Download presentation
Presentation is loading. Please wait.

1
The Hematopoietic and Lymphoid Systems Richard D. Boucher, MD Clinical Medicine II Adjunct Faculty, SCCO

2
Introduction This is a wide range of interlocking diseases sorted into disorders that affect red cells, white cells, or the hemostatic system which includes platelets and clotting factors This is a wide range of interlocking diseases sorted into disorders that affect red cells, white cells, or the hemostatic system which includes platelets and clotting factors Red cell disorders lead to anemia or red cell deficiency Red cell disorders lead to anemia or red cell deficiency White cell disorders caused by excessive proliferation having a neoplastic basis White cell disorders caused by excessive proliferation having a neoplastic basis Hemostatic disorders result in hemorrhagic diathesis i.e. bleeding disorders Hemostatic disorders result in hemorrhagic diathesis i.e. bleeding disorders The Hematopoietic/Lymphoid system comprises the circulation blood, bone marrow, spleen, liver, lymph nodes, and reticuloendothelial system The Hematopoietic/Lymphoid system comprises the circulation blood, bone marrow, spleen, liver, lymph nodes, and reticuloendothelial system

3
Red Cell Disorders Can result in Can result in –Anemia A reduction in normal circulating levels of hemoglobin and red cell mass (hematocrit) A reduction in normal circulating levels of hemoglobin and red cell mass (hematocrit) Results in reduced oxygen carrying capacity of the blood Results in reduced oxygen carrying capacity of the blood Causes Causes –Hemorrhage –Hemolysis –Diminished erythropoiesis –Polycythemia An increase in the number of red cells An increase in the number of red cells
 A reduction in normal circulating levels of hemoglobin and red cell mass (hematocrit) Results in reduced oxygen carrying capacity of the blood Results in reduced oxygen carrying capacity of the blood Causes Causes –Hemorrhage –Hemolysis –Diminished erythropoiesis –Polycythemia An increase in the number of red cells An increase in the number of red cells")
4
Anemias Classification Classification –Cell size Normocytic Normocytic Microcytic Microcytic Macrocytic Macrocytic –Degree of hemoglobinization Normochromic Normochromic Hypochromic Hypochromic –Shape of the cell

5
Anemia Clinical consequences depend on Clinical consequences depend on –Severity –Speed of onset Acute Acute Chronic Chronic –Pathological cause

6
Complete Blood Count (CBC) In order to understand the abnormalities one must understand what comprises a CBC and the normal values In order to understand the abnormalities one must understand what comprises a CBC and the normal values CBC CBC –WBC Differential Differential –RBC –Hemoglobin –Hematocrit –Platelets –Indices of RBC Mean cell volume (MCV) Mean cell volume (MCV) Mean cell hemoglobin (MCH) Mean cell hemoglobin (MCH) Mean cell hemoglobin concentration (MCHC) Mean cell hemoglobin concentration (MCHC)
 In order to understand the abnormalities one must understand what comprises a CBC and the normal values In order to understand the abnormalities one must understand what comprises a CBC and the normal values CBC CBC –WBC Differential Differential –RBC –Hemoglobin –Hematocrit –Platelets –Indices of RBC Mean cell volume (MCV) Mean cell volume (MCV) Mean cell hemoglobin (MCH) Mean cell hemoglobin (MCH) Mean cell hemoglobin concentration (MCHC) Mean cell hemoglobin concentration (MCHC)")
7
Laboratory CBC

8
Normal Red Blood Cells

10
Anemia Symptoms – common to all anemias Symptoms – common to all anemias –Pallor check palpebral side of conjunctiva check palpebral side of conjunctiva –Fatigue –Lassitude Hemolytic anemias Hemolytic anemias –Hyperbilirubinemia –Jaundice Ineffective hematopoiesis Ineffective hematopoiesis –Iron overload – increased absorption

11
Anemia of Blood Loss Hemorrhage Hemorrhage –Acute Can cause shock Can cause shock Hemodilution occurs which reveals the extent of the blood loss Hemodilution occurs which reveals the extent of the blood loss Normocytic and normochromic Normocytic and normochromic Erythropoietin levels rises - reticulocytosis Erythropoietin levels rises - reticulocytosis Due to trauma, ulceration, bleeding disorder Due to trauma, ulceration, bleeding disorder –Chronic Iron stores gradually lost, then anemia appears Iron stores gradually lost, then anemia appears Leads to anemia of underproduction Leads to anemia of underproduction Due to NSAID abuse, cancer, etc. Due to NSAID abuse, cancer, etc.

