Download presentation
Presentation is loading. Please wait.

1
Dr. Sue Shapiro Associate Professor Barry University
Lumbar Spine Dr. Sue Shapiro Associate Professor Barry University

2
Lumbar Spine Bony Anatomy
5 lumbar vertebrae Massive vertebrae bodies with the width greater than the anterior-posterior diameter L4 &5 slightly wedge-shaped & anterior convexity (anterior pelvic tilt) these features stabilize and accommodate the increasing body weight supported at the end of spinal column
 these features stabilize and accommodate the increasing body weight supported at the end of spinal column.")
3
Facet Joints of Lumbar Spine
Articular process have a distinct concave-convex arrangement: inferior facet sits medial to the superior while superior facet faces medial and posterior and is concave the inferior is convex and faces anterior and laterally- this limits rotation f the lumbar and facilitates flexion, extension and side bending

4
Lumbar Spine Facets

5
Lumbar Superior Facets
Superior facet serve as attachment for Multifidus Multifidus muscle has the same mechanical function as the semispinalis capitis muscle of cervical spine; they are primary extensors of the lumbar and cervical spine

6
Spinous Process Orientation in Lumbar Spine
Lumbar spine spinous process have horizontal and extended posterior orientation making it possible to insert a needle b/t the adjacent vertebrae at L3 & L4 for CSF – know as the lumbar puncture

7
Sacral Spine Wedged structure made up of 5 fused vertebrae
Superior it articulates with the L5 vertebrae Inferior with coccyx and Laterally with the ilium This articulation is considered to be the keystone of pelvic arch

8
Sacral Spine Anterior /Posterior View
There is a separate anterior and posterior foramina where the sacral nerves exit. The anterior divisions exit from anterior sacral foramen and give rise to the sciatic nerve

9
L5 S1 Junction Intervertebral disc located b/t L5 & sacrum is very thick especially in anterior border This is where the lumbarsacral angle is formed The most notoriously frequent site for pain in the low back An increase in lumbar lordosis or increase pelvic tilt of the pelvis results in an increased lumbosacral angle. Whereas a decreased in lumbosacral angle is due to posterior tilt of pelvis

10
Lumbar Sacralization 5th lumbar vertebra may be fused at the lumbosacral joint The transverse processed forms a pseudoarthrosis at its point of contact with the sacral wing The L3,4 nerve roots may become irritated on left lateral flexion due to mechanical irritation

11
Lumbar Sacralization

12
Spondylolisthesis Due to anterior shearing of L5 on the sacrum there is a tendency toward anterior displacement of lumbar facets Spondylolisthesis refers to anterior displacement of one vertebra upon the subjacent vertebra and is seen at the lumbosacral articulation.

13
Common Causes of Spondylolisthesis
1. Most common cause is a defect in the bony region between the superior and inferior articular processes of the vertebrae (pars interarticularis) 2. a fracture – stress fractures 3. an elongated pedicle
 2. a fracture – stress fractures. 3. an elongated pedicle.")
14
Scotty Dog Deformity Classification of Spondylopathies
Spondylitis- Inflammation of the vertebrae Spondylosis- Arthritis or osteoarthritis of the vertebrae resulting in pressure being placed o the vertebral nerve root Spondylolisthesis- Forward slippage of a vertebra o the one below it ( may occur secondary to spondylolysis in which the fx of pars interarticularis results Spondylolysis- Degeneratio of a vertebra structure secondary to repetitive stress, most commonly affecting the pars interarticularis but with no displacement of the vertebral body.

