Download presentation
Presentation is loading. Please wait.

1
Heather Tucker RN, MSN, APRN, FNP-BC, CWS

2
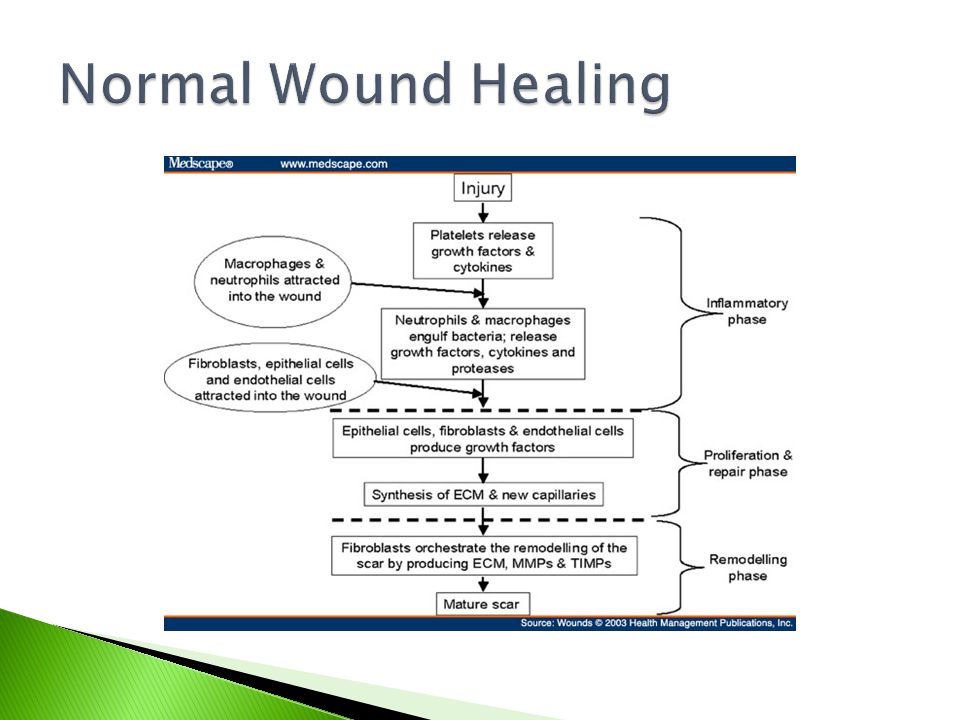
Objectives ◦ Discuss normal wound healing ◦ Discuss the major wound classifications of chronic wounds and how to differentiate ◦ Discuss how to describe wounds ◦ Discuss treatment options for chronic wounds

