Download presentation
Presentation is loading. Please wait.

1
Human Anatomy & Physiology University of Washington PMT
Endocrine System Human Anatomy & Physiology University of Washington PMT

2
The Endocrine System

3
Endocrine System The Endocrine System Regulates long-term processes
Growth Development Reproduction Uses chemical messengers to relay information and instructions between cells Direct communication Paracrine communication Endocrine communication Direct Communication Exchange of ions and molecules between adjacent cells across gap junctions Occurs between two cells of same type Highly specialized and relatively rare Paracrine Communication Uses chemical signals to transfer information from cell to cell within single tissue Most common form of intercellular communication Endocrine Communication Endocrine cells release chemicals (hormones) into bloodstream Alters metabolic activities of many tissues and organs simultaneously
 into bloodstream. Alters metabolic activities of many tissues and organs simultaneously.")
4
Hormonal Action Target Cells Hormones
Are specific cells that possess receptors needed to bind and “read” hormonal messages Hormones Stimulate synthesis of enzymes or structural proteins Increase or decrease rate of synthesis Turn existing enzyme or membrane channel “on” or “off”

5
Hormone Actions “Lock and Key” approach: describes the interaction between the hormone and its specific receptor. Receptors for nonsteroid hormones are located on the cell membrane Receptors for steroid hormones are found in the cell’s cytoplasm or in its nucleus Free Hormones Remain functional for less than 1 hour Diffuse out of bloodstream: bind to receptors on target cells Are broken down and absorbed: by cells of liver or kidney Are broken down by enzymes: in plasma or interstitial fluids

6
Non Lipid Soluble Hormonal Action
Hormones and Plasma Membrane Receptors Bind to receptors in plasma membrane Cannot have direct effect on activities inside target cell Use intracellular intermediary to exert effects First messenger: leads to second messenger may act as enzyme activator, inhibitor, or cofactor results in change in rates of metabolic reactions Hormones and Plasma Membrane Receptors Catecholamines (E, NE & D) and peptide hormones (ADH, ACTH, oxytocin) Are not lipid soluble Unable to penetrate plasma membrane Bind to receptor proteins at outer surface of plasma membrane (extracellular receptors)
 and peptide hormones (ADH, ACTH, oxytocin) Are not lipid soluble. Unable to penetrate plasma membrane. Bind to receptor proteins at outer surface of plasma membrane (extracellular receptors)")
7
Hormones and Plasma Membrane Receptors
Important Second Messengers Cyclic-AMP (cAMP) Derivative of ATP Cyclic-GMP (cGMP) Derivative of GTP Calcium ionsThe Process of Amplification Is the binding of a small number of hormone molecules to membrane receptors Leads to thousands of second messengers in cell Magnifies effect of hormone on target cellDown-regulation Presence of a hormone triggers decrease in number of hormone receptors When levels of particular hormone are high, cells become less sensitive Up-regulation Absence of a hormone triggers increase in number of hormone receptors When levels of particular hormone are low, cells become more sensitive Hormones and Plasma Membrane Receptors G Protein Enzyme complex coupled to membrane receptor Involved in link between first messenger and second messenger Binds GTP Activated when hormone binds to receptor at membrane surface and changes concentration of second messenger cyclic-AMP (cAMP) within cell: increased cAMP level accelerates metabolic activity within cell
 Derivative of ATP. Cyclic-GMP (cGMP) Derivative of GTP. Calcium ionsThe Process of Amplification. Is the binding of a small number of hormone molecules to membrane receptors. Leads to thousands of second messengers in cell. Magnifies effect of hormone on target cellDown-regulation. Presence of a hormone triggers decrease in number of hormone receptors. When levels of particular hormone are high, cells become less sensitive. Up-regulation. Absence of a hormone triggers increase in number of hormone receptors. When levels of particular hormone are low, cells become more sensitive. Hormones and Plasma Membrane Receptors. G Protein. Enzyme complex coupled to membrane receptor. Involved in link between first messenger and second messenger. Binds GTP. Activated when hormone binds to receptor at membrane surface and changes concentration of second messenger cyclic-AMP (cAMP) within cell: increased cAMP level accelerates metabolic activity within cell.")
8
Lipid Soluble Hormonal Action
Steroid Hormones: Lipid soluble Diffuse through cell membranes Endocrine organs Adrenal cortex Ovaries Testes Thyroid Examples are testosterone, thyroxine (T3), triiodothyronine (T4), Calciitonin
, triiodothyronine (T4), Calciitonin.")
9
Hormones and Intracellular Receptors
Alter rate of DNA transcription in nucleus Change patterns of protein synthesis Directly affect metabolic activity and structure of target cell Includes steroids and thyroid hormones

10
Pituitary Gland A marble-sized gland at the base of the brain
Controlled by the hypothalamus or other neural mechanisms and therefore the middle man.