12
Anemia of Blood Loss Hemorrhage Hemorrhage –Internal Iron is saved and can be used again Iron is saved and can be used again –External Iron is lost and without adequate replacement can cause iron deficiency anemia Iron is lost and without adequate replacement can cause iron deficiency anemia

13
Hemolytic Anemias Normal life span of an RBC is 120 days Normal life span of an RBC is 120 days Destruction can be caused by Destruction can be caused by –Red cell defects –External factors – autoantibodies, chemicals, toxins, parasites Characteristics Characteristics –Increased rate of cell destruction –Erythropoiesis -> reticulocytosis –Iron retention Hemolysis Hemolysis –Intravascular Mechanical trauma – bad heart valves Mechanical trauma – bad heart valves Biochemical/physical agents Biochemical/physical agents Hemoglobinemia and hemoglobinuria Hemoglobinemia and hemoglobinuria –Extravascular More common More common Takes place in spleen or liver Takes place in spleen or liver

14
Hemolytic Anemias Hereditary Spherocytosis Hereditary Spherocytosis –Intrinsic defect in the red cell membrane –Cells are spherical instead of a biconcave disc –Cells are sequestered in the spleen –Clinical features Anemia, splenomegaly, jaundice Anemia, splenomegaly, jaundice –Treatment Splenectomy Splenectomy –Risk of susceptibility to infections

15
Spherocytosis

16
Spherocytosis

17
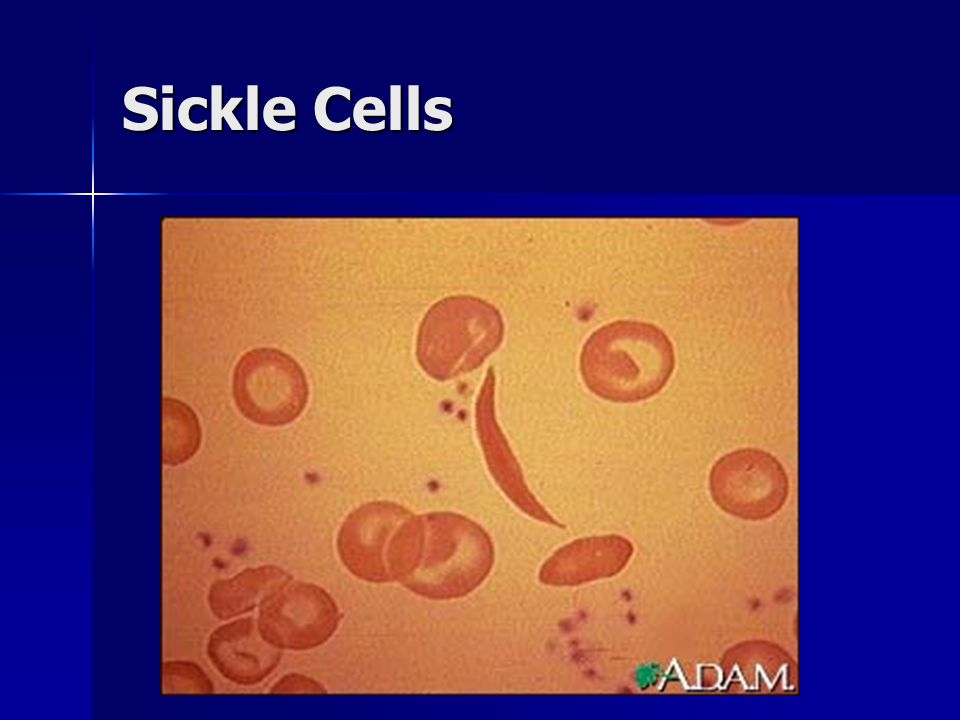
Hemolytic Anemias Sickle Cell Anemia Sickle Cell Anemia –Problem with structurally abnormal hemoglobin (hemoglobinopathy) –Normal hemoglobin HbA - 96% HbA - 96% HbA2 – 3% HbA2 – 3% HbF - 1% HbF - 1% –Sickle cell disease - HbS replaces all HbA –Sickle cell trait - HbS replaces half of HbA –Sickling occurs with slow blood flow Spleen, bone marrow Spleen, bone marrow Areas of inflammation, infection, dehydration Areas of inflammation, infection, dehydration
 –Normal hemoglobin HbA - 96% HbA - 96% HbA2 – 3% HbA2 – 3% HbF - 1% HbF - 1% –Sickle cell disease - HbS replaces all HbA –Sickle cell trait - HbS replaces half of HbA –Sickling occurs with slow blood flow Spleen, bone marrow Spleen, bone marrow Areas of inflammation, infection, dehydration Areas of inflammation, infection, dehydration")
18
Sickle Cells

