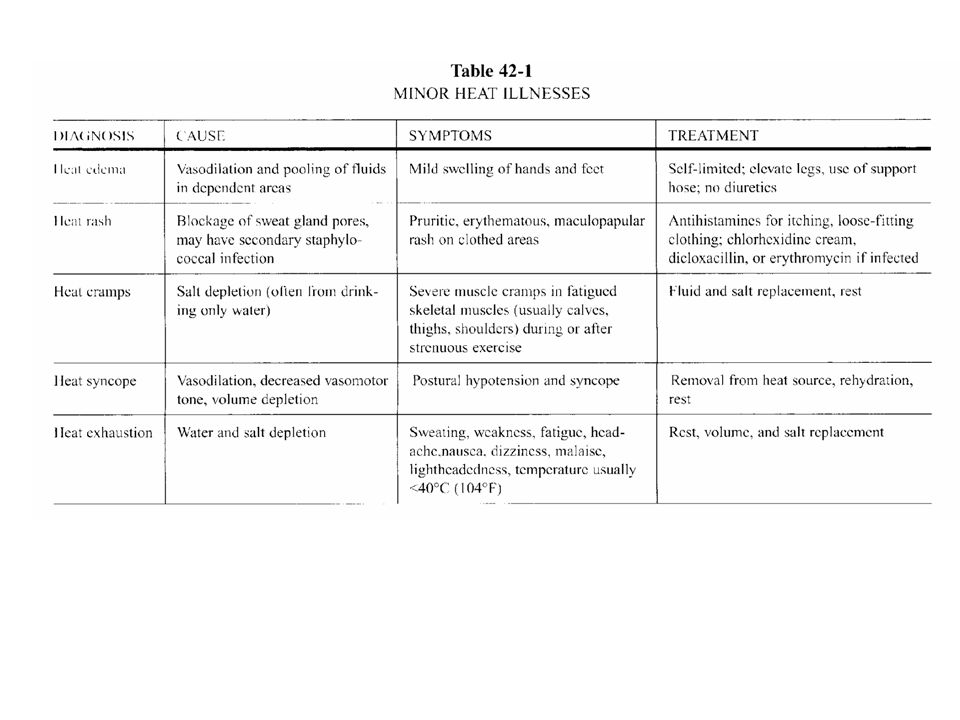
Croup – inflammation of the larynx, trachea, and bronchi
Usually between 3 months and 3 years Usually while asleep Complication of viral infection Difficulty breathing Crowing sound on inspiration (inspiratory stridor) Seal-like barking cough Breath cool moist air for 5 minutes If no improvement after 5 minutes continue to monitor If condition worsens transport to hospital
 Seal-like barking cough. Breath cool moist air for 5 minutes. If no improvement after 5 minutes continue to monitor. If condition worsens transport to hospital.")
99
Epiglottitis Usually between 3 –10 years
Caused by H. influenza (or occasionally a beta hemolytic Strep) infection High fever / Toxic Child Difficulty breathing Inspiratory stridor Drooling Try moist air breathing Will need antibiotics and Airway management! Do not move neck or open mouth EMS Transport to ER
 infection. High fever / Toxic Child. Difficulty breathing. Inspiratory stridor. Drooling. Try moist air breathing. Will need antibiotics and Airway management! Do not move neck or open mouth. EMS Transport to ER.")
103
Acute Airway ; Anaphylaxis
Signs of Allergic Reaction Strange sensations in patient Affected respiration (laryngeal edema) Edema, errythema, allergic dermatitis Treatment Epinephrine IM mg/ml (1:1,000), Subcutaneous ml IV push mg (1-2 ml) (1:10,000) Can repeat Q 3-5 min Diphenhydramine 25-50mg IM or IV push
 Edema, errythema, allergic dermatitis. Treatment. Epinephrine. IM mg/ml (1:1,000), Subcutaneous ml. IV push mg (1-2 ml) (1:10,000) Can repeat Q 3-5 min. Diphenhydramine mg IM or IV push.")
104
Oxygen Delivery Systems
Nasal Cannula Easiest to wear, on demand or continuous Lowest flow rates-up to 6 lpm=20-40% O2 Simple Mask 6-10 lpm gives approximately 40-60% O2 Partial/Non Rebreather Mask Partial has air release valves, NRB-one way valve only For liter flows % O2 Usually used in Acute Emergency situations Venturi Mask Used if specific flow is needed Valves for 25-50% O2 Ambu Bag/Mask For Emergency situations requiring manual ventilation of pt