11
Pituitary Gland

12
The Pituitary Gland and its Hormones
Posterior Lobe Antidiuretic hormone (ADH) Oxytocin Anterior Lobe Adrenocorticotropic (ACTH) Growth hormone (GH) Thyroid-stimulating hormone (TSH) Follicle-stimulating hormone (FSH) Luteinizing hormone (LH) Prolactin (PRL) GH Deficiency: Pituitary Growth Failure / Dwarfism – Retarded growth, abnormal fat distribution, low blood glucose hours after meals GH Overproduction: Gigantism / Acromegaly – Excessive growth ADH Deficiency: Diabetes Insipidus – Polyuria, dehydration, thirst (Central DI vs. Nephrogenic DI) ADH Overproduction: SIADH (Syndrome of Inappropriate Antidiuretic Hormone Secretion) – Increased water content / body mass
 Oxytocin. Anterior Lobe. Adrenocorticotropic (ACTH) Growth hormone (GH) Thyroid-stimulating hormone (TSH) Follicle-stimulating hormone (FSH) Luteinizing hormone (LH) Prolactin (PRL) GH Deficiency: Pituitary Growth Failure / Dwarfism – Retarded growth, abnormal fat distribution, low blood glucose hours after meals. GH Overproduction: Gigantism / Acromegaly – Excessive growth. ADH Deficiency: Diabetes Insipidus – Polyuria, dehydration, thirst (Central DI vs. Nephrogenic DI) ADH Overproduction: SIADH (Syndrome of Inappropriate Antidiuretic Hormone Secretion) – Increased water content / body mass.")
13
Endocrine Reflexes Neuroendocrine Reflexes Complex Commands
Functional counterparts of neural reflexes In most cases, controlled by negative feedback mechanisms Stimulus triggers production of hormone whose effects reduce intensity of the stimulus Endocrine reflexes can be triggered by Humoral stimuli Changes in composition of extracellular fluid Hormonal stimuli Arrival or removal of specific hormone Neural stimuli Arrival of neurotransmitters at neuroglandular junctions Simple Endocrine Reflex Involves only one hormone Controls hormone secretion by the heart, pancreas, parathyroid gland, and digestive tract Complex Endocrine Reflex Involves One or more intermediary steps Two or more hormones The hypothalamus Neuroendocrine Reflexes Pathways include both neural and endocrine components Complex Commands Issued by changing Amount of hormone secreted Pattern of hormone release: hypothalamic and pituitary hormones released in sudden bursts frequency changes response of target cellsTwo Classes of Hypothalamic Regulatory Hormones Releasing hormones (RH) Stimulate synthesis and secretion of one or more hormones at anterior lobe Inhibiting hormones (IH) Prevent synthesis and secretion of hormones from the anterior lobe Rate of secretion is controlled by negative feedback Negative feedback is the primary mechanism through which your endocrine system maintains homeostasis Secretion of a specific hormone s turned on or off by specific physiological changes (similar to a thermostat) EXAMPLE: plasma glucose levels and insulin response
 Stimulate synthesis and secretion of one or more hormones at anterior lobe. Inhibiting hormones (IH) Prevent synthesis and secretion of hormones from the anterior lobe. Rate of secretion is controlled by negative feedback. Negative feedback is the primary mechanism through which your endocrine system maintains homeostasis. Secretion of a specific hormone s turned on or off by specific physiological changes (similar to a thermostat) EXAMPLE: plasma glucose levels and insulin response.")
14
Hypothalamus Two Classes of Hypothalamic Regulatory Hormones
Releasing hormones (RH) Stimulate synthesis and secretion of one or more hormones at anterior lobe Inhibiting hormones (IH) Prevent synthesis and secretion of hormones from the anterior lobe Rate of secretion is controlled by negative feedback
 Stimulate synthesis and secretion of one or more hormones at anterior lobe. Inhibiting hormones (IH) Prevent synthesis and secretion of hormones from the anterior lobe. Rate of secretion is controlled by negative feedback.")
15
Pituitary Gland