4
Ischemic Venous Lymphedema Diabetic Pressure

5
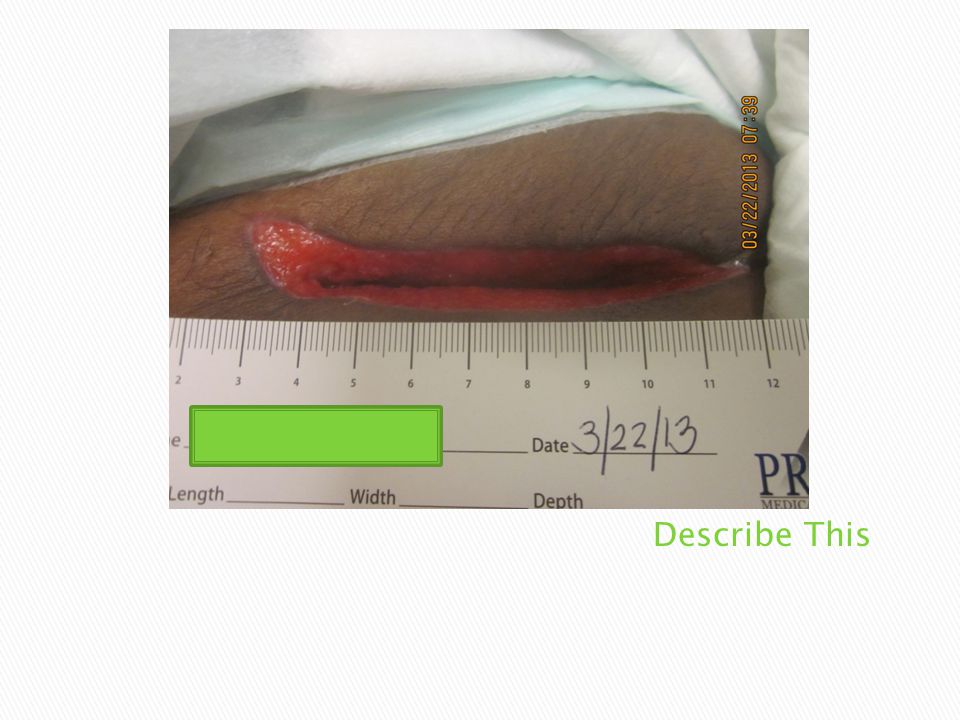
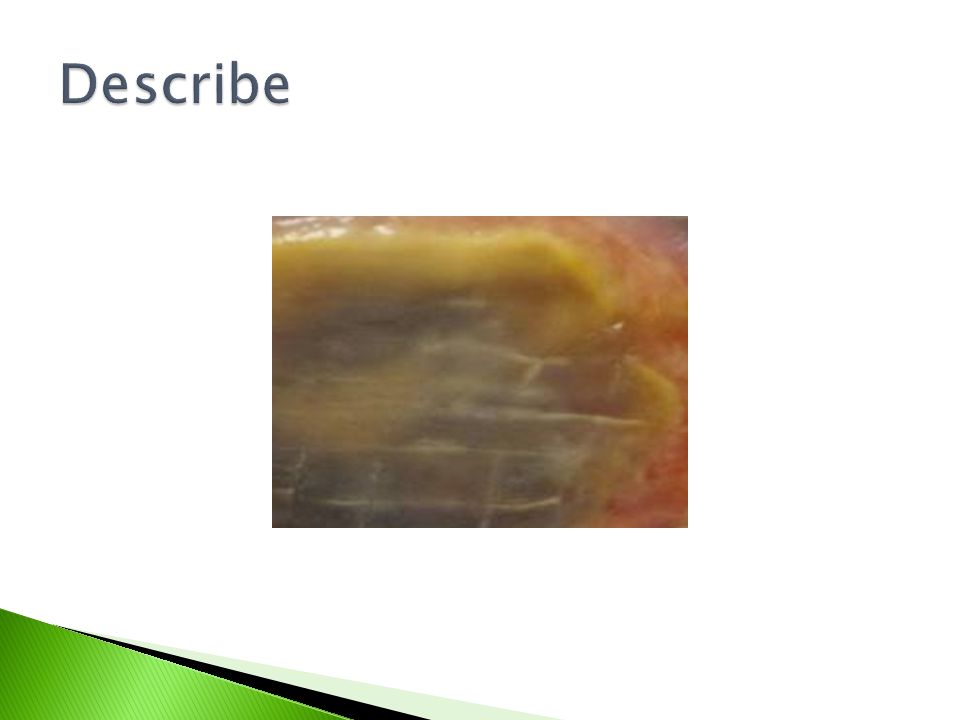
Measurement ◦ Length, width, depth, undermining, tunneling Appearance ◦ Slough, fibrin, eschar Drainage ◦ Mild, moderate, large, serosang, bloody, purulent, serous Exposed Structures ◦ Do you see bone, muscle, tendon, ligament