105
Upper Airway Obstruction
All Patient presentations include inspiratory and/or expiratory Stridor (high pitched sounds) Possible retractions of the thorax Intercostal, suprasternal, supraclavicular Cyanosis (later stage) Drooling (common in pediatrics) LOC with full obstruction
 Possible retractions of the thorax. Intercostal, suprasternal, supraclavicular. Cyanosis (later stage) Drooling (common in pediatrics) LOC with full obstruction.")
106
Upper Airway Obstruction:Tx
Determine if obstruction is mechanical or infectious! If mechanical; Do Heimlich procedure If infectious; consider Epiglottitis Usually found in pediatrics Sudden onset Pt can’t swallow properly/Drooling common Tripod position Swollen airway, infectious signs of fever/malaise

109
What is Shock? The state of metabolic failure that may be caused by either inadequate delivery of oxygen to the tissues or improper metabolism of oxygen at the tissue site Types Early (compensated) reversible in nature General sympathetic nervous system reaction to causative factors, body is compensating Late (decompensated) difficult to reverse effects System is unable to maintain sympathetic responses to causative effects, starts to decompensate and go into failure mode
 reversible in nature. General sympathetic nervous system reaction to causative factors, body is compensating. Late (decompensated) difficult to reverse effects. System is unable to maintain sympathetic responses to causative effects, starts to decompensate and go into failure mode.")
110
Shock Severity Determinants
Compensated Shock Mechanism Signs/symptoms Tachycardia, anxiety, restlessness, apprehension, delayed capillary refill, diaphoresis, widened pulse pressure Treatments are preventative in nature with ABC interventions Decompensated Shock Mechanism Signs/symptoms Hypotension, confusion, Loss of consciousness, oliguria, acidemia Treatments is aggressive and rapid volume resuscitation, medications and invasive procedures Hypotension is a later sign. Tachycardia is an early sign.

111
Signs of Shock Tachycardia Hypotension Adrenergic responses
Earliest signs of shock Hypotension Late sign of shock Adrenergic responses Restless, agitated cool clammy skin “livedo reticularis”-mottled skin Altered Mental Status Orthostatic Vital Signs Problems occur in standing position, often resolve supine

112
Classification of Shock
Hypovolemic Shock Due to a loss of fluids Cardiogenic Shock Cardiac obstruction or pump failure, MI Obstructive Shock Significant fall in cardiac output, CHF Distributive Shock Loss of intravascular and decreased vascular volume; Neurogenic, sepsis, infectious problem

113
Glasgow Coma Scale Revised Trauma Score Eye opening
Spontaneous To verbal command To pain None Verbal Responsiveness Orientated Confused Inappropriate words Incomprehensible Motor Response Obeys commands Localizes pain Withdraws Flexion Extension Revised Trauma Score Respiratory rate (breaths per min) > Systolic BP (mmHg) > No pulse Glasgow conversion scale <
 > Systolic BP (mmHg) > No pulse 0. Glasgow conversion scale < 0.")
114
Seizure Remember: Epilepsy is a clinical diagnosis of exclusion to be sure that the seizure is not from: Infection Mass / CA Electrolyte imbalance Etc…

115
Seizures (Tonic-Clonic)
Most common are febrile Toxin ingestion Treat as any seizure and get follow up medical care Protect patient during seizure to the degree possible See Neuro Notes for other DDX with seizure.

