Download presentation
Presentation is loading. Please wait.

2
Sport Injuries Hand and Wrist

3
HAND AND WRIST HAND WRIST

4
HAND FUNCTIONS 45% GRASP 45% PINCH 5% HOOK 5% PAPERWEIGHT
Side pinch (key pinch) Tip pinch (writing) Chuck pinch (thumb to index/ring) 5% HOOK Carry bag 5% PAPERWEIGHT
 Tip pinch (writing) Chuck pinch (thumb to index/ring) 5% HOOK. Carry bag. 5% PAPERWEIGHT.")
5
HAND & FINGER ANATOMY 9 Finger Flexors Median nerve
Transverse carpal ligament 5 deep flexors pass through superficialis tendons and insert on distal phalanx of each finger and thumb 4 superficial flexors insert on middle phalanx of digits 2-5 Annular ligaments = pulleys (A1-A5) PREVENT BOWSTRINGING
 PREVENT BOWSTRINGING.")
7
HAND ANATOMY VOLAR PLATE COLLATERAL LIGAMENTS
Thickened portion of joint capsule Static stabilizer (hyperextension) COLLATERAL LIGAMENTS Medial and lateral stability Maximally tight at ____ degrees MCP flexion ____ degrees PIP flexion ____ degrees DIP flexion Collaterals will be maximally lengthened at this tightness so beneficial for immobilizing 70 30 15
 COLLATERAL LIGAMENTS. Medial and lateral stability. Maximally tight at. ____ degrees MCP flexion. ____ degrees PIP flexion. ____ degrees DIP flexion. Collaterals will be maximally lengthened at this tightness so beneficial for immobilizing")
8
HAND ANATOMY digits FLEXOR Extensor FDP FDS Volar plate Central bands
Lateral bands

9
Finger Anatomy Figure 1. Anatomy of the finger. (A) Joints and ligaments. (B) Tendons.
 Joints and ligaments. (B) Tendons.")
10
NERVES OF THE HAND RADIAL MEDIAN ULNAR WRIST AND FINGER EXTENSION
THENAR COMPARTMENT, OPPOSITION, PINCER GRIP INTRINSIC MUSCLES POWER GRIP

11
How I Will Approach Each Problem
What is it? Does it need any special imaging? How do I treat it? What are the indications for surgery? I will give a case for many of them Referral different for each person- non-dominant pinky vs. dominant, concert pianist

12
Finger Injury Pearls Treatment should restrict motion of the injured structures while allowing uninjured joints to remain mobile Patients should be counseled that it is not unusual for an injured digit to remain swollen for some time and that permanent deformity is possible even after treatment

13
MALLET FINGER

14
MALLET FINGER ANATOMY MECHANISM: TREATMENT: COMPLICATIONS:
Dorsal avulsion Extensor digitorum tendon tear MECHANISM: Forced flexion of extended digit TREATMENT: No fracture: DIP extended for 6-8 weeks FRACTURE: if <30% joint surface, splint x 4 weeks If >30% Might need ORIF Less than full passive extension????? COMPLICATIONS: Pressure necrosis from splint Permanent extensor lag

15
Mallet Finger Presentation
Pain at dorsal DIP joint Inability to actively extend the joint Characteristic flexion deformity On exam, very important to isolate the DIP joint to ensure extension from DIP and not the central slip If can’t passively extend consider bony entrapment All of these need x-rays Figure 2. Injury to the joint extensor tendon at the distal interphalangeal joint (mallet finger)
")
16
Flexor Digitorum Profundus Tendon Injury (jersey finger)
Athlete’s finger catches another player’s clothing Forced extension of the DIP joint during active flexion 75% occur in the ring finger Force can be concentrated at the middle or distal phalanx -Flexor digitorum profundus tendon inserts into the base of the distal phalanx- volar base -Relatively uncommon, but devastating is missed The true definition is a bony injury If not fixed by 2 weeks the blood supply is so limited that it needs to necrosis of the finger

17
JERSEY FINGER ANATOMY: MECHANISM: TREATMENT: Tendon retracts
Avulsion fragment may limit retraction Blood supply compromised MECHANISM: Forced extension of flexed finger TREATMENT: Refer immediately COMPLICATIONS: Permanent loss of flexion