16
Thyroid Gland Thyroid Gland Located along the midline of the neck
Secretes two nonsteroid hormones Triiodothyronine (T3) Thyroxine (T4) Calcitonin: calcium metabolism (osteoblast) Regulates metabolism increases protein synthesis promotes glycolysis, gluconeogenesis, glucose uptake
 Thyroxine (T4) Calcitonin: calcium metabolism (osteoblast) Regulates metabolism. increases protein synthesis. promotes glycolysis, gluconeogenesis, glucose uptake.")
17
Thyroid Gland

18
Thyroid Gland Thyroid Hormones Enter target cells by transport system
Thyroid-Stimulating Hormone (TSH) Absence causes thyroid follicles to become inactive Neither synthesis nor secretion occurs Binds to membrane receptors Activates key enzymes in thyroid hormone production Thyroid Hormones Enter target cells by transport system Affect most cells in body Bind to receptors in Cytoplasm Surfaces of mitochondria Nucleus In children, essential to normal development of Skeletal, muscular, and nervous systems Calorigenic Effect Cell consumes more energy resulting in increased heat generation Is responsible for strong, immediate, and short-lived increase in rate of cellular metabolism T3/T4 Deficiency: Myxedema / Cretinism – Low metabolic rate / low body temperature / impaired physical & mental development T3/T4 Overproduction: Hyperthyroidism / Graves Disease – High metabolic rate / temperature
 Absence causes thyroid follicles to become inactive. Neither synthesis nor secretion occurs. Binds to membrane receptors. Activates key enzymes in thyroid hormone production. Thyroid Hormones. Enter target cells by transport system. Affect most cells in body. Bind to receptors in. Cytoplasm. Surfaces of mitochondria. Nucleus. In children, essential to normal development of. Skeletal, muscular, and nervous systems. Calorigenic Effect. Cell consumes more energy resulting in increased heat generation. Is responsible for strong, immediate, and short-lived increase in rate of cellular metabolism. T3/T4 Deficiency: Myxedema / Cretinism – Low metabolic rate / low body temperature / impaired physical & mental development. T3/T4 Overproduction: Hyperthyroidism / Graves Disease – High metabolic rate / temperature.")
19
Parathyroid Glands Embedded in posterior surface of the thyroid gland
Parathyroid hormone (PTH) Produced by chief cells In response to low concentrations of Ca2+
 Produced by chief cells. In response to low concentrations of Ca2+")
20
Parathyroid Gland Four Effects of PTH It stimulates osteoclasts
Accelerates mineral turnover and releases Ca2+ from bone It inhibits osteoblasts Reduces rate of calcium deposition in bone It enhances reabsorption of Ca2+ at kidneys, reducing urinary loss It stimulates formation and secretion of calcitriol at kidneys Effects complement or enhance PTH Enhances Ca2+, PO43- absorption by digestive tract PTH Deficiency: Hypoparathyroidism – Muscular weakness, neurological problems, formation of dense bones, tetany due to low blood Ca PTH Overproduction: Hyperparathyroidism – Neurological, mental, muscular problems due to high blood Ca, weak brittle / bones

21
Suprarenal (Adrenal) Gland
Lie along superior border of each kidney Subdivided into: Superficial suprarenal cortex Stores lipids, especially cholesterol and fatty acids Inner suprarenal medulla Secretory activities controlled by sympathetic division of ANS