20
Hemolytic Anemias Sickle Cell Anemia Sickle Cell Anemia –Hematocrit – 18-30% –Disease apparent after 6 months of age (HbF) –Pain can occur in many areas but bone is most common Acute chest syndrome Acute chest syndrome CNS stroke CNS stroke –Autosplenectomy –Treatment Oxygen Oxygen IV fluids IV fluids Pain management Pain management Antibiotics Antibiotics
 –Pain can occur in many areas but bone is most common Acute chest syndrome Acute chest syndrome CNS stroke CNS stroke –Autosplenectomy –Treatment Oxygen Oxygen IV fluids IV fluids Pain management Pain management Antibiotics Antibiotics")
21
Hemolytic Anemias Thalassemia Thalassemia –Microcytic/hypochromic anemia –Indices may look like iron deficiency anemia –Major Treated with transfusions Treated with transfusions Caution with increased iron – use chelators Caution with increased iron – use chelators –Minor No need to treat but diagnosis is important No need to treat but diagnosis is important Beta thalassemia minor – dx with Hb electrophoresis Beta thalassemia minor – dx with Hb electrophoresis

22
Hemolytic Anemias Mechanical trauma to cells Mechanical trauma to cells Red cells are disrupted by physical trauma (traumatic hemolytic anemia) Red cells are disrupted by physical trauma (traumatic hemolytic anemia) –Cardiac valve prosthesis –Narrowing/partial obstruction of vasculature –Mechanical valves shear red blood cells
 Red cells are disrupted by physical trauma (traumatic hemolytic anemia) –Cardiac valve prosthesis –Narrowing/partial obstruction of vasculature –Mechanical valves shear red blood cells")
23
Hemolytic Anemias Malaria Malaria –Endemic in Asia and Africa –Malarial parasite is released approximately every 48 hours Causes shaking, chills, fever Causes shaking, chills, fever –Red cells are destroyed –Protective effect of HbS against malaria

24
Anemias of Diminished Erythropoiesis Caused by inadequate dietary supply of substances for hematopoiesis Caused by inadequate dietary supply of substances for hematopoiesis –Iron, folic acid and vitamin B12 Bone marrow failure or replacement by tumor or inflammatory cells Bone marrow failure or replacement by tumor or inflammatory cells Iron deficiency anemia Iron deficiency anemia –Affects 10% of population in developed countries –Due to diet, chronic slow blood loss – peptic ulcers, colon cancer, hemorrhoids, menses –Microcytic/hypochromic anemia –Iron absorbed in duodenum –Clinical symptoms Asymptomatic Asymptomatic Weakness, listlessness, pallor Weakness, listlessness, pallor Pica – neurobehavioral to eat dirt or clay Pica – neurobehavioral to eat dirt or clay –Lab tests

