Download presentation
Presentation is loading. Please wait.

1
Peritoneal Dialysis Julie Stinson
Specialist Nurse, Renal Community Team University Hospitals of Leicester

2
Aims and Objectives To give an overview of Peritoneal Dialysis – how it works, therapy options To discuss the solutions used for PD To discuss the pharmacological considerations in PD

3
Peritoneal Dialysis Introduced late 1970’s
Alternative treatment to Haemodialysis for End-stage Renal failure Home therapy, self-managed by patient Uses patients own natural membrane – the Peritoneum – for dialysis Need identified for pts to be able to dialyse at home, self-manage dialysis

4
What is Peritoneal Dialysis?
Peritoneal Dialysis (PD) utilises one of the bodies natural membranes Fluid flows through a small plastic tube (catheter) into the peritoneal cavity Whilst the fluid is inside the peritoneal cavity dialysis takes place The fluid is changed every few hours, this is called an exchange Peritoneal membrane acts as a filter Catheter inserted during a minor operation Peritoneal cavity Catheter
 utilises one of the bodies natural membranes. Fluid flows through a small plastic tube (catheter) into the peritoneal cavity. Whilst the fluid is inside the peritoneal cavity dialysis takes place. The fluid is changed every few hours, this is called an exchange. Peritoneal membrane acts as a filter. Catheter inserted during a minor operation. Peritoneal cavity. Catheter.")
5
The Peritoneal Cavity

6
How peritoneal dialysis works
Removal of solutes by DIFFUSION Removal of fluid by OSMOSIS

7
Peritoneal Dialysis Diffusion
Movement of solutes from a strong solution to a weak solution across a semi - permeable membrane 1 2 Blood Membrane Dialysate 1 - Red blood cell 2 - Bacteria Sodium Potassium Chloride Bicarbonate Urea Creatinine Uric acid Beta 2-m

8
Peritoneal Dialysis Osmosis Blood Dialysis Solution
Movement of water from an area of low solute concentration to an area of high solute concentration. Blood Dialysis Solution Water Solute

9
Suitable patients Well motivated/ independent Diabetic Elderly
Patients with residual renal function Needle phobic patients Patients with cardiac disease Have adequate storage space for fluids/ equipment

10
Contraindications for PD
Chronic back pain COPD Diverticular disease Previous abdominal surgery Social circumstances -Lack of space at home for supplies Inability to self- manage treatment: physical or cognitive function

11
Advantages of PD Home based therapy Easy to perform Flexible
Cheaper than hospital HD Gentle form of dialysis Fits into lifestyle- maintains independence Preserves renal function

12
More advantages Less dietary restrictions
Treatment of choice for diabetics No needles involved! No needles for Needlephobics!

13
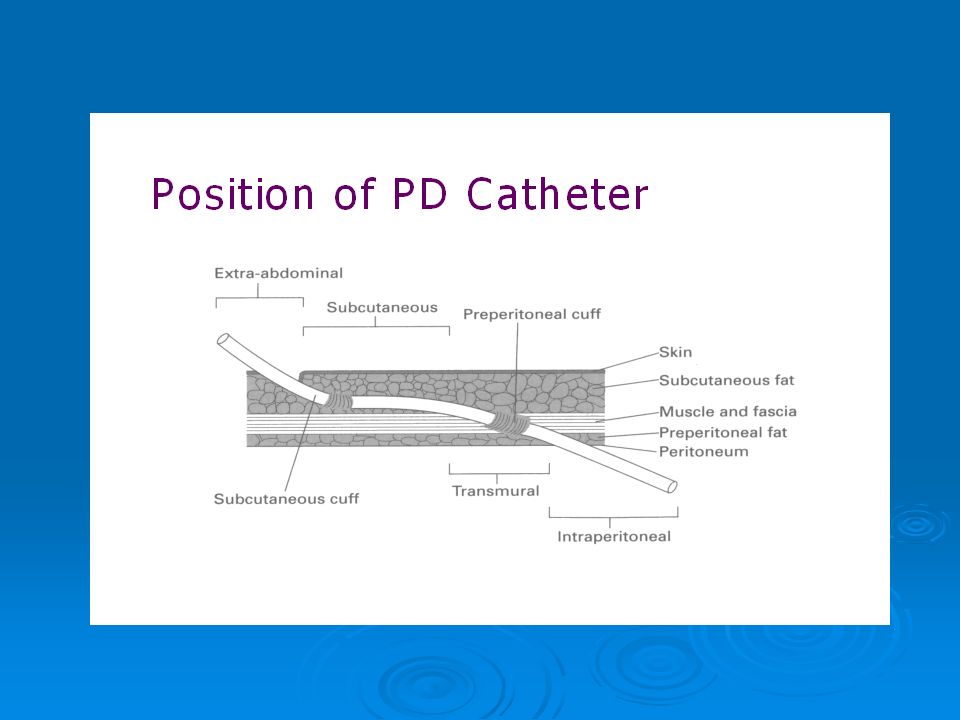
Catheter A flexible, silicone catheter is inserted into the Peritoneal cavity usually laproscopically (under local or general anaesthetic) Dacron cuffs secure in position in peritoneum Can be used after 2-4wks (post-operatively if necessary) SHOW CATHETER
 SHOW CATHETER.")
15
Types of Peritoneal Dialysis
CAPD APD