18
JERSEY FINGER EXAM FINDINGS: Unable to flex isolated DIP
Localized tenderness along flexor tendon FDP: hold PIP straight and flex DIP FDS: hold MCP straight and flex PIP or hold all fingers in extension except affected and flex

19
Jersey Finger Treatment/ Referral
All need to be referred for surgery immediately Tendon retracts Avulsion fragment may limit retraction Blood supply compromised Permanent loss of flexion

20
CENTRAL SLIP AVULSION ANATOMY MECHANISM:
Extensor digitorum communis tendon disruption Lateral bands migrate in volar direction MECHANISM: Volar-directed force on middle phalanx against semi-flexed finger attempting to extend

21
CENTRAL SLIP AVULSION EXAM: TREATMENT COMPLICATIONS:
Pain, swelling over dorsal PIP PIP in degrees flexion May have limited extension (better at 0 degrees than 30 degrees) TREATMENT Surgery if >30% joint surface involved with avulsion fx PIP splint in full extension 4-5 weeks Protect 6-8 weeks for sports *allow DIP to flex- relocates lateral bands COMPLICATIONS: Boutonierre deformity
 TREATMENT. Surgery if >30% joint surface involved with avulsion fx. PIP splint in full extension 4-5 weeks. Protect 6-8 weeks for sports. *allow DIP to flex- relocates lateral bands. COMPLICATIONS: Boutonierre deformity.")
22
Central Slip Extensor Tendon Injury- Boutonnière deformity
PIP joint is forcibly flexed while actively extended Volar dislocation of the PIP joint Examine with PIP joint in degrees of flexion, can’t active extend but can passively extend Tenderness over dorsal aspect of the middle phalanx Commonly occurs in basketball Figure 6. Boutonniére deformity caused by a central slip extensor tendon injury. (A) Normal alignment. (B) Boutonniére deformity.
 Normal alignment. (B) Boutonniére deformity.")
23
Central Slip Extensor Tendon Injury Treatment
A delay in proper treatment will cause boutonniere deformity Deformity can develop over several weeks or occasionally acutely Splint PIP in extension for 6 weeks Can still play sports Boutonnier- flexion of PIP coupled with extension of MCP and DIP Takes several weeks- lateral bands slip inferiorly

24
Central Slip Extensor Tendon Injury ,Surgery
Avulsion fracture involving more than 30 percent of the joint Inability to achieve full passive extension

25
Volar Plate Injury Hyperextension, such as dorsal dislocation
PIP is usually affected Collateral damage is often present The loss of joint stability can cause hyperextension deformity

26
VOLAR PLATE RUPTURE EXAM FINDINGS: MECHANISM: Tender volar PIP
Bruising, swelling MECHANISM: Hyperextension injury Ruptures distally from attachment at middle phalanx

27
VOLAR PLATE RUPTURE TREATMENT: COMPLICATIONS: Early mobilization
Extension block splint Buddy tape Surgery if >30% joint involved COMPLICATIONS: Swan neck deformity: extensor tendons pull PIP into hyperextension, DIP flexion Swan Neck Deformity

28
Volar Plate Injury- Treatment
Progressive splinting starting at 30 degrees flexion Followed by buddy taping If less severe, can buddy tape immediately Can play sports if splinted

30
Collateral Ligament Injuries
Forced ulnar or radial deviation Can cause partial or complete tear PIP is usually involved Present with pain at the affected ligament Evaluate with involved joint at 30 degrees of flexion and MCP at 90 degrees of flexion

31
Collateral Ligament Injuries- Treatment
If joint stable and no large fracture- can buddy tape Never leave the pinky alone ?Physical Therapy- if joint stiff Figure 7. Buddy taping for the treatment of finger injuries. (A) Self-adhesive wrap. (B) Velcro wrap.
 Self-adhesive wrap. (B) Velcro wrap.")
32
Finger Case Ultimate frisbee player tried dove to block an opponents disc and he jammed his thumb on the ground. He was able to keep playing but it swelled and became ecchymotic.