12
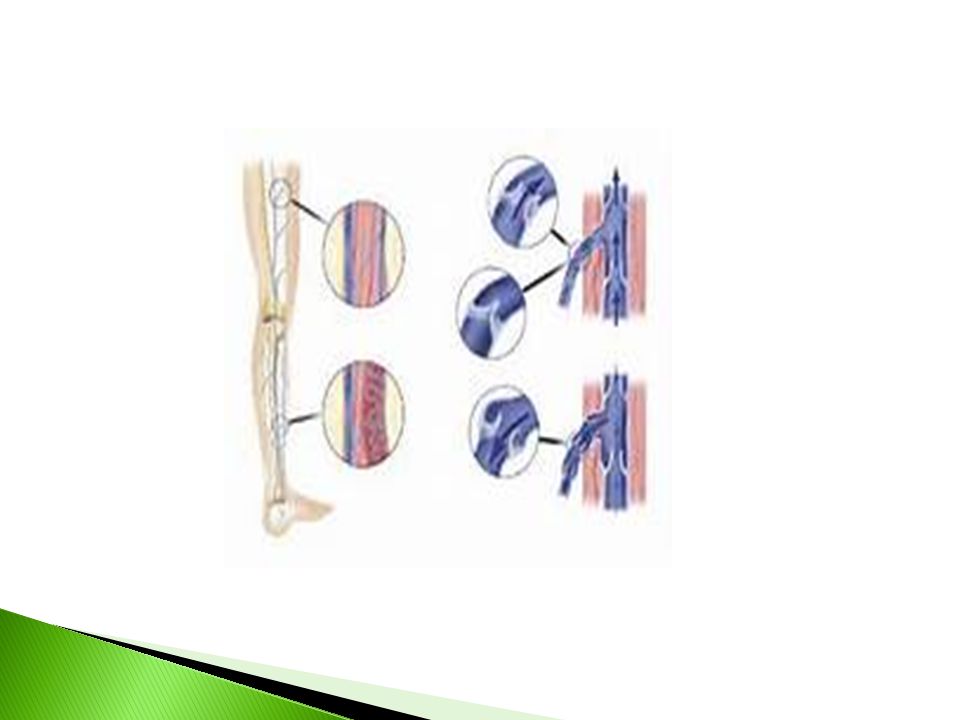
Always assess pulses with lower extremity wounds ◦ If DP and/or PT pulses not palpable or dopplerable- strongly suspect arterial ◦ ABI should be done on all lower extremity wounds ◦ Arterial wounds usually distal on extremities ◦ Usually dry and can have gangrene or eschar ◦ Common with diabetic and smokers ◦ Punched out appearance, well defined even wound margins Palmquist RA, Shimahara L, Donayre CE. Diagnosis and Management of Vascular Ulcers. In Sussman C, Bates-Jensen B, eds. Wound Care: A Collaborative Practice Manual for Health Professionals. Baltimor, MD: Lipincott Williams & Wilkins;

13
Pts may complain of intermittent claudication Pain on elevation Dependent Rubor Very painful unless the occur in presence of neuropathy Palmquist RA, Shimahara L, Donayre CE. Diagnosis and Management of Vascular Ulcers. In Sussman C, Bates-Jensen B, eds. Wound Care: A Collaborative Practice Manual for Health Professionals. Baltimor, MD: Lipincott Williams & Wilkins; 2007:405-420

16
Caused by incompetent veins Usually on Gaiter area of leg/foot Leg does not have to be grossly edematous Hemosideran staining Compression therapy is the cornerstone of wound healing ◦ If not ischemic, should use 30-40mmHg Elevation of extremity above the heart 2 -3 times a day Palmquist RA, Shimahara L, Donayre CE. Diagnosis and Management of Vascular Ulcers. In Sussman C, Bates-Jensen B, eds. Wound Care: A Collaborative Practice Manual for Health Professionals. Baltimore, MD: Lipincott Williams & Wilkins; 2007:405-420

17
Unna’s Boot 4 layer vs 3 layer compression wrap Juxta-Lite™ Circaid ™ Setopress ™ Surepress ™

20
Should be wrapped from base of toes to 3 fingers below back of knee in an upward fashion

23
Causes ◦ Lymph node resection ◦ Obesity ◦ Long standing venous insufficiency ◦ Infection filariasis

26
Treatment ◦ Manual lymph massage ◦ Lymphedema wraps ◦ Lymphedema pumps

27
Diabetes Spina Bifida Hansen’s disease Systemic erythematosus lupus AIDS/HIV Cancer MS Vitamin B def Quad/Paraplegic Elftman N, Conlan JE. Management of the Neuropathic Foot. In Sussman C, Bates-Jensen B, eds. Wound Care: A Collaborative Practice Manual for Health Professionals. Baltimore, MD: Lipincott Williams & Wilkins; 2007:421-462

