Download presentation
Presentation is loading. Please wait.

1
Acute Upper Extremity Injuries
CPT William Cooper D.O. Department of Orthopaedic Surgery DeWitt Army Community Hospital

2
Topics Reviewed Pectoralis Rupture AC joint sprains
Shoulder dislocations Clavicular fractures Biceps Rupture Radial head fractures Elbow Dislocation Skier’s thumb Perilunate injuries Scaphoid fractures TFCC tears Jersey Finger Mallet Finger Sagittal Band rupture

5
Pectoralis Major Rupture
Excessive tension on maximally eccentrically contracted muscle Weightlifters Localized swelling and ecchymosis Palpable defect Weakness with adduction and internal rotation Most common in men 20-50 Complete rupture most common

7
Pectoralis Major Rupture
Treatment Surgical repair to bone for complete tears Nonoperative for partial tears Outcome Less than ideal Weakness, decreased ROM, increased muscle fatigue Cosmesis

8
AC joint sprains AKA “separated shoulder” Mechanism:
Blow to top of shoulder May result from fall onto outstretched arm or elbow Focal tenderness and pain with shoulder motion Cross-chest adduction test usually positive

9
Cross-Chest Adduction Test
AC joint Adduct shoulder Patient pushes elbow up against resistance Pain in AC = + test false + test in RC pathology

10
Types of AC joint sprains
Type 1: mild injury of the AC ligaments Type II: AC lig's disrupted only Type III: AC and coracoclavicular lig's disrupted Type IV: Clavicle displaced posteriorly through trapezius; AC and CC lig's disrputed. Type V: AC joint dislocation with extreme superior elevation of the clavicle. Type VI: clavicle displaced inferior to acromion and coracoid process.

11
AC joint sprains: Radiology eval
Standard AP shoulder views inadequate usually over-penetrate the AC joint Image both sides for comparison Get specific AC joint view (Zanca) AP with 10° cephalic incline Axillary view can show posterior dislocation
 AP with 10° cephalic incline. Axillary view can show posterior dislocation.")
12
Normal AC joint

13
Grade II AC joint sprain

14
Grade III AC joint sprain

15
Weighted AC x-rays seldom unmask unstable injures
Bossart PJ et al. Lack of efficacy of “weighted” radiographs in diagnosing acute acromioclavicular separations. Ann Emerg Med 1988; 117:20-24.

16
Management of mild AC joint sprains (types I and II)
Ice, analgesia Sling 1-3 weeks Early ROM as pain permits Strength exercises after full ROM achieved Return to sports after pain-free function achieved

17
Management of type III AC joint sprints
Initially same as for I and II Referral to ortho advisable within 72 hours Most authors advocate conservative management Outcome just as good as surgery, with quicker recovery time

18
Acute management of severe AC joint sprains (types IV, V, VI)
Ice, analgesia Management of any complications (type VI associated with clavicle fxs, rib fxs, and brachial plexus injuries) Sling/swath Early referral
 Sling/swath. Early referral.")
19
Clavicular Fractures One of the most common fractures Classification
Middle third - most common (thinnest section) Distal third Proximal third Image with AP thorax and 45° AP cephalic tilt Rule out neurological or vascular compromise; pneumothorax in 3%
 Distal third. Proximal third. Image with AP thorax and 45° AP cephalic tilt. Rule out neurological or vascular compromise; pneumothorax in 3%")
21
Lateral third clavicle fracture

22
ER Management of Clavicular Fractures
Ice, analgesics, arm support for all Referral rule: Any displaced, non-middle-third fractures Shortening/displacement >2cm Non-displaced fxs: sling; ROM prn comfort Displaced middle-third fractures: figure 8 splint Re-image in 7 days to assure reduction. If not, refer for shoulder spica cast

23
Shoulder dislocations
Most commonly dislocated large joint Anterior in 97% Mechanism: force on abducted/externally rotated shoulder Exam: Shoulder externally rotated Fullness anteriorly; acromion prominent post. Neurovascular testing Shoulder d/L: 7% incidence in young athletes Axillary neurapraxia in 33%; brachial plexus

24
Radiology of shoulder dislocations
AP and axillary views; optional scapular lateral (Y) Velpeau view Look for fractures (not a contra-indication to reduction) Always pre-reduction x-rays in primary cases Optional pre-reduction x-rays in recurrent cases Always post-reduction x-rays
 Velpeau view. Look for fractures (not a contra-indication to reduction) Always pre-reduction x-rays in primary cases. Optional pre-reduction x-rays in recurrent cases. Always post-reduction x-rays.")
25
Anterior shoulder dislocation

26
Anterior shoulder dislocation

27
Posterior shoulder dislocation

28
Hill-Sachs deformity

29
Bankart lesion

30
Shoulder dislocation reduction techniques
Types of maneuvers Traction (Stimson, self-reduction, Hippocrates, Eskimo,Milch) Scapular manipulation Leverage (Kocher) Combined maneuvers (slump, Snowbird)
 Scapular manipulation. Leverage (Kocher) Combined maneuvers (slump, Snowbird)")
31
The Stimson technique for anterior shoulder dislocation reduction.

