Download presentation
Presentation is loading. Please wait.

1
Coding 101-Pressure Ulcers, Debridement and other Skin related injuries.

2
What is a Pressure Ulcer? A localized injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear and/or friction.A localized injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear and/or friction.

3
Pressure Stops blood flow

4
Shearing Caused by gravity and frictionCaused by gravity and friction Decreases or stops blood flow through the vesselsDecreases or stops blood flow through the vessels

5
Friction Occurs when two surfaces rub togetherOccurs when two surfaces rub together Common sitesCommon sites - Elbow - Heels

6
Stage I Intact skin with non-blanchable redness of a localized area usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its color may differ from the surrounding area.Intact skin with non-blanchable redness of a localized area usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its color may differ from the surrounding area.

7
Translation The skin is not broken or open- it is red or darker pigmented and does not lighten or turn white when pressed on. It is hard to detect on patients with dark skin tones.The skin is not broken or open- it is red or darker pigmented and does not lighten or turn white when pressed on. It is hard to detect on patients with dark skin tones. Many times reactive hyperemia is mistaken for a Stage I ulcer.Many times reactive hyperemia is mistaken for a Stage I ulcer. If truly a Stage I, this indicates that the patient is at high risk for pressure ulcer formation.If truly a Stage I, this indicates that the patient is at high risk for pressure ulcer formation.

8
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open/ruptured serum- filled blister.Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open/ruptured serum- filled blister.

9
Translation The ulcer is red, pink, moist, shiny or dry and shallow. If yellow or bruising is noted in the wound base, the ulcer is a higher stage.The ulcer is red, pink, moist, shiny or dry and shallow. If yellow or bruising is noted in the wound base, the ulcer is a higher stage. Clinicians often mistake incontinence related skin loss, tape burns, and skin tears as stage II ulcers. These are considered partial thickness wounds - NOT pressure ulcers.Clinicians often mistake incontinence related skin loss, tape burns, and skin tears as stage II ulcers. These are considered partial thickness wounds - NOT pressure ulcers. Bruising in wound base of ? Stage II indicates suspected deep tissue injury.Bruising in wound base of ? Stage II indicates suspected deep tissue injury.

10
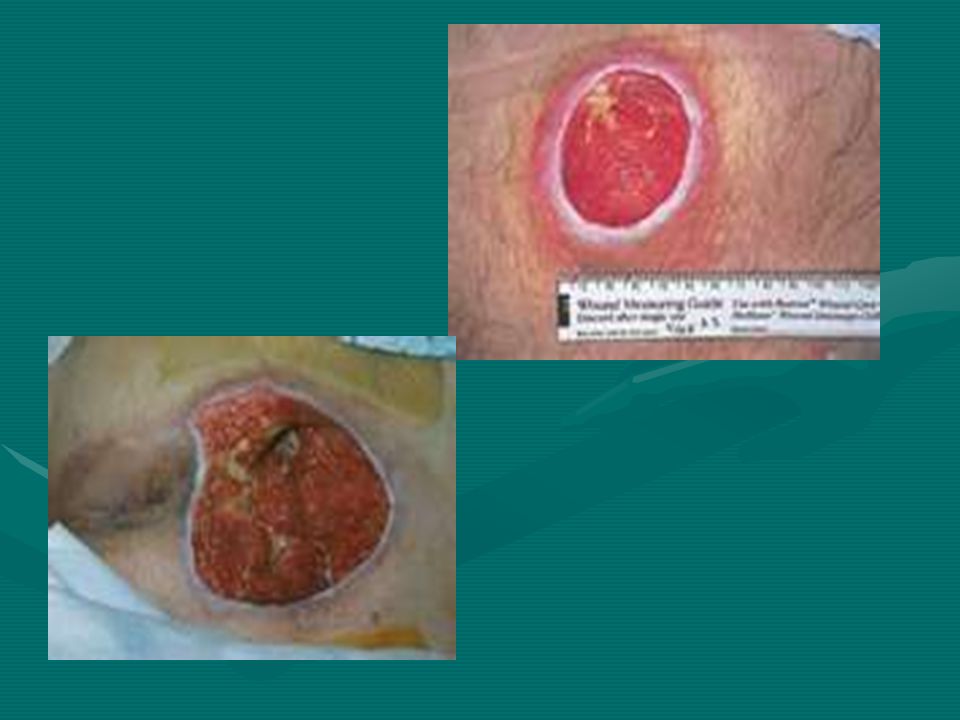
Stage III Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon, or muscle are not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling. Bone/tendon is not visible or directly palpable.Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon, or muscle are not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling. Bone/tendon is not visible or directly palpable.