116
Head Injuries and Trauma
All patients with head injuries and trauma should be treated as if they are positive for cervical spinal injury C-spine immobilization Cervical Collar Head blocks Long board Treat with ABC’s, Glasgow Coma Scoring and Neurological exam techniques All head injury patients require 100% O2 therapy Conscious pts with adequate respirations-Non-rebreather Unconscious or impaired respirations-Bag valve mask

117
Head Injury-special considerations
Associated Symptoms Seizures Considered in GCS <8, cerebral contusion, depressed skull fracture, intracranial hematoma, penetrating head wound Combativeness Evaluate for hypoxia, hypoglycemia, hypotension and pain Pain Control Sedatives-analgesics (narcotics, benzodiazepines) Systemic Hypertension Signs of Intracranial Pressures Bradycardia & hypertension
 Systemic Hypertension. Signs of Intracranial Pressures. Bradycardia & hypertension.")
118
Neck and Spinal Trauma Airway management Cervical stabilization
Penetrating wounds “Leave it there”-knife, sharp objects Underlying anatomical areas Nerve involvement (test cranial) Whiplash Injuries (cervical strain) Hyperextension injury most common No associated fractures X-ray is diagnostic 12-24 hrs for manifestation of symptoms
 Whiplash Injuries (cervical strain) Hyperextension injury most common. No associated fractures. X-ray is diagnostic hrs for manifestation of symptoms.")
119
Trauma and Bleeding Primary Survey/Circulation Establish Homeostasis
Assess any obvious hemorrhage Apply indirect homeostasis measures Apply pressure to wound Graded pressure with pressure bandages Elevate injury above level of heart Vaso-constrictive measures Not more than 30mm Hg (blood pressure cuff)
")
120
Wound Assessment Detailed wound info Time of occurrence
Reduced bacteria in first 6 hours (closure) Increased blood supply lengthens exposure time (facial wounds up to 24 hrs) Exposure of wound Possible environmental contaminants Mechanism of injury Instrument of injury Fragmental mechanisms Chemical exposure Cold can extend tissue integrity
 Increased blood supply lengthens exposure time. (facial wounds up to 24 hrs) Exposure of wound. Possible environmental contaminants. Mechanism of injury. Instrument of injury. Fragmental mechanisms. Chemical exposure. Cold can extend tissue integrity.")
121
Types of Wounds Lacerations Puncture Stretch Injuries
Minimal tissue injury Reduced risk of infection Puncture High risk of infection Check for foreign bodies Stretch Injuries Damage to blood vessels, nerves, ligaments, tendons Damage may not be visual on inspection Crush/Compression Highest level of tissue necrosis Hemorrhage risk Difficult for tissue to heal due to trauma Bites Highest risk of infection Often requires delayed closure of wound to allow drainage Irrigation necessary

122
Wound Management Wound closure Contra-indications to closure
Heavy bacterial infection Needs irrigation, antibiotic therapy Major tissue defects Debridement of dead tissue Excessive tension on wound Foreign body Devitalized tissue Primary Closure Suture or butterfly adhesive suture closure Secondary Closure Wound heals from inside No primary closure done due to infection risk

123
Wound Management Wound Risk Assessment Infection Healing Processes
Puncture, crush injuries Environmental risks Tetanus Usually deep puncture with soil exposure Wash wound with antibacterial soap immediately Immunization hx Q 10 yrs, shots if exposure risk is high Rabies Consider rabies immune globulin USP Healing Processes Thickening around wound x 3 months Errythema around scar x 3-6 months Keloid or hypertrophic scar formation risk Acupuncture around scar post healing “Surround the dragon” technique