28
Neuropathy- Basically Pressure Ulcers ◦ Semmes Weinstein Sensation test High Glycohemoglobin A1C ◦ >7 Always culture ◦ GOLD STANDARD TISSUE CX Offloading is the key to healing ◦ Total contact cast TCC-EZ™ Boot ◦ Heel/Forefoot offloading boot Elftman N, Conlan JE. Management of the Neuropathic Foot. In Sussman C, Bates-Jensen B, eds. Wound Care: A Collaborative Practice Manual for Health Professionals. Baltimore, MD: Lipincott Williams & Wilkins; 2007:421- 462

29
OFFLOADING

30
Offload ◦ Certain stages will qualify for certain offloading devices ◦ Examples air, gel or foam cushions for wc for wheelchairs and gel/foam or air mattress for beds Temperpedic not an offloading mattress ◦ Do not use bunny boots for offloading heels-if ulcer needs more offloading such as Prevalon ™ or Heelift ™

31
Category/Stage I: Non-blanchable erythema Intact skin with non-blanchable redness of a localized area usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its color may differ from the surrounding area. The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue. Category I may be difficult to detect in individuals with dark skin tones. May indicate “at risk” persons. Category/Stage II: Partial thickness Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open/ruptured serum-filled or sero- sanginous filled blister.Presents as a shiny or dry shallow ulcer without slough or bruising*. This category should not be used to describe skin tears, tape burns, incontinence associated dermatitis, maceration or excoriation. *Bruising indicates deep tissue injury. NPUAP Staging Report. 2007. National Pressure Ulcer Advisory Panel (NPUAP). www.npuap.org. http://www.npuap.org/resources/educational-and-clinical-resources/npuap-pressure-ulcer-stagescategories/. Accessed 2/14/2013www.npuap.org http://www.npuap.org/resources/educational-and-clinical-resources/npuap-pressure-ulcer-stagescategories/
. Accessed 2/14/2013www.npuap.org")
34
Category/Stage III: Full thickness skin loss Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling. The depth of a Category/Stage III pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have (adipose) subcutaneous tissue and Category/Stage III ulcers can be shallow. In contrast, areas of significant adiposity can develop extremely deep Category/Stage III pressure ulcers. Bone/tendon is not visible or directly palpable. Category/Stage IV: Full thickness tissue loss Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present. Often includes undermining and tunneling. The depth of a Category/Stage IV pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have (adipose) subcutaneous tissue and these ulcers can be shallow. Category/Stage IV ulcers can extend into muscle and/or supporting structures (e.g., fascia, tendon or joint capsule) making osteomyelitis or osteitis likely to occur. Exposed bone/muscle is visible or directly palpable. NPUAP Staging Report. 2007. National Pressure Ulcer Advisory Panel (NPUAP). www.npuap.org. http://www.npuap.org/resources/educational-and-clinical-resources/npuap-pressure-ulcer- stagescategories/. Accessed 2/14/2013www.npuap.org http://www.npuap.org/resources/educational-and-clinical-resources/npuap-pressure-ulcer- stagescategories/
