Download presentation
Presentation is loading. Please wait.

1
Dr Lawrence Siamuyoba Senior Registrar Department of Medicine/Haemato- oncology

2
Mechanisms: Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and further cellular hypoperfusion Clinical Manifestations: Multiple organ failure Hypotension

3
Hypovolemic Obstructive Cardiogenic Distributive Anaphylactic Septic

4
Hypovolemic: (classic shock) THE MOST COMMON CLASS. It is the standard used to compare other forms of shock to differentiate the diagnosis Hemorrhagic/Blood loss Dehydration/Fluid loss

6
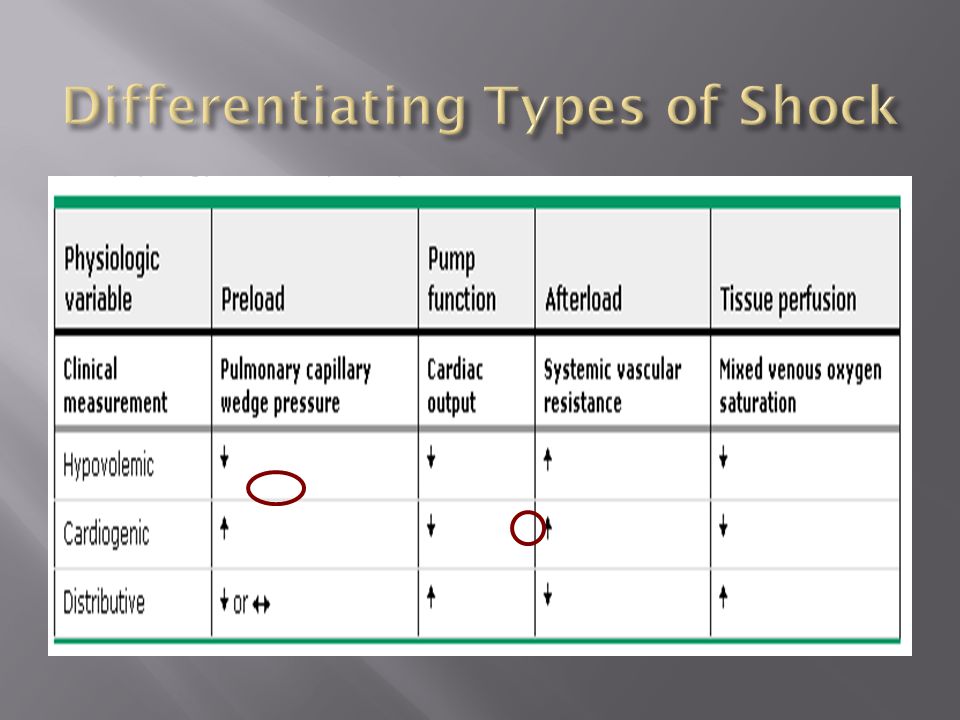
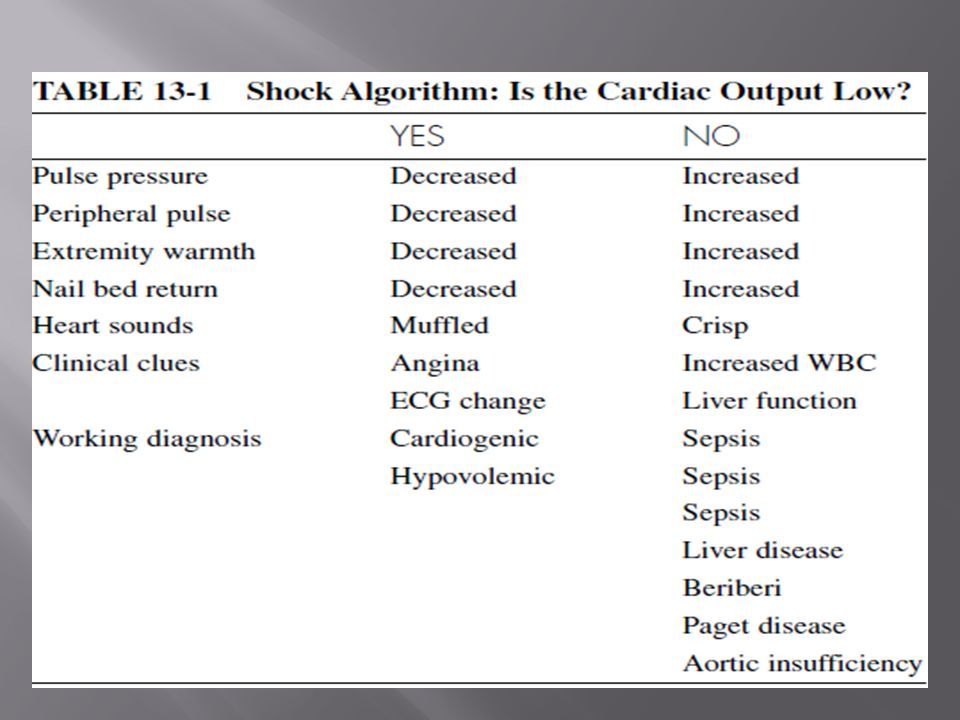
What type of shock is it? Step I: is the cardiac output reduced or elevated Septic shock is strongly suggested if High cardiac output hypotension Widened pulse pressure Strong apical impulse Fever or hypothermia Low cardiac output indicates cardiogenic or hypovolaemic shock Narrow pulse pressure Reduced apical impulse Cool extremities