33
GAMEKEEPER’S THUMB Hyperabduction of thumb EXAM: Weak, painful pinch
MECHANISM Hyperabduction of thumb EXAM: Weak, painful pinch Pain over ulnar thumb XRAYS BEFORE STRESS Type I: avulsion, no displacement; Type II: avulsion, displaced; Type III: torn ligament, stable in flexion; Type IV: torn ligament, unstable flexion

34
GAMEKEEPER’S THUMB SIGNS Pain over ulnar thumb Stress testing positive
Testing in Extension and 40 degrees of FLEXION of MCP With extension or slight flexion the normally taut volar plate gives MCP stability Type I: avulsion, no displacement; Type II: avulsion, displaced; Type III: torn ligament, stable in flexion; Type IV: torn ligament, unstable flexion

35
Ulnar Collateral Ligament Injury of the Thumb (Skier’s Thumb)
Caused by forced abduction of the 1st MCP joint Left untreated the joint will be unstable with weak grip strength

36
Skier’s Thumb- Diagnosis
Difficulty opposing pinky to thumb Swelling and black and blue over thenar eminence Can’t hold an OK sign Consider digital block and to facilitate ligament testing Kim does not digital block, nor has she ever seen anybody do it

37
Stener Lesion Figure 8. Stener lesion. Note that the proximal end of the UCL displaces outside of the adductor aponeurosis. (UCL = ulnar collateral ligament.) Adductor Aponeurosis: fibers of the adductor pollicis tendon (intrinsic hand muscle) with fibers of the extensor aponeurosis One of the big debate is when to get the MRI. Pt. wants to avoid the OR. Fine after a cast for 6 weeks because stiff but will loosen up. MRI can help show the patient.
 Adductor Aponeurosis: fibers of the adductor pollicis tendon (intrinsic hand muscle) with fibers of the extensor aponeurosis. One of the big debate is when to get the MRI. Pt. wants to avoid the OR. Fine after a cast for 6 weeks because stiff but will loosen up. MRI can help show the patient.")
38
Skier’s Thumb Grading/Treatment
Grade 1 Pain without instability with stress Splinting 1-2 weeks Grade 2 Pain with mild instability: gapping <20 degrees Casting 3-6 weeks Grade 3 Stenner’s Lesion Instability: gapping > 20 degrees or > 35 degrees compared to unaffect thumb Early surgical intervention within 2-3 weeks

39
Skier’s Thumb Treatment

40
Finger Fractures

41
Distal Tuft Fractures Common due to crush injuries Painful
Splint in extension for 3 weeks

42
Proximal and Middle Phalange Fractures
Most common in athletes Fall or direct blunt trauma More difficult than metacarpal fractures Close relationship between fractured bone and pulley system

43
Rotational Alignment Figure 4.
Detecting rotation in middle phalanx fractures. If no rotation is present, all fingertips will be on the same plane and pointing toward the scaphoid bone. (A) No rotation. (B) Rotation. Reducing fractures? Hematoma block? Check the other hand, it can be the baseline Can passively extend the wrist and will cause the fingers to flex
 No rotation. (B) Rotation. Reducing fractures Hematoma block Check the other hand, it can be the baseline. Can passively extend the wrist and will cause the fingers to flex.")
44
Middle and Proximal Phalangeal Fractures
Might need Surgery: Inability to maintain proper alignment Rotation Irreducible Injury Intra-articular fracture

45
Finger Case 16 year old baseball player had a frustrating discussion with his coach about playing time so punched a locker. He immediately developed pain over the outside aspect of his right hand and lost the normal morphology of the 5th knuckle.

46
Metacarpal Fractures Common hand fracture Usually involves the neck
30-35% Usually involves the neck Fight or fall common mechanism 4TH and 5th most common fractures

47
Metacarpal Fracture Treatment
Angulation up to 40+ degrees can be tolerated Attempt reduction? Different cast types Statius, et al, Immediate immobilization gives good results in boxer’s fractures with volar angulation up to 70 degrees: a prospective randomized trial comparing immediate mobilization with cast immobolization. Arch Orthop Trauma Surg 2003;123:534-7 Kim rarely operates on these Statius, Arch Orthop Trauma Surg 2003;123:534-7

48
Metacarpal Shaft Fractures Diagnosis
Present with edema over the dorsum of the hand Point tender Ecchymosis The distal fragment usually displaces volarly due to the interosseous muscles Radiographs: AP, lateral, oblique