 subcutaneous tissue and Category/Stage III ulcers can be shallow. In contrast, areas of significant adiposity can develop extremely deep Category/Stage III pressure ulcers. Bone/tendon is not visible or directly palpable. Category/Stage IV: Full thickness tissue loss Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present. Often includes undermining and tunneling. The depth of a Category/Stage IV pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have (adipose) subcutaneous tissue and these ulcers can be shallow. Category/Stage IV ulcers can extend into muscle and/or supporting structures (e.g., fascia, tendon or joint capsule) making osteomyelitis or osteitis likely to occur. Exposed bone/muscle is visible or directly palpable. NPUAP Staging Report National Pressure Ulcer Advisory Panel (NPUAP). stagescategories/. Accessed 2/14/2013www.npuap.org stagescategories/.")
37
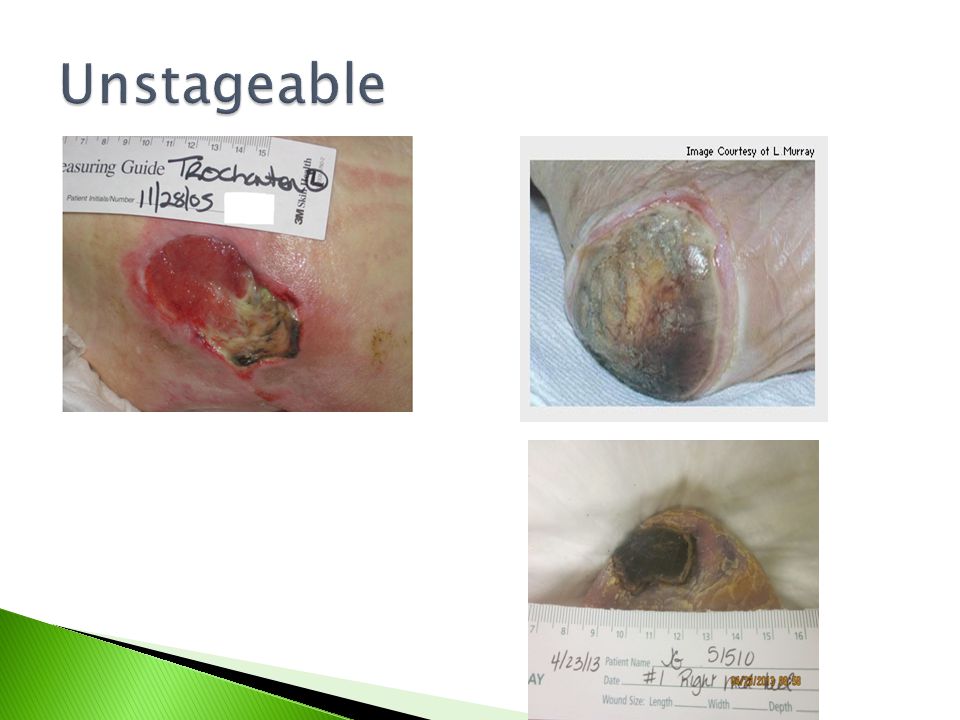
Unstageable/Unclassified: Full thickness skin or tissue loss – depth unknown Full thickness tissue loss in which actual depth of the ulcer is completely obscured by slough (yellow, tan, gray, green or brown) and/or eschar (tan, brown or black) in the wound bed. Until enough slough and/or eschar are removed to expose the base of the wound, the true depth cannot be determined; but it will be either a Category/Stage III or IV. Stable (dry, adherent, intact without erythema or fluctuance) eschar on the heels serves as “the body’s natural (biological) cover” and should not be removed. Suspected Deep Tissue Injury – depth unknown Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue. Deep tissue injury may be difficult to detect in individuals with dark skin tones. Evolution may include a thin blister over a dark wound bed. The wound may further evolve and become covered by thin eschar. Evolution may be rapid exposing additional layers of tissue even with optimal treatment. NPUAP Staging Report. 2007. National Pressure Ulcer Advisory Panel (NPUAP). www.npuap.org. http://www.npuap.org/resources/educational-and-clinical-resources/npuap-pressure-ulcer- stagescategories/. Accessed 2/14/2013www.npuap.org http://www.npuap.org/resources/educational-and-clinical-resources/npuap-pressure-ulcer- stagescategories/
 eschar on the heels serves as the body’s natural (biological) cover and should not be removed. Suspected Deep Tissue Injury – depth unknown Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue. Deep tissue injury may be difficult to detect in individuals with dark skin tones. Evolution may include a thin blister over a dark wound bed. The wound may further evolve and become covered by thin eschar. Evolution may be rapid exposing additional layers of tissue even with optimal treatment. NPUAP Staging Report National Pressure Ulcer Advisory Panel (NPUAP). stagescategories/. Accessed 2/14/2013www.npuap.org stagescategories/.")
40
Goal is for offloading ◦ Air cushion in chairs ◦ Foam cushion in chairs ◦ Alternating low air loss/air mattress

Similar presentations
















>")
 for Pressure Ulcers>")

















 A pressure ulcer is localized injury to the skin and/or underlying.>")