7
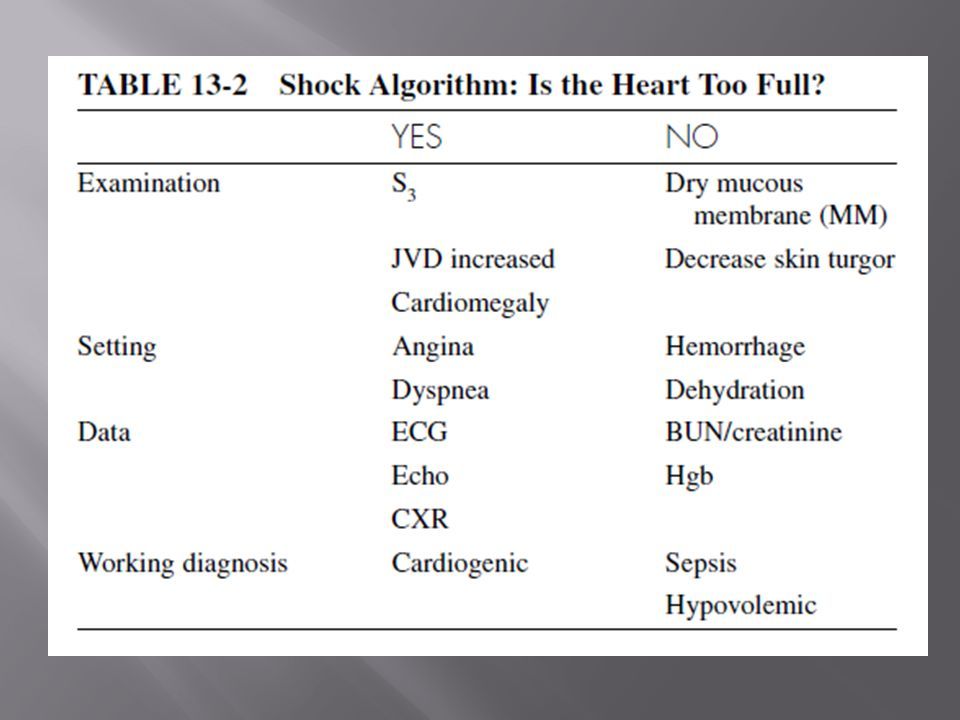
Step II: if the cardiac output is low, is the heart empty or full Cardiogenic shock Volume overload Findings include A large heart Murmurs Gallop rhythms JVP Hypovolaemic shock Obvious intravascular depletion Blood loss

10
Hemorrhage Severe diarrhea Vomiting Excessive perspiration Third Spacing Shift of fluid in severe burns can lead to hypovolemic shock Peritonitis Intestinal obstruction

11
Kidneys release antidiuretic hormone which increases vasoconstriction Signs and symptoms: Mental status: lethargy, sleepy, combative Skin: clammy, pale, mottling. Cyanosis around the nose and mouth first, spreads to extremities Blood pressure: begins to fall, capillary refill delayed Pulse: rapid and weak Respirations: rapid and shallow Other: decreased urination

12
Signs and symptoms: Mental status: decreased LOC, to unresponsive Skin: gray, mottled, cyanotic, waxen, sweating stops Blood pressure: decreases, becomes undetectable Pulse: slows then disappears Respiration: agonal Other: irritable heart, bradycardia, leads to asystole

13
Stop the fluid loss – direct pressure, surgery Replace fluids – blood and blood products, plasma expanders, crystalloid fluids (provide H2O replacement and E-lytes), Colloids (albumin, FF) Pneumatic antishock garments Use low dose inotropics
, Colloids (albumin, FF) Pneumatic antishock garments Use low dose inotropics")
14
Systemic hypoperfusion secondary to severe depression of cardiac output and sustained systolic arterial hypotension despite elevated filling pressures.