22
Suprarenal (Adrenal) Gland
Adrenal Medulla Contains two types of secretory cells Epinephrine (70-75% of mass) Increase H.R. and B.P. Increase respiration Increase metabolic rate Increase glycogenolysis Bronchodilation Norepinephrine (20-25% of mass) Vasoconstriction Interesting that both hormones when released by Adrenal gland, but neurotransmitters when released at synapses Catacholeamine Deficiency: None known Catacholeamine Overproduction: Pheochromocytoma – High metabolic rate, elevated temperature, high HR and blood glucose levels
 Increase H.R. and B.P. Increase respiration. Increase metabolic rate. Increase glycogenolysis. Bronchodilation. Norepinephrine (20-25% of mass) Vasoconstriction. Interesting that both hormones when released by Adrenal gland, but neurotransmitters when released at synapses. Catacholeamine Deficiency: None known. Catacholeamine Overproduction: Pheochromocytoma – High metabolic rate, elevated temperature, high HR and blood glucose levels.")
23
Suprarenal (Adrenal) Gland
Adrenal Cortex Mineralocorticoids (Zona Glomerulosa) Aldosterone: maintains electrolyte balance Na+ reabsorption by kidneys & K+ urinary loss Glucocorticoids (Zona Fasciculate) Cortisol (Hydrocortisone): Stimulates gluconeogenisis Mobilization of free fatty acids Anti-inflammatory agent Androgens (Zona Recticularis) Bone growth, muscle growth & blood formation Aldosterone Deficiency: Hypoaldosteronism – Polyuria, low blood volume, high serum K, low serum Na Aldosterone Overproduction: Aldosteronism – Increased body weight due to Na & water retention, low serum K Glucocorticoids Deficiency: Addison’s Disease – Inability to tolerate stress, mobilize energy reserves or maintain normal blood glucose levels Glucocorticoids Overproduction: Cushing Disease – Excessive break down of tissue proteins and lipid reserves, impaired glucose metabolism
 Aldosterone: maintains electrolyte balance. Na+ reabsorption by kidneys & K+ urinary loss. Glucocorticoids (Zona Fasciculate) Cortisol (Hydrocortisone): Stimulates gluconeogenisis. Mobilization of free fatty acids. Anti-inflammatory agent. Androgens (Zona Recticularis) Bone growth, muscle growth & blood formation. Aldosterone Deficiency: Hypoaldosteronism – Polyuria, low blood volume, high serum K, low serum Na. Aldosterone Overproduction: Aldosteronism – Increased body weight due to Na & water retention, low serum K. Glucocorticoids Deficiency: Addison’s Disease – Inability to tolerate stress, mobilize energy reserves or maintain normal blood glucose levels. Glucocorticoids Overproduction: Cushing Disease – Excessive break down of tissue proteins and lipid reserves, impaired glucose metabolism.")
24
Pineal Gland Lies in posterior portion of roof of third ventricle
Contains pinealocytes Synthesize hormone melatonin Inhibits reproductive functions Protects against damage from free radicals Setting circadian rhythms

25
Pancreas Exocrine / Endocrine Gland
Endocrine Pancreas consists of “clusters” of cells called Islets of Langerhans 4 types of cells of endocrine pancreas Comprise only 1% of entire pancreas

26
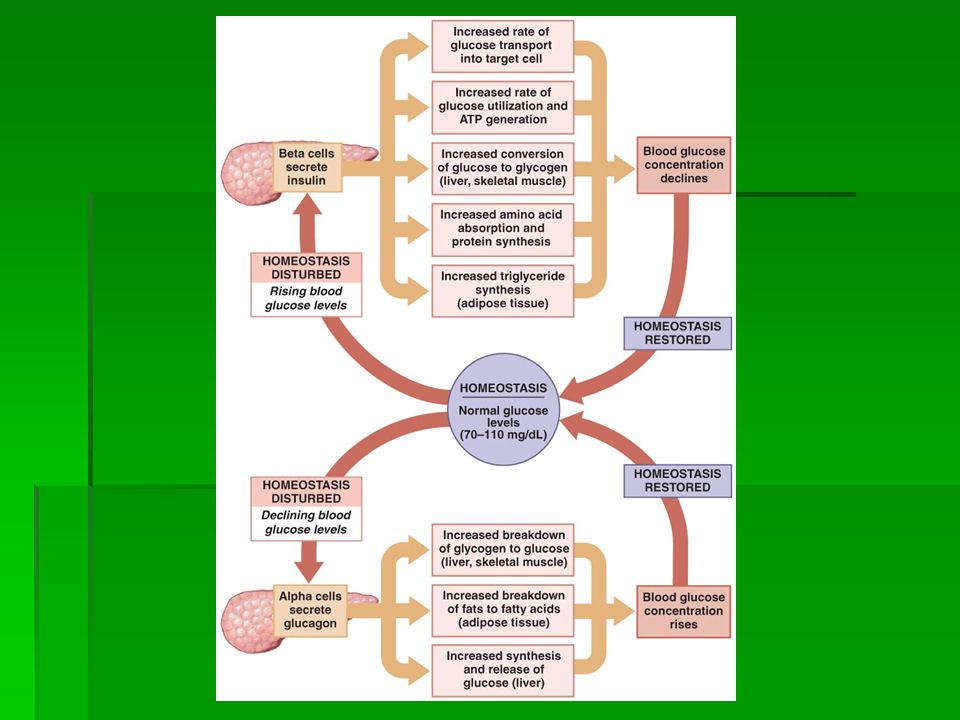
Pancreas Insulin Affects target cells by:
A peptide hormone released by beta cells Affects target cells by: Accelerate glucose uptake Accelerate glucose utilization and enhances ATP formation Stimulate glycogen formation Stimulate amino acid absorption and protein synthesis Stimulate triglyceride formation in adipose tissue Insulin Deficiency: Diabetes Mellitus – High blood sugars, impaired glucose utilization, dependance on lipids of energy, glycosuria Insulin Overproduction: (Iatrogenic / Tumor) – Low blood sugars
 – Low blood sugars.")
27
Pancreas Glucagon Affects target cells: Released by alpha cells
Mobilizes energy reserves Affects target cells: Stimulates breakdown of glycogen in skeletal muscle and liver tissue Stimulates breakdown of triglycerides in adipose tissue Stimulates production of glucose in liver