49
Metacarpal Fracture-Complications
Malrotation Common with spiral or oblique fractures Greater than 10% malrotation leads to scissoring effect of the fingers Metacarpal head Loss of knuckle Can you feel the metacarpal head in the palm- if hockey or stick handling can be a problem Can have an extensor lag that gets better over time

50
THUMB CMC FRACTURE DISLOCATION (BENNETT’S FRACTURE)
Anatomy: Anterior oblique carpometacarpal ligament holds palmar fragment in normal anatomic position Abductor pollicis longus (APL) pulls metacarpal shaft fragment radial & dorsal Treatment Reduction Traction, abduction, extension, pronation Often unstable, requires surgery AOCMC ligament also attaches to trapezium Triangular fragment = palmar beak fragment
 pulls metacarpal shaft fragment radial & dorsal. Treatment. Reduction. Traction, abduction, extension, pronation. Often unstable, requires surgery. AOCMC ligament also attaches to trapezium. Triangular fragment = palmar beak fragment.")
51
ROLANDO’S FRACTURE ANATOMY TREATMENT
3 part fracture at metacarpal base Comminuted with “Y” or “T” fragment TREATMENT May be non-surgical if highly comminuted Surgery if fragments are large and amenable

52
DIP JOINT DISLOCATION MECHANISM ANATOMY TREATMENT
Hyperextension, varus/valgus forces ANATOMY Usually dorsal Rare Strong collateral ligaments usually prevent TREATMENT Reduction: digital block first Splint in degrees flexion for days

53
PIP JOINT DORSAL DISLOCATION (COACH’S FINGER)
MECHANISM Hyperextension with disruption of volar plate ANATOMY Loss of volar stabilizing force causes phalanx to ride dorsally TREATMENT Reduction: avoid longitudinal traction Post-reduction: dorsal extension block splint with PIP blocked at degrees flexion BEWARE OF THE VOLAR DISLOCATION PROXIMAL PHALANX CONDYLE BUTTONHOLES THROUGH THE TORN EXTENSOR MECHANISM OFTEN CAN’T BE CLOSED REDUCED Bayonet deformity Traction allows for soft tissue interposition

54
Proximal PIP dorsal dislocation (Coach’s Finger)
Most common dislocated joint in the body Can injure the volar plate or cause an avulsion fracture of the middle phalanx The severity of this injury often is underestimated and improper treatment can cause long-term morbidity Figure 2. Reduction technique for proximal interphalangeal joint dislocations. Apply distal tension on the injured finger while applying volarly directed pressure to the middle phalanx. Hold the proximal phalanx in place while applying counterpressure.

55
Proximal PIP dorsal dislocation- Reduction
Reduce via minimal longitudinal traction If initially unsuccessful should hyperextend the distal portion to unlock I had to use sticky spray during football game one time Put the wrist into flexion because it relaxes the flexor tendon There is often a rotator component- a Chinese finger trap- gently

56
Post Reduction Care Radiographs should be obtained to ensure joint congruity Examine collaterals PIP should be splinted in less than 30 degrees X-ray in the splint Local for the dorsal V sign on the lateral

57
WRIST

58
Wrist Pathology Fracture Nerve Injury Ligament-Tendon Injuries Other
Scaphoid Ligament-Tendon Injuries TFCC tear Scapholunate dissociation DeQuervain’s Intersection Syndrome Ganglion Cyst Nerve Injury Carpal tunnel Other Kienbocks

59
Ganglion Cyst Account for 60% of soft tissue, tumor-like swelling affected the hand and wrist Develop spontaneously in year olds Female to male, 3:1 Cyst filled with soft, gelatinous, sticky, and mucoid fluid Location 65% dorsal scapholunate joint 20-25% volar distal aspect of the radius 10-15% flexor tendon sheath Mass generated from chronic irritation of the wrist that cause fluid production Excess fluid leaks into subcutaneous space where a cyst is formed

60
Ganglion Cyst Diagnosis
Usually obvious on exam- may be helpful to flex and extend wrist Radiographs, ultrasound, or MR not usually indicated If they have had trauma look for scapholunate dissocation They come from the SC joint

