Download presentation
Presentation is loading. Please wait.

1
SHOCK

2
DEFINITION Profound hemodyamic and metabolic disturbance characterized by failure of the circulatory system to maintain adequate perfusion of vital organs

3
Types of Shock Cardiogenic (intracardiac vs extracardiac) Hypovolemic
Distributive sepsis**** neurogenic (spinal shock) adrenal insufficiency anaphylaxis
 adrenal insufficiency. anaphylaxis.")
5
Cardiogenic Shock, intracardiac
Myocardial Injury or Obstruction to Flow Arrythymias valvular lesions AMI Severe CHF VSD Hypertrophic Cardiomyopathy

6
Presentation of Cardiogenic Shock
Pulmonary Edema JVD hypotensive weak pulses oliguria

7
Cardiogenic Shock, extracardiac (Obstructive)
Pulmonary Embolism Cardiac Tamponade Tension Pneumothorax Presentation will be according to underlying disease process.

8
Hypovolemic Shock Reduced circulating blood volume with secondary decreased cardiac output Acute hemorrhage Vomiting/Diarrhea Dehydration Burns Peritonitis/Pancreatitis

9
Presentation of Hypovolemic Shock
Hypotensive flat neck veins clear lungs cool, cyanotic extremities evidence of bleeding? Anticoagulant use trauma, bruising oliguria

10
Distributive Shock Peripheral Vasodilation secondary to disruption of cellular metabolism by the effects of inflammatory mediators. Gram negative or other overwhelming infection. Results in decreased Peripheral Vascular Resistance.

11
Distributive Shock: Presentation
Febrile Tachycardic clear lungs, evidence of pneumonia warm extremities flat neck veins oliguria

12
Diagnosing Shock Response to fluids Echo/EKG CXR Evidence of infection
Swan-Ganz Catheter?

13
Swan-Ganz Catheter Utilized to differentiate types of shock and assist in treatment response. Probably overused by physicians. Studies documenting increased mortality in patients with catheters versus no catheters, although somewhat swayed by selection bias.

14
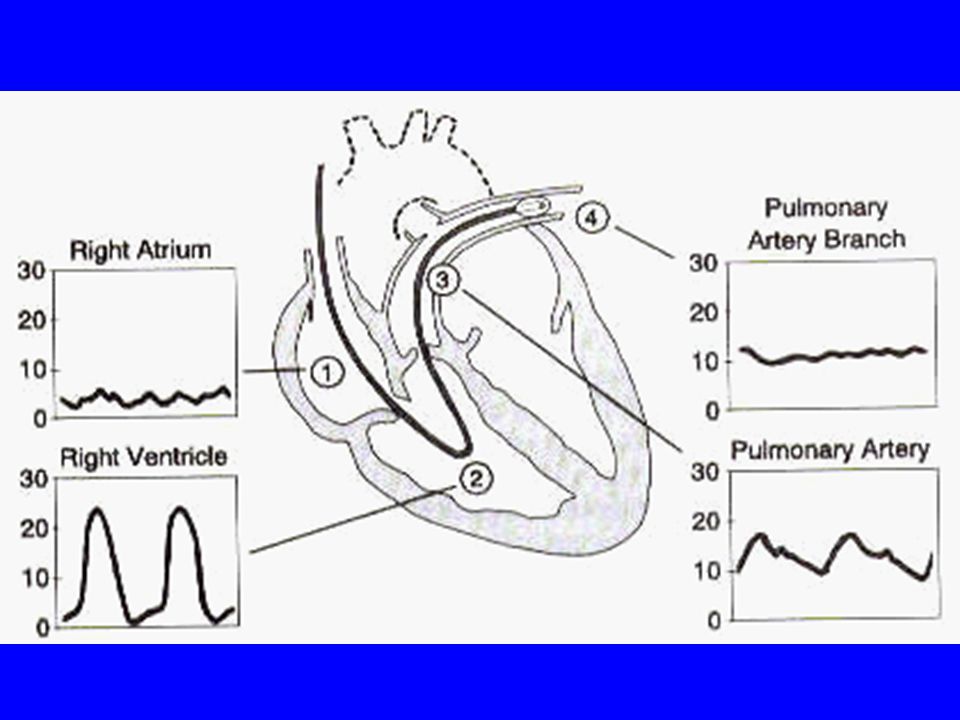
Swan-Ganz Catheter

16
Swan-Ganz Interpretation

17
Management Correct underlying disorder if possible and then direct efforts at increasing the blood pressure to increase oxygen delivery to the tissues. Maintain a mean arterial pressure of 60 (1/3 systolic + 2/3 diastolic) Keep O2 sats >92%, intubate if neccesary
 Keep O2 sats >92%, intubate if neccesary.")
18
Correction of hypotension
Normal Saline should be administered anytime a patient is hypotensive. If hypotension exists give more NS. *** If possible give blood as it replaces colloid. Vasopressors Inotropic agents for cardiogenic shock Intra-aortic Balloon Pump for cardiogenic

19
Autonomic Drugs in Shock

20
Management of Cardiogenic Shock
Attempt to correct problem and increase cardiac output by diuresing and providing inotropic support. IABP is utilized if medical therapy is ineffective. Catheterization if ongoing ischemia Cardiogenic shock is the exception to the rule that NS is always given for hypotension NS will exacerbate cardiac shock.

21
Intra-Aortic Balloon Pump

22
Management of Septic Shock
Early goal directed therapy Identification of source of infection Broad Spectrum Antibiotics IV fluids Vasopressors Steroids ?? Recombinant human activated protein C ( Xygris) Bicarbonate if pH < 7.1
 Bicarbonate if pH < 7.1.")
23
Management of Hypovolemic Shock
Correct bleeding abnormality If PT or PTT elevated then FFP Aggressive Fluid replacement with 2 large bore IV’s or central line. Pressors are last line, but commonly required.

24
Addison’s Disease Deficiency of cortisol and aldosterone production in the adrenal glands This is suspected when patient is non-responsive to fluids and antibiotics. Electrolytes may reveal hyponatremia and hyperkalemia Hydrocortisone 100 mg IV immediately then taper appropriately

Similar presentations