15
Heart pump failure (40% of myocardium damaged by an MI) Cardiac trauma Cardiomyopathy Congestive heart failure Cardiac dysrhythmias
 Cardiac trauma Cardiomyopathy Congestive heart failure Cardiac dysrhythmias")
16
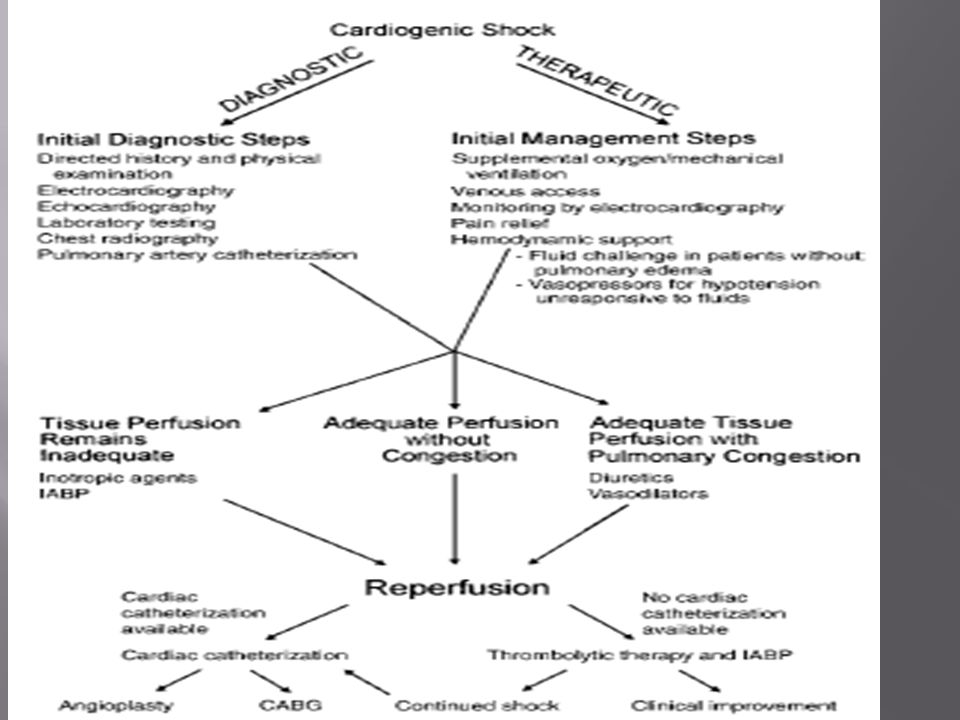
Etiologies Pathophysiology Clinical/Hemodynamic Characteristics Treatment Options

17
Acute myocardial infarction/ischemia LV failure VSR Papillary muscle/chordal rupture- severe MR Ventricular free wall rupture with subacute tamponade Other conditions complicating large MIs Hemorrhage Infection Excess negative inotropic or vasodilator medications Prior valvular heart disease Hyperglycemia/ketoacidosis Post-cardiac arrest Post-cardiotomy Refractory sustained tachyarrhythmias Acute fulminant myocarditis End-stage cardiomyopathyHypertrophic cardiomyopathy with severe outflow obstruction Aortic dissection with aortic insufficiency or tamponade Pulmonary embolu Severe valvular heart disease - Critical aortic or mitral stenosis, Acute severe aortic or MR

20
Drop in cardiac output Skin: cyanosis Pulse: bradycardia, tachycardia, or within normal limits Respirations: diminishing breath sounds progressing to wheezing and crackles. Patient complains of increasing dyspnea. Coughs white or pink tinged foamy sputum Other: pulmonary edema and left heart failure Pitting edema+ right heart failure

21
Massive pulmonary embolism Acute dissecting aneurism of the aorta Acute cardiac tamponade Acute hemorrhage Cerebrovascular thrombosis Diabetic acidosis Acute pancreatitis Acute adrenal insufficiency

23
The priority in treatment of cardiogenic shock is to expand the circulating blood volume with IV fluids-using PWP or CVP as a basic guide.