32
J. Bone Joint Surg. Am., Dec 2009; 91: 2775 – 2782
The FARES method Significantly more effective, faster, and less painful method of reduction of an anterior shoulder dislocation in comparison with the Hippocratic and Kocher methods

34
Post-reduction treatment for shoulder dislocation
Ice 72 hrs, NSAID 7-14 days Immobilization 3-6 weeks Capsule needs time to heal Physical Therapy referral for rehab Less immobilization (1 week) and quicker rehab in pts >40 (to prevent stiffness) and in recurrent dislocators
 and quicker rehab in pts >40 (to prevent stiffness) and in recurrent dislocators.")
35
Indications for early orthopedic referral for pts with shoulder dislocation
Displaced greater tuberosity fxs (>1 cm post-reduction) Glenoid rim fxs displaced >5mm Irreducible dislocations (soft tissue interposition) Young athletes Immediate arthroscopic repair of Bankart lesions in athletes at West Point; reduced recurrence from 80% to <20%. Arciero et al. Arthroscopic Bankart repair versus non-operative treatment for acute, initial anterior shoulder dislocations. Am J Sports Med 1994; 22:
 Glenoid rim fxs displaced >5mm. Irreducible dislocations (soft tissue interposition) Young athletes. Immediate arthroscopic repair of Bankart lesions in athletes at West Point; reduced recurrence from 80% to <20%. Arciero et al. Arthroscopic Bankart repair versus non-operative treatment for acute, initial anterior shoulder dislocations. Am J Sports Med 1994; 22:")
36
Biceps Tendon Rupture Proximal rupture Most common in age > 60
Usually degenerative changes present initially Usually hear/feel snap Some may experience pain relief afterwards Popeye deformity Treatment nonoperative Unless young patient with traumatic rupture

37
Biceps Tendon Rupture Distal Biceps Rupture
Much less common (5% of biceps ruptures) Middle aged patients Usually tendonopathy/degenerative changes present which predispose Forceful, eccentric overload of the partially flexed elbow Up to 50% loss of supination power has been documented after rupture Treatment is surgical
 Middle aged patients. Usually tendonopathy/degenerative changes present which predispose. Forceful, eccentric overload of the partially flexed elbow. Up to 50% loss of supination power has been documented after rupture. Treatment is surgical.")
38
Biceps Tendon Rupture The Hook Test for Distal Biceps Tendon Avulsion Am J Sports Med November ; published online before print August 8, 2007

39
Does this happen in distal biceps rupture???

40
Elbow trauma Fractures Dislocations Ligament sprains
Look for compartment syndrome Rule out neurovascular injury

45
Axioms in elbow trauma radiograph evals
Look for fat pads signs (capsular effusion) Anterior fat pad (from coronoid fossa) may be normal; compare to other side Posterior fat pad (from olecranon fossa) is always abnormal Compare to x-rays of other side in children If elbow can’t be extended, obtain AP/lat of both humerus and forearm
 Anterior fat pad (from coronoid fossa) may be normal; compare to other side. Posterior fat pad (from olecranon fossa) is always abnormal. Compare to x-rays of other side in children. If elbow can’t be extended, obtain AP/lat of both humerus and forearm.")
47
Fat pad signs

48
Elbow fractures Supracondylar, epicondylar Radial head/neck Olecranon
Coronoid process **Consult current texts or your friendly local orthopedist for treatment of each.

49
Radial head/neck fractures
Common fracture in adults FOOSH usually Detection may require oblique view Assure proper alignment of head on capitellum (radiocapitellar line)
")
50
Radial head fracture types
Type I: less than 2 mm displacement Type II: angulated or >2 mm displaced Type III: comminuted Type I: less than 2 mm displacement Type II: Angulation or >2 mm displacement Type III: comminuted

51
Radiocapitellar line Radiocapitellar line should bisect radial head and intersect the center of the capitellum.

52
Radial head fracture

53
ER treatment of Radial head/neck fractures
Consider aspiration of hemarthrosis to relieve pain Type I Posterior splint a few days Sling; AROM when tolerated Physical therapy in 3 weeks Types II and III - splint and refer