61
Ganglion Cyst- Treatment
Watchful waiting- most resolve spontaneously over time Aspiration/Injection No recurrence in 27-67% of patients Give patients reassurance when they see gelitanous fluid that it is not a cyst Can transiluminate

62
Ganglion Cyst Surgery Patient preference Pain Cosmetic?
20% recurrence rates Bump vs. a scar The smaller ones tend to be more painful -proximal interosseous nerve- motor branch of the radial nerve

63
Wrist Case 24-year-old male FOOSH (fell on outstretched hand) while skiing over the weekend Seen at the mountain clinic and told “wrist sprain”

64
Scaphoid Fracture Most common fractured bone in the wrist
Peanut shaped bone that spans both row of carpal bones Does not require excessive force and often not extremely painful so can be delayed presentation I have missed one of these- football player, initial x-ray was normal and pain was on his distal radius If missed can develop long term arthritis

65
Scaphoid Fracture Presentation
Pain over the anatomic snuff box Pain is not usually severe Often present late

66
Scaphoid Fracture Pathoanatomy
Blood supplied from distal pole In Adolescents, mostly involve distal pole In adults, mostly involve waist Treatment depends on location of fracture

67
Imaging AP, lateral, oblique and scaphoid view
Radiographs can be delayed for up to 4 weeks ?MRI, bone scan, or treat and repeat film

69
Scaphoid Fracture Imaging
Initial plain films often normal Bone scan 100% sensitive and 92% specific at 4 days MRI, CT scan

70
SCAPHOID FRACTURE TREATMENT Initial radiographs positive
distal third heal in approx 6-8 weeks middle third frx heal in 8-12 weeks proximal third heal in weeks Initial radiographs negative MRI Immobilize thumb spica cast x 7-14 days Take out of cast, re-evaluate for tenderness If +tenderness but neg radiographs….

71
Scaphoid Fracture Surgery: Angulated or displaced (1mm)
Non-union or AVN Scapholunate dissociation Proximal fractures Late presentation Early return to play

72
Non Operative Treatment- Disadvantages
Nonunion rate could be HIGH Mal-union “cast disease”- joint stiffness Prolonged immobilization- sometimes >12 weeks Loss of time from employment

73
Union Rates 100% High Union Rates- approaches 100% 73

74
Wrist Case 34-year-old female hairdresser with thumb pain for 2-3 months Gradual onset Now thumb hurts with any movement

75
Wrist Case 4 The College player starting softball shortstop presented with pain at the base of her left thumb. It was aggravated by hitting when she rolled her left hand over the top.

76
DeQuervain’s Tenosynovitis
Pain due to inflammation of the short extensor and abductor tendons of the thumb Repetitive or unaccustomed griping and grasping causes friction over the distal radial styloid

77
DeQuervain’s Tenosynovitis: Diagnosis
Swelling and pain over 1st dorsal compartment +Finkelstein’s test

78
DeQuervain’s Tenosynovitis: Treatment
Splint Injection- 1st line up to 90% are pain free if injected within 6 months Splinting performs poorly in comparison to steroid injection Post injection flare! Splint for a couple weeks after the injection Coldham F.. British Journal of Hand Therapy.2006

79
DeQuervain’s Tenosynovitis, Surgery
Recurrence despite repeated injections If don’t respond cut the sheet volarly

80
Wrist Case An College crew athlete presented following spring break training trip in Georgia. She reported pain distal dorsal forearm, accompanied by swelling, and palpable/audible crepitus.