124
Burn Injury Assessment
Severity of Injury Burn Size Rule of Nines (adults)=100 9=each arm, head/neck 18=each side of torso, each leg Genitalia and perineum=1 Rule of Fives (pediatrics)=100 10=each arm, and infant leg 15=head/neck of child and each leg 20=infant head/neck, child side of torso No value for peds genitalia
=100. 9=each arm, head/neck. 18=each side of torso, each leg. Genitalia and perineum=1. Rule of Fives (pediatrics)= =each arm, and infant leg. 15=head/neck of child and each leg. 20=infant head/neck, child side of torso. No value for peds genitalia.")
125
Rule of Nines/Fives

126
Burn Assessment Burn Depth Superficial (1st degree)
Mild errythema, heals spontaneously Partial thickness (2nd degree) Heals spontaneously Blistering, errythema Deep Partial Thickness burns might need grafting to decrease contractures and hypertrophic scarring Full-thickness (3rd degree) Deep past skin layers Damage to nerves, vessels Loss of sensation common Needs grafting
 Heals spontaneously. Blistering, errythema. Deep Partial Thickness burns might need grafting to decrease contractures and hypertrophic scarring. Full-thickness (3rd degree) Deep past skin layers. Damage to nerves, vessels. Loss of sensation common. Needs grafting.")
127
Burn Assessment Major Burn Injuries Moderate Uncomplicated Burn Injury
2nd degree >25% BSA (adults) 2nd degree >20% BSA (peds) 3rd degree >10% BSA Most burns of face, hands, eyes, ears, feet, perineum Inhalation, Electrical, major trauma Poor risk patients (adults >55yrs , peds< 5yrs) Moderate Uncomplicated Burn Injury 2nd degree 15-25% BSA adults 2nd degree 10-20% BSA peds 3rd degree <10% BSA Know these numbers!
 2nd degree >20% BSA (peds) 3rd degree >10% BSA. Most burns of face, hands, eyes, ears, feet, perineum. Inhalation, Electrical, major trauma. Poor risk patients (adults >55yrs , peds< 5yrs) Moderate Uncomplicated Burn Injury. 2nd degree 15-25% BSA adults. 2nd degree 10-20% BSA peds. 3rd degree <10% BSA. Know these numbers!")
128
Burn Assessment Location of Burns Hands and Feet Face Eyes Ears
Can cause scarring and disability Face Associated with inhalation injury Physical/emotional injury Eyes Corneal scarring Quick assess-periorbital edema is eminent Ears Pressure deformity Infection risk Perineum High risk of infection

129
Burn Assessment Types of Burns Circumferential Inhalation
Considered major injury Lymphatic/venous obstruction Increased tissue pressure/edema Look at structures affected in area Inhalation Confined spaces Soot around nares Stridor, hoarseness, respiratory distress Carboxyhemoglobin level >10% Consider Intubation quickly

130
Burn Assessment Electrical Burns Types
Lightning Burns Linear, Punctate, Feathering, Thermal Electrical Shock Alternating house current is most dangerous Extensive internal injury/damage Labs-Myloglobinuria present (tissue breakdown) Renal damage Associated Injury-Fractures Hemorrhage, Internal injuries
 Renal damage. Associated Injury-Fractures Hemorrhage, Internal injuries.")
131
Burn Assessment Chemical Burns Determine type of chemical exposure
Take personal precautions for exposure Face mask gloves Remove chemical if possible Powder-brush off Liquid-see poisoning chart Remove associated clothing if smoldering or exposed to chemical Consider inhalation injury (treat airway) Treat wound appropriately to protect skin integrity and underlying structures
 Treat wound appropriately to protect skin integrity and underlying structures.")
132
Burn Treatment Ventilation and Oxygenation Intravenous Access
Non-rebreather, 100%-15 lpm or Bag Valve mask if impeded respiration If inhalation injury suspected, consider intubation to protect airway Intravenous Access Necessary in patients with 15% or more body surface area burns Due to cellular fluid loss At least one large bore IV (>16 gauge) Insert thru non-burned skin Central venous access used for large burns
 Insert thru non-burned skin. Central venous access used for large burns.")
133
Fluid Resuscitation Fluid Resuscitation Types of Resuscitation
Large losses of fluids, electrolytes and proteins thru increased capillary permeability Maximum loss during first 6-8 hrs One half of fluid volume given in the first 8 hrs, the remainder over next 16 hrs Types of Resuscitation Parkland (Baxter)Lactated Ringers 4 ml/kg per bsa burned adults Modified Brooke Lactated Ringers 2 ml/kg per bsa burned adults, 3 ml/kg per bsa pediatrics
Lactated Ringers 4 ml/kg per bsa burned adults. Modified Brooke Lactated Ringers 2 ml/kg per bsa burned adults, 3 ml/kg per bsa pediatrics.")
134
Burn Treatment Laboratory Data Nasogastric Tube Urinary Catheter
CBC, carboxyhemoglobin levels, CMP, urine electrolytes, ABG Nasogastric Tube Prevention of aspiration/emesis Common problems with >20% BSA burns Urinary Catheter Used to monitor urine output as it relates to fluid resuscitation Urine output show be maintained at mL/kg/h adults, 1.0 mL/kg/h peds <10kg