55
Elbow Dislocations Defined by the direction of the forearm bones
80% posterolateral

56
Elbow Dislocations Treatment
Simple dislocations – no associated fracture 1 week immobilization Splint in 90 degrees flexion with forearm pronated Begin therapy/ROM Good long term results Complex dislocations – fracture present Surgery Radial head and neck 50-60% of time Instability within 30 degrees of full extension may be an indication for acute ligamentous repair. Lateral ligamentous complex is always repaired MCL if instability persists

57
Terrible Triad Elbow Injury
Elbow dislocation Fractures Radial head Coronoid process Treatment Ligamentous repair, ORIF of the coronoid, and either ORIF or prosthetic replacement of the radial head Persistent instability - hinged external fixator. The primary goal in all elbow dislocations is early motion

58
Perilunate Dislocations
Result from forced dorsiflexion, ulnar deviation, and supination of the wrist Approximately 25% missed in E.R. Emergent reduction and stabilization of these injuries are recommended

59
Perilunate Dislocations
Treatment Repair of ligamentous structures Percutaneous pinning Acute carpal tunnel syndrome may be present Necessitates release Late diagnosis associated with poor outcomes

60
Skier’s Thumb Sprain of ulnar collateral ligament of thumb MCP
Pathoanatomy Sprain of ulnar collateral ligament of thumb MCP Grades I, II, and III I = no laxity II = laxity but intact III = complete tear

61
Skier’s Thumb Forced abduction and hyperextension of thumb
Mechanism of injury Forced abduction and hyperextension of thumb FOOSH with thumb caught in extension Diagnosis History Radiographs Physical exam

62
Skier’s Thumb

63
Skier’s thumb: exam Anesthesia (block)
Valgus stress to MCPJ in extension Over 20° opening is probably grade III tear

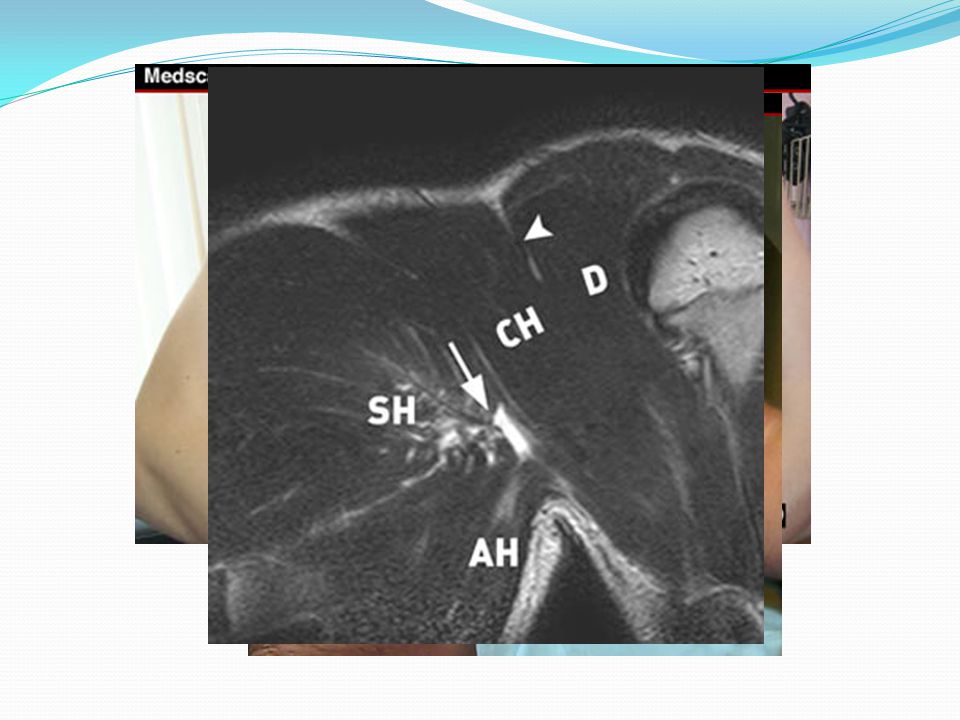
64
Skier’s Thumb Stener lesion 64% of Grade III injuries
Adductor aponeurosis interposed Prohibits reattachment of ligament MRI and arthrogram are sensitive

65
Stener Lesion

66
Skier’s Thumb: Treatment
Grades I & II Thumb spica splint 2-4 weeks, then Splint or tape 3 months Grade III Controversial Surgery Refer to Ortho

67
Scaphoid Fracture FOOSH Dull, deep, ache in radial side of wrist
History FOOSH Dull, deep, ache in radial side of wrist