25
Anemias of Diminished Erythropoiesis Megaloblastic anemias Megaloblastic anemias –Folate (folic acid) deficiency Macrocytic anemia Macrocytic anemia Due to poor diet Due to poor diet Destroyed by 10-15 minutes of cooking Destroyed by 10-15 minutes of cooking Associated with pregnancy and alcohol abuse Associated with pregnancy and alcohol abuse Absorbed in upper 1/3 of the small intestine Absorbed in upper 1/3 of the small intestine Clinical symptoms Clinical symptoms –Weakness –Easy fatigability –No neurological abnormalities
 deficiency Macrocytic anemia Macrocytic anemia Due to poor diet Due to poor diet Destroyed by minutes of cooking Destroyed by minutes of cooking Associated with pregnancy and alcohol abuse Associated with pregnancy and alcohol abuse Absorbed in upper 1/3 of the small intestine Absorbed in upper 1/3 of the small intestine Clinical symptoms Clinical symptoms –Weakness –Easy fatigability –No neurological abnormalities")
26
Anemias of Diminished Erythropoiesis Vitamin B12 deficiency – pernicious anemia Vitamin B12 deficiency – pernicious anemia –Macrocytic anemia –Can be due to dietary problems –Most common problem is malabsorption Due to autoimmune reaction against intrinsic factor Due to autoimmune reaction against intrinsic factor Gastrectomy Gastrectomy Resection of the ileum Resection of the ileum Diseases involving the distal ileum – Crohn’s disease Diseases involving the distal ileum – Crohn’s disease –Clinical symptoms pallor, easy fatigability pallor, easy fatigability Neurological – symmetric numbness, tingling, burning in hands or feet Neurological – symmetric numbness, tingling, burning in hands or feet Unsteadiness of gait, loss of position sense Unsteadiness of gait, loss of position sense

27
Anemias of Diminished Erythropoiesis Aplastic anemia Aplastic anemia –Multipotent myeloid stem cells are suppressed –Marrow failure and pancytopenia –Causes Idiopathic – 50% of cases Idiopathic – 50% of cases Myelotoxic drugs – antineoplastic drugs Myelotoxic drugs – antineoplastic drugs Chloramphenicol Chloramphenicol Sulfonamides – hypersensitivity reaction Sulfonamides – hypersensitivity reaction Certain viral infections Certain viral infections –Clinical course Anemia – weakness, pallor, dyspnea Anemia – weakness, pallor, dyspnea Thrombocytopenia – petechiae, ecchymosis Thrombocytopenia – petechiae, ecchymosis Granulocytopenia – infections, fever, chills, prostration Granulocytopenia – infections, fever, chills, prostration

28
Laboratory Diagnosis of Anemia Hemoglobin electrophoresis Hemoglobin electrophoresis Coombs test Coombs test Reticulocyte count Reticulocyte count Iron indices Iron indices Folate and vitamin B12 concentrations Folate and vitamin B12 concentrations Unconjugated bilirubin levels Unconjugated bilirubin levels

29
Polycythemia Increase in blood cell concentration of red cells Increase in blood cell concentration of red cells Correlates with increase in hemoglobin concentration Correlates with increase in hemoglobin concentration Ocular manifestation – dilated, engorged, and tortuous retinal veins and arteries Ocular manifestation – dilated, engorged, and tortuous retinal veins and arteries Blood is “thick” leading to thrombosis Blood is “thick” leading to thrombosis Types Types –Relative – hemoconcentration due to decrease in plasma volume – dehydration, vomiting, diarrhea, diuretics –Absolute – increase in total red cell mass Primary – uncontrolled overproduction of RBC’s – malignancy Primary – uncontrolled overproduction of RBC’s – malignancy –Known as Polycythemia vera – Hct – 20-25 Secondary - response to increase of erythropoietin - hypoxia Secondary - response to increase of erythropoietin - hypoxia