24
1. Position the patient 2. Make certain that there is adequate airway 3. Mainatain adequate oxygenation 4. Start an IV infusion of 5% Dextrose Water using 5. Insert CVP or swan-Ganz catheter into the pulmonary artery 6. Draw the necessary blood samples 7. Insert urinary catheter for purposes of obtaining adequate measurement of the urine output. 8. Monitor patient continuously 9. Relieve any pain 10. Relieve any agitation 11. Take portable Chest X-rays

25
Hemodynamic monitoring IV fluids Intra-aortic balloon pump Cardiac transplant Inotropics/cardiotonics Digoxin, Amrinone, Primacor Vasodilators Diuretics If from obstructive may need surgical repair, chest tube, pacemaker, needle aspiration of fluid

26
Can be classed as a type of cardiogenic shock Pulmonary embolism/Blocked pulmonary circulation Tension pneumothorax/Increased intrathoracic pressure Cardiac tamponade/Pressure on myocardium. Decreased preload

27
Mental status : anxiety, feeling of impending doom Skin : pallor to cyanosis around the mouth and the nose Other : chest pain, lung sounds may be clear, possible syncope, cardiac dysrhythmias can lead to sudden cardiac arrest

28
Anaphylactic Shock Mechanism: severe allergic reaction Skin: hives, possible petechia. Urticaria, pallor, cyanosis Blood pressure: abrupt fall in cardiac output Respiration: rapid shallow, dyspnea with stridor, wheezes, crackles, leading to respiratory arrest Other: swelling of mucus membranes/pulmonary edema

29
Maintain airway Ice to site of injection or sting Gastric lavage Isotonic IV fluids – D5W, NACL, LR Epinephrine and theophylline Antihistamines (H2 blockers) Steroids Vasopressors to constrict blood vessels and raise BP
 Steroids Vasopressors to constrict blood vessels and raise BP")
30
Mechanism: overwhelming infection Skin: varies form flushed pink (if fever is present) to pale and cyanotic. Purple blotches possible, peeling skin, general or on palms and soles of feet Blood pressure: early—cardiac output increases but toxins prevent increase in BP. Late --- drop in BP, hypotension Respiratory: dyspnea with altered lung sounds Other: high fever, (except in elderly and very young), Late sign is pulmonary edema
, Late sign is pulmonary edema.")
31
C & S for infective site IV fluids with NS Medications and other treatment Vancomycin Penicillin Cephalosporin Cardiotonics and inotropics Vasopressors Heparin Blood products

32
Remember your ABC’s Administer airway 100% O2 via a non- re-breather mask Assist ventilations if necessary Position patient to assist perfusion Keep patient warm Perform focused assessment Monitor and adjust O2, gain IV access, cardiac monitor, pulse oximetry Fluid replacement of LR or NS Need 3 liter of fluid to replace I liter of blood loss Apply pressure to IV or blood to facilitate faster infusion

33
Ineffective Tissue Perfusion Decreased Cardiac Output Anxiety Fluid Volume Deficit Risk for Injury Risk for Infection

34
Defined as when generalized inflammation occurs and threatens vital organs Causes: multiply transfusions, massive tissue injury, burns, and pancreatitis, severe infections or sepsis Effects: endothelium is damaged and allows fluid to leak into the body tissues, results in poor perfusion of blood to organs Body is in a hypermetabolic state

35
Diagnosis made when 2 or more of the following are seen: Temperature less than 97 or greater than 100.4 Heart rate more than 90 Respiratory rate more than 20 or PaCO2 less than 32mm Hg WBC count less than 4000 cells or more than 12,000 Sepsis is used if patient has SIRS with and infection

36
Defined: when 2 or more organ systems are failing at one time Is caused by the immune system’s uncontrolled response to severe illness or injury Common cause of death of patients in the ICU, with mortality of 50% Identifying and acting quickly can help survival Can develop quickly following surgery, trauma, or severe burns or slowly in the case of an infection

37
Critical care nursing Goals Prevent and treat infections Maintain tissue oxygenation Provide nutritional and metabolic response Support failing organs

Similar presentations
















 leading to inadequate oxygen delivery to tissues.>")


 The McGraw-Hill Companies, Inc. Permission required for reproduction or display.>")