68
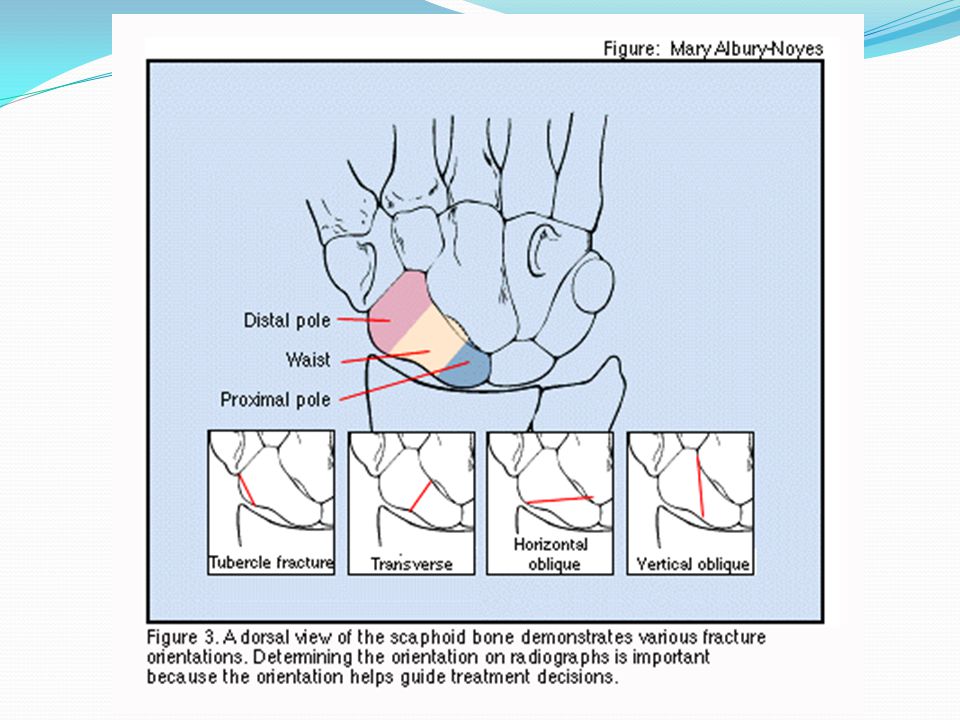
Scaphoid Fracture: Anatomy
Blood supplied from distal pole The more proximal the fracture, the greater the risk of avascular necrosis (AVN) or delayed union
 or delayed union.")
70
Scaphoid Fracture: Examination
Minimal swelling Tenderness in snuff box Pain with axial load

71
Scaphoid tubercle fracture

72
Scaphoid fracture: Radiographs
Lateral Oblique Scaphoid view **Normal plain films don’t rule out a scaphoid fracture

75
Scaphoid Fracture Treatment
Non-displaced fracture of waist or distal pole Long arm thumb spica cast 6 weeks Then, short arm thumb spica cast for 2-6 weeks Replace cast/get x-rays Q2 wks to assess healing

76
Scaphoid Fracture: Treatment (cont)
Clinically suspected fracture with normal plain films Treat as non-displaced fracture Short-arm thumb spica cast F/U in 10 days for repeat x-rays Consider bone scan/MRI if x-rays neg but fx suspected CT

77
Scaphoid Fracture: Referral criteria
Proximal fractures Angulated; displaced >1mm Scapholunate dissociation Presentation > 2 wks Early return to play necessary Non-union or AVN

78
Triangular Fibrocartilage Complex (TFCC) Tear
Mechanism of injury Fall on dorsiflexed and ulnar deviated wrist Axial load with forearm in hyperpronation Patient c/o ulnar sided wrist pain, swelling, loss of grip strength

79
TFCC Thickened pad of connective tissue that functions as a cushion for ulnar axial loads Articular disc Meniscus Ulnar collateral ligament

80
TFCC tear: Examination (cont)
Tenderness just distal to ulnar styloid

81
TFCC tear: Examination (cont)
Press test Patient presses arms of chair to lift body off seat 100% sensitive

82
TFCC tear: Examination (cont)
TFCC load test Pain = positive test

83
TFCC tear: Examination (cont)
Rule out injury to distal radio-ulnar joint (DRUJ) Squeeze radius/ulna together and passively rotate forearm Painful in DRUJ injury No pain in isolated TFCC tear
 Squeeze radius/ulna together and passively rotate forearm. Painful in DRUJ injury. No pain in isolated TFCC tear.")
84
TFCC Tear: Radiography
Plain films Positive ulnar variance (ulna 1-5 mm longer than radial articular surface) a/w TFCC tear Assess for fracture or ulnar subluxation MRI or Arthrography optional to confirm
 a/w TFCC tear. Assess for fracture or ulnar subluxation. MRI or Arthrography optional to confirm.")
85
MRI: TFCC tear