30
White Cell Disorders Non-neoplastic Non-neoplastic –Leucopenia – decrease in white cells More specifically neutropenia – decrease in granulocytes More specifically neutropenia – decrease in granulocytes WBC count < 1000 WBC count < 1000 More susceptible to bacterial and fungal infections More susceptible to bacterial and fungal infections Due to marrow failure, chemotherapy, immune-mediated injury to neutrophils (triggered by some drugs or idiopathic) Due to marrow failure, chemotherapy, immune-mediated injury to neutrophils (triggered by some drugs or idiopathic) Clinical symptoms Clinical symptoms –Malaise, chills, fever, weakness, fatigability –Reactive leucocytosis Increase in number of white cells due to inflammatory reaction – infection, allergy Increase in number of white cells due to inflammatory reaction – infection, allergy
 Due to marrow failure, chemotherapy, immune-mediated injury to neutrophils (triggered by some drugs or idiopathic) Clinical symptoms Clinical symptoms –Malaise, chills, fever, weakness, fatigability –Reactive leucocytosis Increase in number of white cells due to inflammatory reaction – infection, allergy Increase in number of white cells due to inflammatory reaction – infection, allergy")
31
White Cell Disorders Neoplastic Neoplastic –Lymphomas Non-Hodgkin Non-Hodgkin Hodgkin Hodgkin –Leukemias Lymphocytic Lymphocytic Myelogenous Myelogenous –Plasma cell dyscrasias

32
Lymphomas Non-Hodgkin lymphomas Non-Hodgkin lymphomas –A heterogeneous group of cancers of lymphocytes –Malignant proliferation of lymphoid cells –Arise anywhere in the body where there is lymphatic tissue –Classification of lymphomas is controversial and undergoing evolution

33
Lymphomas Non-Hodgkin Lymphomas Non-Hodgkin Lymphomas –Symptoms and signs Painless lymphadenopathy Painless lymphadenopathy –Isolated –Extranodal – skin, GI tract Advanced disease Advanced disease –Night sweats, weight loss, weakness, anemia, metastasis Laboratory work-up Laboratory work-up –CXR –CT scan of abdomen and pelvis –Bone marrow biopsy –Serum LDH – useful prognostic marker –Tissue bx needed for Dx – lymph bx or bx of extra-nodal tissue Needle aspiration may yield suspicious results Needle aspiration may yield suspicious results Treatment Treatment –Depends on stage of disease and clinic status of patient –Oncology consult