12
Translation The depth of a Stage III ulcer varies by anatomical location.The depth of a Stage III ulcer varies by anatomical location. Areas of the body with little to no subcutaneous tissue can have a very shallow Stage III (example-ears, nose, ankle, back of the head)Areas of the body with little to no subcutaneous tissue can have a very shallow Stage III (example-ears, nose, ankle, back of the head) Areas of the body with significant adipose tissue can develop very deep Stage III ulcers and still not reveal tendon or bone.Areas of the body with significant adipose tissue can develop very deep Stage III ulcers and still not reveal tendon or bone.
Areas of the body with little to no subcutaneous tissue can have a very shallow Stage III (example-ears, nose, ankle, back of the head) Areas of the body with significant adipose tissue can develop very deep Stage III ulcers and still not reveal tendon or bone.Areas of the body with significant adipose tissue can develop very deep Stage III ulcers and still not reveal tendon or bone..")
13
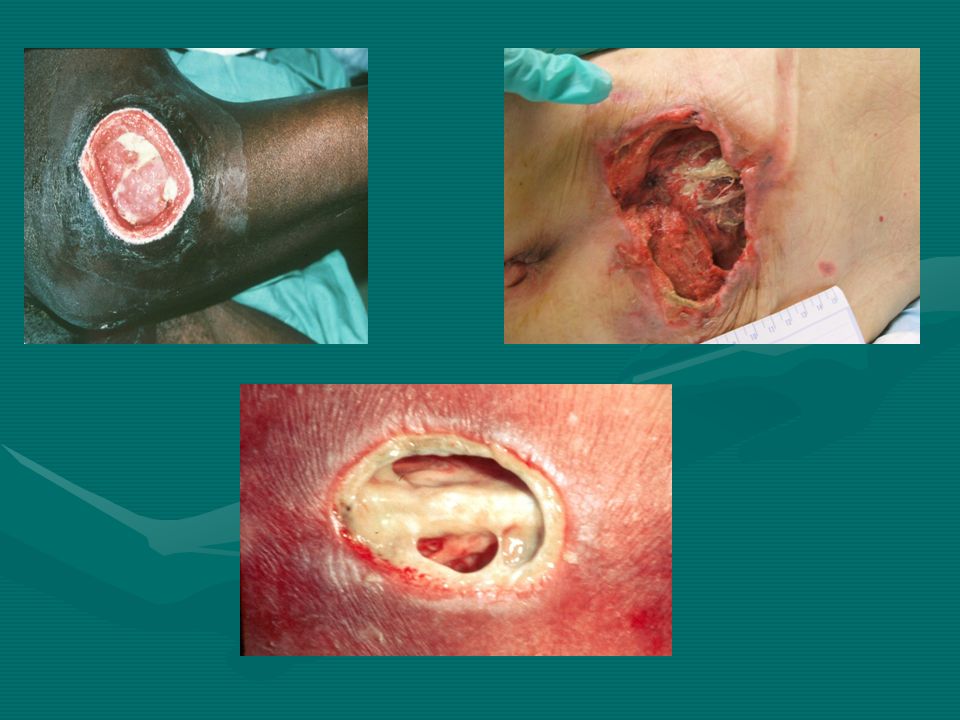
Stage IV Full thickness tissue loss with exposed bone, tendon, or muscle. Slough or eschar may be present on some parts of the wound bed. Often include undermining and tunneling. Exposed bone/tendon is visible or directly palpable.Full thickness tissue loss with exposed bone, tendon, or muscle. Slough or eschar may be present on some parts of the wound bed. Often include undermining and tunneling. Exposed bone/tendon is visible or directly palpable.