81
Intersection syndrome
Friction point where muscle bellies of 1st compartment- APL, EPB cross 2nd and 3rd dorsal compartments Inflammatory peritendinitis Common with rowers due to clenched fist and thumb abduction Friction and crepitus felt 4-5cm proximal to radial styloid with rest flexion and extension and radial deviation Compartment1: (APL) abductor pollicus longus (mid ulna-base of 1st metacarpal), (EPB) Extensor pollicis brevis (distal ulna-base of proximal phalange) Compartment 2: Extensor carpi radialis longus (humerus-base of 2nd metacarpal), Extensor carpi radialis brevis (common extensor bundle to base of 3rd metacarpal) Compartment 3: Extensor pollicis Longus (distal to APL and proximal to EPB on the ulna-base of distal thumb phalange) About a 60 degree angle between. Also seen in skiers due to poling
 abductor pollicus longus (mid ulna-base of 1st metacarpal), (EPB) Extensor pollicis brevis (distal ulna-base of proximal phalange) Compartment 2: Extensor carpi radialis longus (humerus-base of 2nd metacarpal), Extensor carpi radialis brevis (common extensor bundle to base of 3rd metacarpal) Compartment 3: Extensor pollicis Longus (distal to APL and proximal to EPB on the ulna-base of distal thumb phalange) About a 60 degree angle between. Also seen in skiers due to poling.")
82
Intersection Syndrome Diagnosis
Pain and swelling about 2-3 finger breadths proximal to dorsal wrist joint Palpable crepitus (“squeaker’s wrist”) Fig. 2A. —28-year-old male tennis player who presented with tender mass on distal forearm. Axial T2-weighted fat-suppressed fast spin-echo image (TR/TEeff, 2,300/88) shows peritendinous and subcutaneous edema (arrow) in region of intersection of first extensor compartment and second extensor compartment tendons. Individual tendons are not well discerned.
 Fig. 2A. —28-year-old male tennis player who presented with tender mass on distal forearm. Axial T2-weighted fat-suppressed fast spin-echo image (TR/TEeff, 2,300/88) shows peritendinous and subcutaneous edema (arrow) in region of intersection of first extensor compartment and second extensor compartment tendons. Individual tendons are not well discerned.")
83
Intersection Syndrome Treatment
Splinting Activity modification Icing NSAIDS Corticosteroid injection Inject perpendicular

84
Intersection Syndrome Surgery
Failure of conservative measures Tenosynovectomy and fasciotomy of abductor pollicis longus can be performed

85
Wrist Case 25-year-old tennis player twists wrist as he falls backwards.

87
SCAPHOLUNATE DISSOCIATION

88
Scapholunate Dissociation
Most common ligamentous instability of the wrist Patients may have high degree of pain despite apparently normal radiographs Physicians should suspect this injury if patient has wrist effusion and pain seemingly out of proportion to the injury If improperly diagnosed can lead to chronic pain Located proximal axial line from 3rd metacarpal Also can lead to arthritis in years

89
Scapholunate Dissociation- Diagnosis
Exam Watson’s test Scaphoid shuck test Pain/swelling over dorsal wrist, proximal row Imaging Plain films: >3mm difference on clenched fist view Scaphoid ring sign Grab the distal pole scaphoid and then when radial deviate you should feel it push your finger away Always get comparison views The scaphoid falls into flexion and looks like a ring

90
Scapholunate Dissociation Treatment
If discovered within 4 weeks, surgery After 4 weeks, conservative treatment reasonable Bracing NSAIDS Delayed Surgery

91
Triangular Fibrocartilage Complex (TFCC) Tear
Fall on dorsiflexed and ulnar deviated wrist Axial load with forearm in hyperpronation

92
TFCC Anatomy

93
TFCC Tear Pathoanatomy
Tear in structures of TFCC Positive ulnar variance predisposes to injury

94
Triangular Fibrocartilage Complex (TFCC) Tear
Fall on dorsiflexed and ulnar deviated wrist Axial load with forearm in hyperpronation Positive ulnar variance predisposes to injury Because they bear more weight at the wrist, Normally 80/20 but longer ulna is 60/40 - Measurement: - requires zero rotation view: (measured on PA radiograph w/ wrist in neutral supination/pronation); - draw transverse line at the level of the lunate fossa, and a second transverse line at the level of the ulnar head; - the difference indicates ulnar variance;
; - draw transverse line at the level of the lunate fossa, and a second transverse line at the level of the ulnar head; - the difference indicates ulnar variance;")
95
TFCC Tear History Ulnar-sided wrist pain aggravated by pronation/ supination

96
TFCC Tear Physical Exam
Press test TFCC grind test Check for DRUJ injury

97
TFCC Tear Diagnosis Exam Imaging Ulnar sided wrist pain
Often experience a click Imaging Radiographs MR arthrogram

98
TFCC Tear Treatment Splinting Time Injection Surgical treatment
Debridement Repair Open vs. arthroscopic Ulnar shortening osteotomy