29
Sex Organs (Testes & Ovaries)
Testes (Gonads) Produce androgens in interstitial cells Testosterone is the most important male hormone Secrete inhibin in nurse (sustentacular) cells Support differentiation and physical maturation of sperm Ovaries (Gonads) Produce estrogens Principle estrogen is estradiol After ovulation, follicle cells Reorganize into corpus luteum Release estrogens and progestins, especially progesterone Female: Estrogens Deficiency: Hypogonadism– Sterility, lack of secondary sex characteristics Estrogen Overproduction: Adrenogenital Syndrome – Masculinization Precocious puberty – Premature sexual maturation, related behavioral changes Male: Androgen Deficiency: Hypogonadism– Sterility, lack of secondary sex characteristics Androgen Overproduction: Adrenogenital Syndrome – Breast enlargement
 Produce androgens in interstitial cells. Testosterone is the most important male hormone. Secrete inhibin in nurse (sustentacular) cells. Support differentiation and physical maturation of sperm. Ovaries (Gonads) Produce estrogens. Principle estrogen is estradiol. After ovulation, follicle cells. Reorganize into corpus luteum. Release estrogens and progestins, especially progesterone. Female: Estrogens Deficiency: Hypogonadism– Sterility, lack of secondary sex characteristics. Estrogen Overproduction: Adrenogenital Syndrome – Masculinization. Precocious puberty – Premature sexual maturation, related behavioral changes. Male: Androgen Deficiency: Hypogonadism– Sterility, lack of secondary sex characteristics. Androgen Overproduction: Adrenogenital Syndrome – Breast enlargement.")
30
Thymus Produces thymosins (blend of thymic hormones)
That help develop and maintain normal immune defenses

31
Endocrine Tissues of Other Organs
Kidneys: Produce calcitriol and erythropoietin Produces enzyme renin Heart: Produces natriuretic peptides (ANP & BNP) When blood volume becomes excessive Action opposes angiotensin II Resulting in reduction of blood pressure & volume Kidneys sense lower GFR and lower blood oxygen saturations, release EPO
 When blood volume becomes excessive. Action opposes angiotensin II. Resulting in reduction of blood pressure & volume. Kidneys sense lower GFR and lower blood oxygen saturations, release EPO.")
33
Hormone Interactions General Adaptation Syndrome (GAS)
Also called stress response How body responds to stress-causing factors Is divided into three phases: Alarm phase Resistance phase Exhaustion phase

34
Fight or Flight Epinephrine is dominant hormone

35
Stresses that persist for hours / days / weeks – starvation, acute illness, etc
Mobilization of remaining Lipid & Protein Reserves Conservation of Glucose for Neural Tissues Elevation & Stabilization of Blood Glucose concentration Conservation of Salts & Water and the Loss of K+ and H+

Similar presentations





 that are released into the blood Hormones control several major processes Reproduction - gametogenesis,>")

>")