135
Urinary Catheter Equipment Prepared Foley insertion tray
Foley catheter (rubber) 14-18 French catheter (double walled lumen) with a 5 ml balloon Urine drain bag Sterile lubricant Sterile syringe (5-10ml NS) Placement Procedure Thoroughly cleanse area Lubricate catheter and insert till urine is visualized in tube Advance another 4-5 cm past urine return for balloon placement, full in men Inflate balloon with sterile H2O and attach bag-tape tube to medial thigh for security
 French catheter (double walled lumen) with a 5 ml balloon. Urine drain bag. Sterile lubricant. Sterile syringe (5-10ml NS) Placement Procedure. Thoroughly cleanse area. Lubricate catheter and insert till urine is visualized in tube. Advance another 4-5 cm past urine return for balloon placement, full in men. Inflate balloon with sterile H2O and attach bag-tape tube to medial thigh for security.")
136
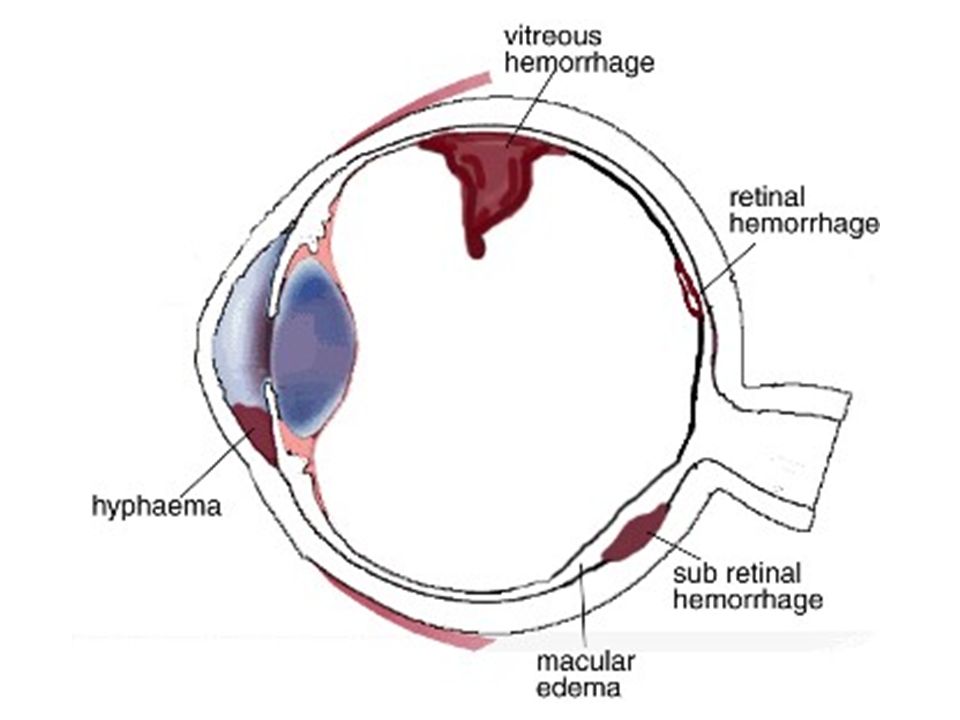
Eye Trauma!