99
TFCC Tear Treatment Ulnar shortening osteotomy

100
GOLFER’S FRACTURE Hook of hamate fracture
Swing of golf club 2% of all carpal fractures 1/3 of all hamate fractures = golf related Distal lateral border of Guyon’s Canal High rate of non-union May consider early operative treatment

102
GOLFER’S FRACTURE CARPAL TUNNEL VIEW

103
GUYON’S CANAL SYNDROME
ANATOMY Ulnar nerve rides between pisiform and hamate Feeds interosseous muscles, hypothenar muscles, lumbricals (intrinsic muscles) TREATMENT Pad area NSAIDS r/o hamate fracture Pisohamate ligament Volar carpal ligament Transverse carpal ligament
 TREATMENT. Pad area. NSAIDS. r/o hamate fracture. Pisohamate ligament. Volar carpal ligament. Transverse carpal ligament.")
104
Finger injuries in rock climbing

105
Rock climbing is an increasingly popular recreational activity despite the obvious inherent risks

106
Rock Climbing

107
Traditional Leading

108
Sport Climbing

109
Competitive Disciplines

111
Climbing Injuries Climbers are susceptible to overuse injuries of the upper limb: Studies consistently report a high prevalence of finger related injuries (Jones et al, 2008; Shoffl et al, 2003) Disruption of the annular pulley system (particularly A2) Rotator cuff and shoulder impingement syndromes which are associated with prolonged and repeated reaching overhead (Peters, 2001) Tendonopathies
 Disruption of the annular pulley system (particularly A2) Rotator cuff and shoulder impingement syndromes which are associated with prolonged and repeated reaching overhead (Peters, 2001) Tendonopathies.")
112
Why are the fingers susceptible ?
During the crimp grip wrist extension increases the mechanical advantage of the finger flexors and reduces active insufficiency (Lockwood, 1998) Paradoxically this hand position may increase the pre-disposition of the climber to injury (Joel et al, 2000)
 Paradoxically this hand position may increase the pre-disposition of the climber to injury (Joel et al, 2000)")
113
Why the 3rd & 4th fingers ? Flexion of the remaining fingers when holding a one finger pocket may increase the maximum holding force up to 48% (Shweizer, 2001) Lumbrical tears to the third or fourth lumbrical may occur if the finger is dynamically loaded (Shweizer 2003) Due to the musculotendonous interconnection of flexor digitorum profundus
 Lumbrical tears to the third or fourth lumbrical may occur if the finger is dynamically loaded (Shweizer 2003) Due to the musculotendonous interconnection of flexor digitorum profundus.")
114
Carpal Tunnel Syndrome
Most common nerve entrapment disorder Pain and parasthesias from high pressures in the carpal tunnel causing compression and inflammation of the median nerve Carpal bones dorsally and transverse carpal ligament (flexor retinaculum) ventrally Median nerve compression: osteoarthritis, rheumatoid arthritis, diabetes, hypothyroidism, repetitive use, trauma, pregnancy
 ventrally. Median nerve compression: osteoarthritis, rheumatoid arthritis, diabetes, hypothyroidism, repetitive use, trauma, pregnancy.")
115
Carpal tunnel syndrome

116
Hand Diagrams Tinel + hand diagram – PPV = 0.71
Ann Intern Med 1990 Mar 1;112(5):321-7.
:")
117
Carpal Tunnel Syndrome
Always compare with the unaffected side Document when phalen’s becomes + Durken’s compressive test- higher sensitivity

118
Sensitivity and Specificity
For both Phalen’s and Tinel’s is LOW High Combined with hand diagram and history Ann Intern Med 1990 Mar 1;112(5):321-7
:")
119
Nerve Conduction Study
Can be painful and costly Reserve for patients who have failed conservative therapy diagnosis is uncertain late presentation with thenar wasting and motor dysfunction False negative rates as high as 10% AAOS guideline However, does not help surgery decision Can help with mild carpal tunnel -night time symptoms Operate Always have symptoms Dennervation of thenar muscles J Hand Surg [Am] 1995 Sep;20(5):848-54
:")
120
Carpal Tunnel Syndrome Diagnosis
Pain involves thumb, first two fingers and radial half of the fourth finger Palpation: thenar eminence wasting ROM: thumb weakness and difficulty pincher grasping Diagnostic Tests or special maneuvers Nerve conduction studies Tinel’s Phalen’s Night time symptoms most common