15
Translation The depth of Stage IV varies by anatomical location. (same as stage III)The depth of Stage IV varies by anatomical location. (same as stage III) If bone is visible in the wound bed, 99.9% chance of osteomyelitis being present!If bone is visible in the wound bed, 99.9% chance of osteomyelitis being present!
The depth of Stage IV varies by anatomical location. (same as stage III) If bone is visible in the wound bed, 99.9% chance of osteomyelitis being present!If bone is visible in the wound bed, 99.9% chance of osteomyelitis being present!.")
16
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green, or brown) and/or eschar (tan, brown, or black) in the wound bed.Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green, or brown) and/or eschar (tan, brown, or black) in the wound bed.
 and/or eschar (tan, brown, or black) in the wound bed.Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green, or brown) and/or eschar (tan, brown, or black) in the wound bed.")
17
Translation Once the eschar or non-viable tissue is debrided, the ulcer will be a Stage III or IV pressure ulcer.Once the eschar or non-viable tissue is debrided, the ulcer will be a Stage III or IV pressure ulcer. Not all eschars should be removed—AHCPR Guidelines state that an intact stable/dry eschar on the heel of the bedridden patient or the patient with compromised blood flow should be left alone. Continued pressure relief and reducing the chance for infection would be the goal.Not all eschars should be removed—AHCPR Guidelines state that an intact stable/dry eschar on the heel of the bedridden patient or the patient with compromised blood flow should be left alone. Continued pressure relief and reducing the chance for infection would be the goal.

18
Suspected Deep Tissue Injury (DTI) Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue.Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue.

20
Translation The DTI category was added to define the ulcers that have been seen over the years by clinicians. These pressure related skin injuries will rapidly progress to eschar/dead tissue regardless of care given.The DTI category was added to define the ulcers that have been seen over the years by clinicians. These pressure related skin injuries will rapidly progress to eschar/dead tissue regardless of care given. A DTI usually will evolve into an eschar (which would be a stage III or IV skin injury) despite the addition of pressure relieving interventions. However, clinicians have seen that some DTI’s will resolve. On going research to identify why this may occur is necessary.A DTI usually will evolve into an eschar (which would be a stage III or IV skin injury) despite the addition of pressure relieving interventions. However, clinicians have seen that some DTI’s will resolve. On going research to identify why this may occur is necessary.
 despite the addition of pressure relieving interventions. However, clinicians have seen that some DTI’s will resolve. On going research to identify why this may occur is necessary.A DTI usually will evolve into an eschar (which would be a stage III or IV skin injury) despite the addition of pressure relieving interventions. However, clinicians have seen that some DTI’s will resolve. On going research to identify why this may occur is necessary..")
21
What is slough/eschar? Both are nonviable tissue that is adhered to the wound bed. Usually the goal is to remove this as soon as possible so healing can begin.Both are nonviable tissue that is adhered to the wound bed. Usually the goal is to remove this as soon as possible so healing can begin.

22
What do they mean by a granulating or a healing full thickness wound? The wound at some point was a stage III or IV and now is in the healing stage—if the wound was not seen by the clinician at the beginning of this process, the clinician can not tell which stage it had been.The wound at some point was a stage III or IV and now is in the healing stage—if the wound was not seen by the clinician at the beginning of this process, the clinician can not tell which stage it had been.

23
Hospital acquired pressure ulcers are a national concern due to patient morbidity, treatment cost, and reimbursement issues. Are your facility Coders, Wound Care Team, and Providers talking and working together?Are your facility Coders, Wound Care Team, and Providers talking and working together? What can be done to help increase a team approach to assure accuracy of coding?What can be done to help increase a team approach to assure accuracy of coding?