16
What is CAPD? CAPD stands for Continuous Ambulatory Peritoneal Dialysis CAPD can be performed in any clean and convenient place The manual exchanges use gravity to drain the used fluid out of the peritoneal cavity and replace it with fresh fluid Most CAPD patients need to do 4 bag exchanges per day CAPD can be performed in any clean and convenient place- at home, at work, at school, or on holiday

17
CAPD Continuous Ambulatory Peritoneal Dialysis
Dialysis takes place whilst patient continues normal daily activities Performed manually (usually) 4 times every day 1.5 – 2.5 litres of fluid per exchange Each exchange takes minutes
 4 times every day. 1.5 – 2.5 litres of fluid per exchange. Each exchange takes minutes.")
18
Automated Peritoneal Dialysis
Dialysis is performed by an automated machine and exchanges are done at night while patient sleeps Machine has 3 main functions: Heats PD fluid to body temperature Controls time of exchange and amount of fluid used Monitors treatment (safety alarms)
")
19
APD Automated Peritoneal Dialysis Performed every night
Free from exchanges during the day Greater flexibility in volume and time of exchanges Can be performed by a carer so possible for for patients unable to self manage Assisted APD will be discussed at forthcoming session

20
Types of PD fluids Primarily made up of glucose as this provides the osmotic gradient required to remove water Other constituents include Lactate/bicarbonate as a buffer Electrolytes i.e. sodium, calcium, etc Amino Acids/bicarbonate Varies from 1.5L to 3Litres

21
Types of PD Fluids Glucose Icodextrin - Extraneal
Amino acids - Nutrineal Bicarbonate - Physioneal (Baxter Healthcare) AIM_ BIOCOMPATIBILITY.
 AIM_ BIOCOMPATIBILITY.")
22
Glucose (as osmotic agent) in different concentrations:
Traditional PD fluids are glucose based and use Lactate as buffer - Bioincompatible Glucose (as osmotic agent) in different concentrations: 1.36%, 2.27% 3.86% More glucose = more fluid removal High concentrations of glucose – 1.36% bag = 75mmol/litre, 3.86% = 215mmol/l Risk of peritoneal damage increases with time
 in different concentrations: 1.36%, 2.27% 3.86% More glucose = more fluid removal. High concentrations of glucose – 1.36% bag = 75mmol/litre, 3.86% = 215mmol/l. Risk of peritoneal damage increases with time.")
23
Constant exposure to glucose can damage Peritoneum in time
Absorption of glucose leads to hyperglycaemia in Diabetics, insulin resistance, obesity

24
Glucose polymer, starch based fluid – 7.5% Icodextrin
Extraneal Glucose polymer, starch based fluid – 7.5% Icodextrin Allows better ultrafiltration Used once daily for longer dwell time (at least 8 hours) Reduces glucose load, so maintains better glycaemic control for diabetics; reduces weight gain AIM - Reduce Glu load, preserve peritoneum = Biocmpatible
 Reduces glucose load, so maintains better glycaemic control for diabetics; reduces weight gain. AIM - Reduce Glu load, preserve peritoneum = Biocmpatible.")
25
1.1% Amino acid – 87mmol/litre
Nutrineal 1.1% Amino acid – 87mmol/litre One bag per day – at mealtime exchange in CAPD, with o/night mix in APD Absorption rate 70-80% amino acids, hence can use in malnourished pts No glucose = less load!