15
Spondylolisthesis

16
Sacroiliac Joint Fusion of first 3 sacra vertebrae and ilium
Movement of sacrum on the ilium is referred to as Nutation ( flexion) or countranutation (extension) Movement of ilium on the sacrum is referred to as torsion – Anterior torsion occurs when the ASIS moves forward and down ; posterior torsion occurs when the ASIS moves upward and back
 or countranutation (extension) Movement of ilium on the sacrum is referred to as torsion – Anterior torsion occurs when the ASIS moves forward and down ; posterior torsion occurs when the ASIS moves upward and back.")
17
Lumbosacral Trunk LST is in close approximation to the LSJ and can cause compression injuries that may cause muscle spasms. Since L4 & L5 are the principal constituents of the sciatic nerve (L4-S3) any irritation can cause Sciatica
 any irritation can cause Sciatica.")
18
Spinal Nerves and Plexus
There are 31 pairs of spinal nerves They form networks of nerves or plexus -5 plexuses Cervical Plexus- C1-C4 Brachial Plexus-C5- T1 Lumbar plexus L1-L4 Sacral plexus L4- S4 Coccygeal plexus S4-S5

19
Coccyx Composed of 3-5 fused vertebral bodies that have no vertebral arch 1st coccygeal vertebra is the largest and articulates with the sacrum at the sacrococcygeal junction Serves as a bony origin for muscles of the pelvic diaphragm Falls on to the coccyx can be very painful and necessitate coccyx excision for pain relief

20
Ligaments of the Lumbar Spine
Anterior Longitudinal Lig- It’s narrow in the Cs region, increases in width in the lumbar spinal column. Prevents anterior disc protrusion Posterior Longitudinal LIg.- it’s widest in C spine but narrows in the thoracic and lumbar spine- only ½ as wide in lumbar spine as in C spine which is a problem for posterior stability of disc and shifting in L spine

21
Ligaments of the Lumbar Spine
Ligamentum flavum – bridges the space b/t adjacent laminae and is highly elastic preventing the chance that lig. Will buckle into the spinal canal Interspinous Lig. Broad and thick, resist separation of the spinous processes therefore limiting flexion of the lumbar segments Supraspinous ligament- most outward lig. That terminates at L4 in 22% of individuals and completely lacking at L5-S1. It limits forward bending of the lumbar spine

22
Iliolumbar Ligaments

23
Sacroliliac Ligaments

24
LUMBAR DISC Lumbar disc are significantly thicker and have a greater cross section Provide 1/3 of the length in the lumbar spine compared to 1/5 in cervical and thoracic spine

25
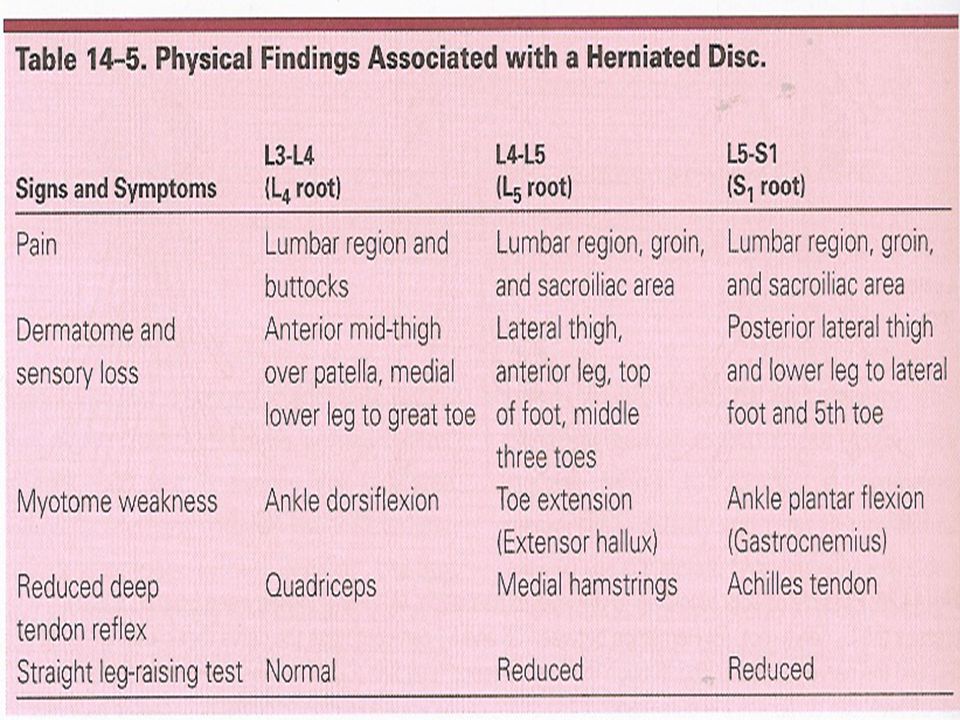
Herniated Disc Classifications
Protruded- some eccentric accumulation of the nucleus with slight deformity of annulus Prolapsed- definite deformity as it works its way through the fiber of annulus Extruded - nuclear material comes into the spinal canal and runs the risk of impinging adjacent nerve roots Sequestrated- nuclear material has separated from the disc itself and potentially migrates