34
Lymphomas Hodgkin’s Lymphoma (disease) Hodgkin’s Lymphoma (disease) –Characterized by Reed-Sternberg cells –Bimodal age distribution One peak in the 20’s, second over age 50 One peak in the 20’s, second over age 50 –Patient presents with a painless mass in neck –May have fever, weight loss, night sweats, generalized pruritus
 Hodgkin’s Lymphoma (disease) –Characterized by Reed-Sternberg cells –Bimodal age distribution One peak in the 20’s, second over age 50 One peak in the 20’s, second over age 50 –Patient presents with a painless mass in neck –May have fever, weight loss, night sweats, generalized pruritus")
35
Lymphomas Hodgkin’s Lymphoma Hodgkin’s Lymphoma –Staging nomenclature (Ann Arbor) Stage I – one lymph node region involved Stage I – one lymph node region involved Stage II – two lymph node areas involved on one side of the diaphragm Stage II – two lymph node areas involved on one side of the diaphragm Stage III – lymph node regions involved on both sides of the diaphragm Stage III – lymph node regions involved on both sides of the diaphragm Stage IV – disseminated disease with bone marrow or liver involvement Stage IV – disseminated disease with bone marrow or liver involvement In addition In addition –Stage A – patient lacks constitutional symptoms –Stage B – 10% weight loss over 6 months, fever or night sweats are present –Treatment Radiation/chemotherapy Radiation/chemotherapy Lararotomy no longer routinely performed Lararotomy no longer routinely performed
 Stage I – one lymph node region involved Stage I – one lymph node region involved Stage II – two lymph node areas involved on one side of the diaphragm Stage II – two lymph node areas involved on one side of the diaphragm Stage III – lymph node regions involved on both sides of the diaphragm Stage III – lymph node regions involved on both sides of the diaphragm Stage IV – disseminated disease with bone marrow or liver involvement Stage IV – disseminated disease with bone marrow or liver involvement In addition In addition –Stage A – patient lacks constitutional symptoms –Stage B – 10% weight loss over 6 months, fever or night sweats are present –Treatment Radiation/chemotherapy Radiation/chemotherapy Lararotomy no longer routinely performed Lararotomy no longer routinely performed")
36
Leukemias Acute Leukemia Acute Leukemia –Malignancy of the hematopoietic progenitor cell –Cells lose their ability to mature and differentiate, proliferate in an uncontrolled fashion and replace normal bone marrow –Causes Most have no clear cause Most have no clear cause Radiation Radiation Toxins (benzene) Toxins (benzene) Chemotherapy Chemotherapy
 Toxins (benzene) Chemotherapy Chemotherapy")
37
Leukemias Acute Lymphocytic Leukemia (ALL) Acute Lymphocytic Leukemia (ALL) –Rapid onset of very high lymphocyte count, very immature, malignant cells (blasts) –Symptoms related to depressed bone marrow Fatigue – anemia Fatigue – anemia Fever – infections Fever – infections Bleeding – thrombocytopenia Bleeding – thrombocytopenia Bone pain – marrow expansion Bone pain – marrow expansion Lymphadenopathy, splenomegaly, hepatomegaly Lymphadenopathy, splenomegaly, hepatomegaly Headache, vomiting, nerve palsies – meningeal spread Headache, vomiting, nerve palsies – meningeal spread –Lab findings WBC can be > 100,000 WBC can be > 100,000 Platelets < 100,000 Platelets < 100,000
 Acute Lymphocytic Leukemia (ALL) –Rapid onset of very high lymphocyte count, very immature, malignant cells (blasts) –Symptoms related to depressed bone marrow Fatigue – anemia Fatigue – anemia Fever – infections Fever – infections Bleeding – thrombocytopenia Bleeding – thrombocytopenia Bone pain – marrow expansion Bone pain – marrow expansion Lymphadenopathy, splenomegaly, hepatomegaly Lymphadenopathy, splenomegaly, hepatomegaly Headache, vomiting, nerve palsies – meningeal spread Headache, vomiting, nerve palsies – meningeal spread –Lab findings WBC can be > 100,000 WBC can be > 100,000 Platelets < 100,000 Platelets < 100,000")
38
Leukemias Chronic Lymphocytic Leukemia (CLL) Chronic Lymphocytic Leukemia (CLL) –Slow onset, not Dx’d for months –WBC count can be >200,000 but are not as malignant in characteristic as with ALL –Peripheral blood lymphocytosis >4000 –Symptoms Asymptomatic at first Asymptomatic at first Fatigue, weight loss, anorexia Fatigue, weight loss, anorexia Lymphadenopathy, hepatomegaly Lymphadenopathy, hepatomegaly Discovered on routine blood exam Discovered on routine blood exam
 Chronic Lymphocytic Leukemia (CLL) –Slow onset, not Dx’d for months –WBC count can be >200,000 but are not as malignant in characteristic as with ALL –Peripheral blood lymphocytosis >4000 –Symptoms Asymptomatic at first Asymptomatic at first Fatigue, weight loss, anorexia Fatigue, weight loss, anorexia Lymphadenopathy, hepatomegaly Lymphadenopathy, hepatomegaly Discovered on routine blood exam Discovered on routine blood exam")
39
Leukemias Acute Myelogenous Leukemia (AML) Acute Myelogenous Leukemia (AML) –Affects older adults, median age 50 –Bone marrow replaced with myeloblasts –Signs and symptoms closely resemble ALL Fatigue, pallor, abnormal bleeding, infections Fatigue, pallor, abnormal bleeding, infections
 Acute Myelogenous Leukemia (AML) –Affects older adults, median age 50 –Bone marrow replaced with myeloblasts –Signs and symptoms closely resemble ALL Fatigue, pallor, abnormal bleeding, infections Fatigue, pallor, abnormal bleeding, infections")
40
Leukemias Chronic Myelogenous Leukemia (CML) Chronic Myelogenous Leukemia (CML) –Affects adults between age 25 and 60 yrs –Has Philadelphia chromosome –WBC > 100,000; increased granulocytes –Slow onset, nonspecific symptoms Easy fatigability, weakness, weight loss Easy fatigability, weakness, weight loss –Treatment – bone marrow transplant
 Chronic Myelogenous Leukemia (CML) –Affects adults between age 25 and 60 yrs –Has Philadelphia chromosome –WBC > 100,000; increased granulocytes –Slow onset, nonspecific symptoms Easy fatigability, weakness, weight loss Easy fatigability, weakness, weight loss –Treatment – bone marrow transplant")
41
Plasma Cell Dyscrasias Originates from a clone of B cells that differentiate into neoplastic plasma cells and secrete a single immunoglobulin Originates from a clone of B cells that differentiate into neoplastic plasma cells and secrete a single immunoglobulin Most common is marked secretion of light chains in the urine called Bence-Jones proteins Most common is marked secretion of light chains in the urine called Bence-Jones proteins Multiple Myeloma Multiple Myeloma –Most common –Multifocal lytic lesions throughout the skeletal system –50 – 60 y/o –Bone pain, pathologic fractures, hypercalcemia (confusion, lethargy), infections, hyperviscosity syndrome, renal insufficiency
, infections, hyperviscosity syndrome, renal insufficiency")
42
Lytic Bone Lesions