86
Long arm cast with forearm neutral for 4-6 weeks
TFCC Tear: Treatment Long arm cast with forearm neutral for 4-6 weeks Referral criteria: Associated injuries including DRUJ instability Persistent pain after immobilization

87
Jersey Finger Avulsion of the FDP tendon from its insertion
Ring finger most commonly affected Occurs with sudden hyperextension during finger flexion May be seen on plain x-ray Type I - retraction of tendon into palm Type II - retraction to PIP Type III - associated with a large, bony articular

88
Exam --Finger held in forced extension
--Tender along volar aspect of DIP --Unable to flex DIP

89
Jersey Finger Type I injuries must be repaired early (within 1 week) because of loss of blood supply to the tendon Splint in position Arthrodesis is generally favored over late (>3 months) repair due to finger stiffness after tendon grafting
 repair due to finger stiffness after tendon grafting.")
90
Mallet Finger Avulsion of the terminal extensor tendon
X-ray used to rule out fracture. Treated with prolonged (>6 weeks) extension splinting Results are almost uniformly good. Chronic injuries Swan-neck deformities due to chronic overpull of the extensor tendon at the PIP with flexion of the distal interphalangeal joint (DIP
 extension splinting. Results are almost uniformly good. Chronic injuries. Swan-neck deformities due to chronic overpull of the extensor tendon at the PIP with flexion of the distal interphalangeal joint (DIP.")
91
Mallet Finger

92
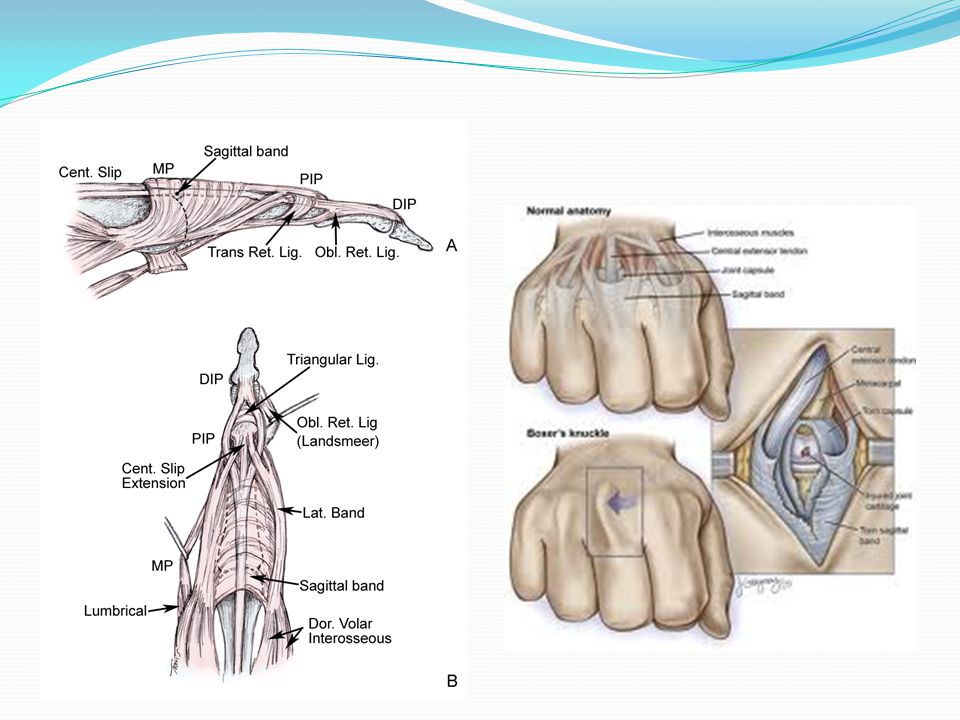
Sagittal Band Rupture “Boxer's knuckle”
Typically occurs in pugilists due to forceful subluxation of the extensor tendon Index and long fingers in professionals Ring and small fingers in amateurs Acute injuries are treated with extension splinting for 4 weeks Chronic injury will lead to persistent extensor tendon subluxation Repaired or reconstructed

94
QUESTIONS

Similar presentations





























![What am I?. What am I? Articulations of the humerus, radius, and ulna Articulations of the humerus, radius, and ulna. [ olecranon process ] Medial.](/14/4241906/big_thumb.jpg "What am I?. What am I? Articulations of the humerus, radius, and ulna Articulations of the humerus, radius, and ulna. [ olecranon process ] Medial.>")