121
Carpal Tunnel Syndrome Treatment
Ice Activity modification Workspace modification Splinting Injection Surgery

122
Carpal Tunnel Injection
Short term efficacy: RCT, 70% vs 34% at 2 weeks Long-term benefits are more variable 43% of patients above required referral to surgery Should not inject into the nerve -the median nerve can go out- should not inject severe carpal tunnel- wrist to surgery Good for pregnant people Kim does not inject- Pregnancy Old people trauma Injection technique: 23-25g needle: 20-40mg Methylprednisolone. Muscle Nerve 2004 Jan;29(1):82-8
:82-8.")
123
Carpal Tunnel Syndrome Surgery
Constant numbness and tingling Thenar eminence wasting If get EMG: Severe carpal tunnel or dennervation

125
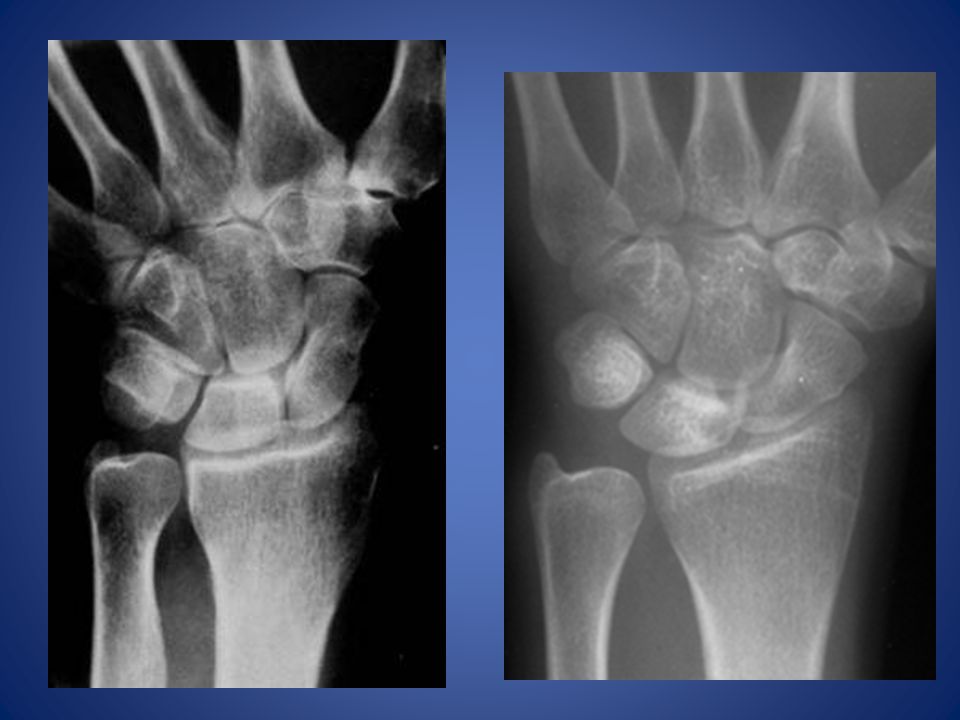
Kienbock Disease Lunatomalacia
Avascular necrosis/vascular insufficiency ?repetitive microfractures of lunate Young adults yo Risk factors: negative ulnar variance

126
Kienbock Disease EXAM:: Wrist pain that radiates up the forearm
stiffness, tenderness, swelling over lunate passive dorsiflexion of middle finger produces characteristic pain

127
Kienbock Disease Stage I – IV Stage I: MRI only Stage II: Sclerosis
Stage III: Some collapse Stage IV: Total collapse

128
Kienbock Disease TREATMENT: Surgical
EARLY: Radial shortening, ulnar lengthening LATE: proximal row carpectomy, arthrodesis Reduce ulnar load

129
References Hand Surgery Textbooks Allyson S. Howe, MD
Andrew Getzin, MD Gareh Jones

Similar presentations