45
Bleeding Disorders Abnormal bleeding Abnormal bleeding –Blood vessel wall, platelets, clotting cascade –Spontaneous –Inciting event such trauma or surgery Causes Causes –Increased vessel fragility Vitamin C deficiency Vitamin C deficiency Steroid use Steroid use Infectious and hypersensitivity vasculitides Infectious and hypersensitivity vasculitides Petechiae and ecchymosis in skin and mucus membranes Petechiae and ecchymosis in skin and mucus membranes –Deficiencies of platelets (thrombocytopenia) Number Number Function – aspirin, von Willebrand disease Function – aspirin, von Willebrand disease Signs – easy bruising, nosebleeds, excessive bleeding from minor trauma Signs – easy bruising, nosebleeds, excessive bleeding from minor trauma –Derangements of clotting mechanisms
 Number Number Function – aspirin, von Willebrand disease Function – aspirin, von Willebrand disease Signs – easy bruising, nosebleeds, excessive bleeding from minor trauma Signs – easy bruising, nosebleeds, excessive bleeding from minor trauma –Derangements of clotting mechanisms")
46
Coagulation Disorders Deficiencies in clotting factors Deficiencies in clotting factors Vitamin K is essential for synthesis of prothrombin and clotting factors VII, IX, and X Vitamin K is essential for synthesis of prothrombin and clotting factors VII, IX, and X Liver is site of synthesis of several coagulation factors Liver is site of synthesis of several coagulation factors Parenchymal diseases of the liver cause hemorrhagic diatheses Parenchymal diseases of the liver cause hemorrhagic diatheses von Willebrand disease von Willebrand disease –Defect in platelet function and depressed Factor VIII level –Spontaneous bleeding from mucus membranes –Excessive bleeding from wounds –menorrhagia Factor VIII deficiency (Hemophilia A) Factor VIII deficiency (Hemophilia A) –Reduction in Factor VIII activity –Easy bruising, massive hemorrhage after trauma –Treatment – infusion of Factor VIII (prepared from human plasma)
 Factor VIII deficiency (Hemophilia A) –Reduction in Factor VIII activity –Easy bruising, massive hemorrhage after trauma –Treatment – infusion of Factor VIII (prepared from human plasma)")
Similar presentations














. Complete Blood Count ( CBC)>")





:>")