137
Trauma Cascade In addition to obvious signs and effects of globe trauma, remember the potential for orbital and skull fractures and trauma and damage to the optic nerve.

139
Hyphema Subconjunctival Hyperemia

140
Chemical burn: Eye Injuries Irrigation and EMERGENCY referral
*****Irrigation as primary intervention Ointment type instillation prior to transport Lacrilube (OTC) / Vitamin A Oil
 / Vitamin A Oil.")
141
“Flash” burn: Common with people doing welding
Shredded raw potato poultice Vitamin A oil eye application Hydro: Direct cold X 10 min

142
Eye Injury / Abrasion Corneal Abrasion: Naturopathic treatments:
Anesthetize/gross examination with Flourescein dye. May use anesthetic. Injury is generally superficial, and dye shows shallow pooling A patch is worn for 24 hours to maintain lid closure unless injury is <1 mm. Antibiotics may be needed. Lubricant daily or at least HS during the healing phase. PO Analgesics for pain, including narcotics. *MUST rule out retention of foreign body or matter in the eye before sending patient home (in most cases irrigation and careful examination will confirm) Naturopathic treatments: Lubricant: (see above) Botanicals: 1. Calendula succus: (1:1) Apply to gauze. Use as a compress 2. Pleo-muc eye drops 3. Analgesic formula: for eye pain (internal) Piscidia erythina 2 dr (Contraindicated in pregnancy) Passiflora dr Valerian dr Bryonia gtt Gelsemium gtt QSAD: 2 oz SIG: 1 tsp., prn or up to q 2 hr. Homeopathy – See Eye – injuries 1. Aconite Hypericum Symphytum
 Naturopathic treatments: Lubricant: (see above) Botanicals: 1. Calendula succus: (1:1) Apply to gauze. Use as a compress. 2. Pleo-muc eye drops. 3. Analgesic formula: for eye pain (internal) Piscidia erythina 2 dr (Contraindicated in pregnancy) Passiflora 2 dr. Valerian 2 dr. Bryonia 5 gtt. Gelsemium 30 gtt. QSAD: 2 oz SIG: 1 tsp., prn or up to q 2 hr. Homeopathy – See Eye – injuries. 1. Aconite 2. Hypericum 3.Symphytum.")
143
2 Corneal Abrasions: 1: Non-flourescein view
Note lateral corneal edema 2: Flourescein view of another abrasion. 2

144
Eye Injury / Ulceration
Injury deeper than the outer (epithelial) corneal layer. In general needs referral for work-up Concerns include: Deep infection in the cornea Scarring / Opacity / Blindness Perforation ND Tx can follow abrasion tx guidelines Pain management is very important in ulceration, along with the above.
 corneal layer. In general needs referral for work-up. Concerns include: Deep infection in the cornea. Scarring / Opacity / Blindness. Perforation. ND Tx can follow abrasion tx guidelines. Pain management is very important in ulceration, along with the above.")
145
Corneal Ulceration Flourescein Stain Photography Mild and Severe

146
ENT Emergencies

147
Special Considerations
Common in school age population Can be life-threatening May cause great anxiety Usually non-urgent

148
Selected ENT Emergencies
Ear Laceration Hematoma Abrasions Foreign Body Burns Frostbite Nose Nasal fracture Epistaxis Foreign Body Acute Sinusitis Throat Tonsillitis Streptococus infection Peritonsillar abscess Epiglottis Retropharyngeal abscess

149
Interventions In Ear Emergencies
Lacerations/avulsions Pad between scalp and ear Assess for tetanus status Hematomas Refer for possible aspiration Abrasions Clean the area Foreign bodies Attempt to remove if near external meatus Avoid excessive manipulation Burns Wrap lightly in gauze Pad between scalp and ear Frostbite Rewarm in warm water Avoid excessive heat