26
Uses Bicarbonate + Lactate as buffer – Biocompatible
Physioneal Uses Bicarbonate + Lactate as buffer – Biocompatible Prolongs efficiency of peritoneum as dialysis membrane Prolong peritoneum – can aid length of time on PD

27
PHARMACOLOGICAL CONSIDERATIONS IN PD

28
Complications of PD (with Pharmacy involvement)
Peritonitis Exit site and Tunnel infection Constipation Mechanical Emphasise concentrate on comps with Pharm implications

29
Treatment protocols given are specific to University Hospitals of Leicester
Most PD units will have variations in protocols! – Please refer to your local policies EMPHASISE

30
Important to take regular laxatives Usually Lactulose and Senna
Constipation Constipation can lead to PD catheter problems- fluid will not drain out/in Important to take regular laxatives Usually Lactulose and Senna Some patients may need Sodium Docusate Picolax if severe constipation Lact and Senna usual

31
Blocked catheter caused by Fibrin May require UROKINASE lock
Urokinase 5000u in 5mls Saline - for 2 hour dwell into catheter Fibrin – protein naturally lost in PD

32
PD Peritonitis Inflammation of peritoneum usually due to infection
Signs and symptoms: Cloudy PD fluid +/- abdominal pain, ?fever, nausea, D and V Diagnosis based on symptoms of cloudy fluid, pain Fluid will show > 100 white cells; Identification of organisms on Gram stain or subsequent culture of fluid Dx – based on CLOUDY FLUID/Pain

33
Treatment of peritonitis
Outpatient ‘APD regime’ Gram positive - Bolus IP Vancomycin – 1-2gram dependant on body weight Gram negative - oral Ciprofloxacin (500mg bd) No organism – both Vanc and Cipro Day 4 – vanc level checked; <15mg/ml=further dose: Repeat at days 8 and 12
 No organism – both Vanc and Cipro. Day 4 – vanc level checked; <15mg/ml=further dose: Repeat at days 8 and 12.")
34
Inpatients regime Gram positive organisms - IP Vancomycin 25mg/litre for 10days Gram negative – IP Gentamycin 5mg/litre No growth – give both

35
Special considerations for Pseudomonas, fungal
IP Gentamycin 7.5mg/l alternate bags + Oral Ciprofloxacin 750mg bd Continued for 4 weeks (weekly Gent levels)? Tube removed if recurrent, non-resolving peritonitis Fungal – Tube removal (Ref: UHL Policy – PD peritonitis diagnosis and treatment)
 Tube removed if recurrent, non-resolving peritonitis. Fungal – Tube removal. (Ref: UHL Policy – PD peritonitis diagnosis and treatment)")
36
Recurrent peritonitis:
Rifampicin 600mg once day for 4 weeks (weekly LFTs) + Urokinase flush 5000u/5mls on day 4 and 7/8
 + Urokinase flush 5000u/5mls on day 4 and 7/8.")
37
Exit Site and Tunnel infections
Commonly caused by skin commensals Clinical signs of infection:- swab taken; Instigate abx treatment- Flucloxacillin 500mg qds x 5days (as appropriate) /Erythromicin 500mgs qds if Penicillin sensitive Gram positive organism -continue 7 days Gram negative – Ciprofloxacin 500mg bd x7days )
 /Erythromicin 500mgs qds if Penicillin sensitive. Gram positive organism -continue 7 days. Gram negative – Ciprofloxacin 500mg bd x7days. )")
38
If pt is Staph Aureus carrier, treated with nasal and topical Mupiricin (Swab each clinic visit
(ref: UHL policy: PD catheter ESI)
")
39
Tunnel infection Cause usually unresolved ESI. Inflammed tract under skin along tube tunnel= erythema, tenderness Treated with IV Vancomycin 1g; likely admission Tube removal if unresolved (r/v 48hrs)
")
40
THANK YOU!

Similar presentations






 Principles Peritoneum Fluid and Solute Removal PD Fluid Treatment modes CAPD/APD Complications Treatment Strategy.>")

>")