24
Tips for Coding Pressure Ulcers The provider has the responsibility to resolve inconsistent, missing or conflicting documentation issues. The coder should query the provider when the documentation is insufficient to assign a specific code.The provider has the responsibility to resolve inconsistent, missing or conflicting documentation issues. The coder should query the provider when the documentation is insufficient to assign a specific code. As long as the diagnosis of a pressure ulcer is made by the provider, the stage can be obtained from the documentation of other clinicians, such as the bedside nurse, the wound care nurse or the physical therapist.As long as the diagnosis of a pressure ulcer is made by the provider, the stage can be obtained from the documentation of other clinicians, such as the bedside nurse, the wound care nurse or the physical therapist.

25
The coder should first classify the type of wound as either traumatic or nontraumatic.The coder should first classify the type of wound as either traumatic or nontraumatic. Nontraumatic wounds can then be categorized as a pressure ulcer, nonhealing chronic ulcer or nonhealing surgical wound.Nontraumatic wounds can then be categorized as a pressure ulcer, nonhealing chronic ulcer or nonhealing surgical wound. Only pressure ulcers will need a 2 code sets – one for site/location and one for stage.Only pressure ulcers will need a 2 code sets – one for site/location and one for stage.

26
Some pressure ulcer cannot be staged because the depth of the wound is obscured by dead/nonviable tissue. The stage of these ulcers will need to be updated when and if debridement completed.

27
ICD-9-CM Coding Issues Only the first 8 secondary diagnosis codes will be captured in the Medicare data system.Only the first 8 secondary diagnosis codes will be captured in the Medicare data system. There is no requirement that the corresponding stage code be in the first 8 secondary diagnosis codes.There is no requirement that the corresponding stage code be in the first 8 secondary diagnosis codes. The above leads to under reporting of both HAC or POA pressure ulcersThe above leads to under reporting of both HAC or POA pressure ulcers

28
Debridement and Coding TypesTypes –Excisional-the sharp removal of tissue at the wound margin or at the base until viable tissue is removed. Debridement codes are based on the deepest layer of viable tissue removed. –Selective-the removal of nonviable tissue. The physician removes no viable tissue. –Non-selective- the gradual removal of nonviable tissue, not usually provided by physician.

29
Excisional Debridement Documentation must include one of the following to code this type debridement.Documentation must include one of the following to code this type debridement. –Bleeding tissue –Removal of viable tissue ( “down to and including”) –Increasing wound size by width, length or depth –Must be described as “excisional” not “sharp” and include type instrument used (scalpel)and technique used (snipping/cutting)
 –Increasing wound size by width, length or depth –Must be described as excisional not sharp and include type instrument used (scalpel)and technique used (snipping/cutting).")
30
Selective Debridement To code for this type debridement documentation must include the following elements.To code for this type debridement documentation must include the following elements. –Location and characteristic of lesion –Depth –Type of tissue removed (nonviable) –Instrument used (sharp) –Patient’s tolerance –Dressings applied and treatment plan
 –Instrument used (sharp) –Patient’s tolerance –Dressings applied and treatment plan.")
31
Non-selective Debridement This would include autolytic, enzymatic, chemical, mechanical debridement provided by topical dressings.This would include autolytic, enzymatic, chemical, mechanical debridement provided by topical dressings. These treatments are provided by the bedside nurse, wound care team and or physical therapist.These treatments are provided by the bedside nurse, wound care team and or physical therapist.

32
Reimbursement is essential for financial success of our facilities. Providers need to work as a team with the coders to assure proper documentation to receive the reimbursement they deserve!

33
Questions?

34
References/Resources http://www.npuap.orghttp://www.npuap.orghttp://www.npuap.org http://www.wocn.orghttp://www.wocn.orghttp://www.wocn.org http://www.nursingquality.orghttp://www.nursingquality.orghttp://www.nursingquality.org http://www.ihi.orghttp://www.ihi.orghttp://www.ihi.org http://www.5millionlives.premierinc.comhttp://www.5millionlives.premierinc.comhttp://www.5millionlives.premierinc.com

Similar presentations

>")
 for Pressure Ulcers>")













 A pressure ulcer is localized injury to the skin and/or underlying.>")