26
Degenerated Disc Disc herniation can be acute or stress related
Most show signs of previous degeneration Most common lumbar disc herniation are between L4-L5 and L5-S1 Next most common herniations are lower two cervical discs

27
Disc Impingement Symptoms
Intervertebral discs are not innervated thus do not cause pain , it is sensory nerves supplying the ligaments, bony structures, spinal cord or spinal nerves that produce both sensory and motor symptoms Depending on where herniation takes place the myotome and dermatome patterns associated with the nerve root will cause symptoms

29
Spinal Sternosis Defined as a loss of cerebrospinal fluid around the spinal cord due to deformation of the spinal cord, or a narrowing of the neural canal Common symptom is bilateral leg weakness and numbness with or without sciatica: neg SLR; + pain on prolonged spine extension exacerbated with ipsilateral trunk lateral flexion

30
Combination of Disc Degeneration and Spinal Sternosis or Spondylosis

31
Orthopedic Test for Disc Pathology
Well Leg Raise Test Milgram Test Valsalva’s Test Naffzinger Test

32
Sciatica Defined as compression and/or inflammation of a spinal nerve making up the sciatic nerve due to a herniated disc, annular tear, myogenic or muscle-related disease, spinal sternosis, facet joint arthropathy, or compression from the piriformis muscle Typically, if related to herniated disc, radiating leg pain is greater than back pain and increases with sitting and leaning forward , coughing, sneezing and straining Pain is produced during ipsilateral SLR With annular tears, back pain is more prevalent and exacerbated with SLR Different from spinal sternosis because back pain starts usually after walking a limited distance and concomitantly increases as distance increases . Pain is not reproduced with SLR but can be reproduced with prolonged spine extension, which is relieved with spine flexion

34
Orthopedic Test to Evaluate Sciatica
Straight Leg Raise “Lasegue Test” Kernig/Brudzinski Test Bowstring Test (Cram Test) Slump Test
 Slump Test.")
35
Low Back Pain (LBP) 60 to 80% of the population experiences LBP at some time in their lives Males and females appear to be equally susceptible LBP is second only to the common cold as the leading cause of lost work time Back injuries dominate claims for worker’s compensation LBP accounts for 10% of all chronic health problems and is ranked 11th among causes for hospitalization in the US Most cases are idiopathic or unknown origin Mechanical stress is the primary causal mechanism Most common among runners , soccer, field hockey , lacrosse, rowers Mechanism of injury is tight hip flexors, hamstring which produce a forward body lean leading to anterior pelvic tilt and hyperlordosis of the lumbar spine

36
Lumbar Contusion, Strains, and Sprains
Soft tissue injuries are the most common injuries in the lumbar spine MOI – Lumbar muscles develop tension to counteract the forward bending moment of the entire trunk when the trunk is in flexion, they are susceptible to strain Symptoms: Localized pain, increasing with active and resistive motion, radiating pain and neurological deficits

37
Abdominal Muscle Strains

38
Hip Flexor Muscles

39
Erector Spinae and Multifidus Muscles

Similar presentations