150
Interventions In Nose Emergencies
Nasal fracture Check for related injuries (e.g. head injury) Ice Refer to ED Epistaxis Firm pressure for minutes Refer if bleeding continues or frequent epistaxis Foreign body Have student blow nose vigorously Remove only if easily retrievable
 Ice. Refer to ED. Epistaxis. Firm pressure for minutes. Refer if bleeding continues or frequent epistaxis. Foreign body. Have student blow nose vigorously. Remove only if easily retrievable.")
151
Interventions in Throat Emergencies
Tonsillitis/Streptococcus infection Tx as appropriate Peritonsillar abcess/cellulitis Severe pain, dysphagia Urgent - refer to ED for treatment Epiglottitis - emergent!! Monitor ABC’s and call EMS Retropharyngeal abscess - emergent!!

152
Prevention Ear protection from loud noises
Isolation of infected students Protective padding and helmets for sports Correct size and fit Educate students in proper use

153
Dental Emergencies

154
Assessment Of Dental/Oral Trauma
Use body substance isolation precautions ABC’s Types include: Soft tissue Impaled objects Injury to tooth Injury to bony structures

155
Soft Tissue Trauma Laceration/Bleeding Apply direct pressure and ice
If major bleed (over 5 minutes) – Tx or Transport Edema If swelling related to trauma - apply ice Airway compromise, difficulty talking – call EMS Impaled Object Emergent-call EMS Apply cold packs Pack gauze sponges around object to secure it
 – Tx or Transport. Edema. If swelling related to trauma - apply ice. Airway compromise, difficulty talking – call EMS. Impaled Object. Emergent-call EMS. Apply cold packs. Pack gauze sponges around object to secure it.")
156
Dental Trauma Send to dentist within the hour Fracture of a tooth
Small, cover with dental wax Large, emergent-refer to dentist Displacement of tooth Refer to dentist Avulsion of tooth Replace if possible Store appropriately for transport with student to dentist Send to dentist within the hour

157
Bony Fractures Alveolar Fracture LeForte (Maxillary) Fracture
Mandible fracture Fracture of the zygomatic arch

158
Bony Fracture Interventions
Assess ABC's Check for abnormal movement Teeth Upper or lower jaw Ice and direct pressure for bleeding Emergent - call EMS! For mandible fracture, stabilize jaw by wrapping a cravat around the protuberance of chin and top of head Transport to ED

159
Dental Pain Caries Exfoliation Eruption Orthodontic appliances

160
Soft Tissue Pain Types Most are non-urgent URGENT CONDITIONS
Bleeding gums Fistula and edema Ulcers Most are non-urgent URGENT CONDITIONS Fistula or swelling Non-draining Risk of airway compromise from cellulitis Diffuse ulcers Fever and malaise Refer for diagnosis and cause

161
Psychosocial Pain Dysmorphism Oral Habits Facial disfigurement
Craniofacial abnormalities Urgent May be subjected to peer teasing or harassment Refer to craniofacial team Oral Habits Thumb/finger sucking Non-urgent May result in malocclusion as well as social ridicule Refer to dentist

162
PREVENTION Protective devices are recommended for sport and recreational activities to decrease/prevent the risk of injuries Total head and larynx protection – football, hockey, lacrosse, baseball catchers, batters Full face protection – fencing, hockey goalies Eye protectors – all racquet sports, soccer, basketball, softball

163
SUMMARY Pain or injury involving the eyes, ears, nose, throat or oral structures often evokes tremendous anxiety in students. Always maintain a reassuring demeanor as you perform your assessment and management. Develop and conduct injury prevention programs and implement safety measures to prevent EENT emergencies.

Similar presentations









 RESUSCITATION Chapter 4 Ver 5.1 May 2013.>")





 cardiopulmonary.>")






