Download presentation
Presentation is loading. Please wait.

1
Foot and Ankle orthopedics
Congenital deformities

2
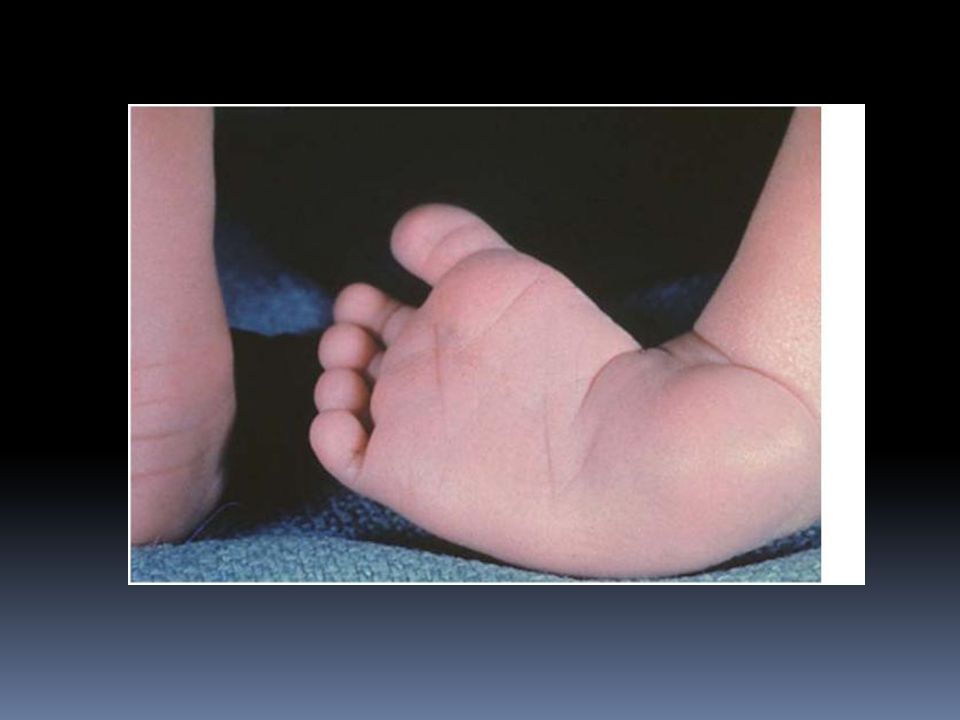
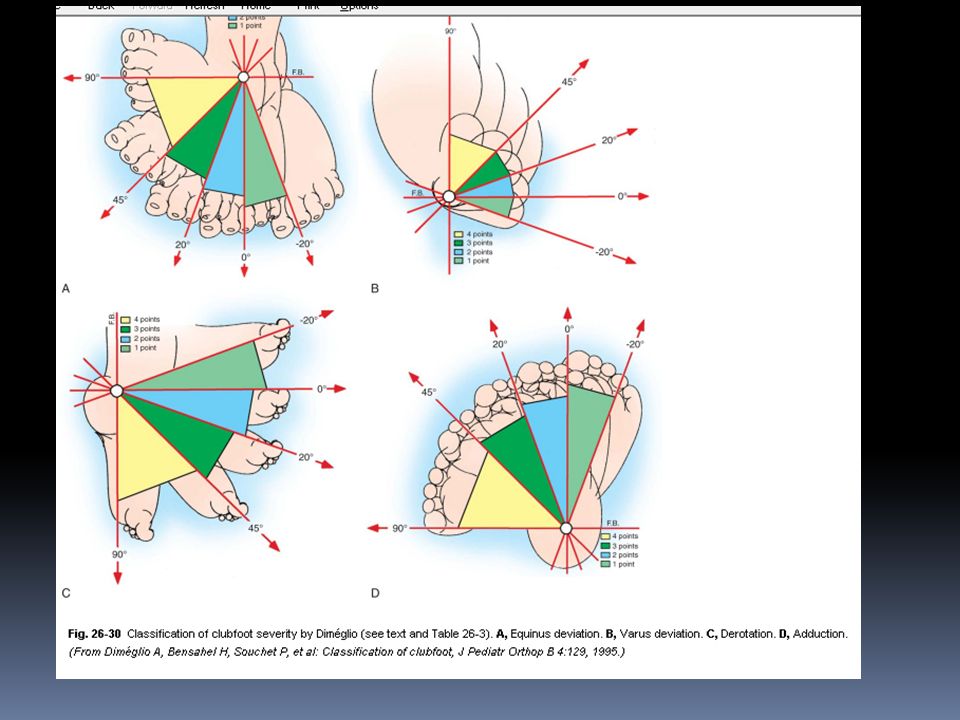
Talipes Equinovarus (Idiopathic clubfoot) talus= L anke bone, pes= L foot Equinus= heal tilted backward varus= heel deviated medially Incidence: 1-2/thousand births. Male/female = 2/1. Bilateral in 1/3rd of cases.

4
Etiology Idiopathic in most of cases, but may be associated with tight uterus as in primegravida uterus. Associated with myelomeningocele, congenital tibial deficiency and arthrogriposis.

5
Clinical features Components: Small heel and calf muscle.
Equinus of heel. Varus of hind foot. Adduction and supination of forefoot. Small heel and calf muscle. Exam for associated: DDH. Spina bifida. Arthrogriposis (absent creases in legs).
.")
6
Spina bifida with club foot

9
Treatment Conservative
Begin in the first few days of life. Ponseti Method: Weakly manipulation and POP casting. If conservative treatment fails ; then Operative treatment is considered.

10
Adhesive strapping

12
Pes Planus (flat-foot)
The medial border (arch of the foot) is in contact with the ground. Common among children. Types: Flexible flat-foot: normal variation usually disappears spontaneously. Rigid flat-foot: cannot be corrected passively. Compensatory flat-foot e g. short tendo achillis, or external rotation of lower limbs (Charlie Chaplin look) .
 is in contact with the ground. Common among children. Types: Flexible flat-foot: normal variation usually disappears spontaneously. Rigid flat-foot: cannot be corrected passively. Compensatory flat-foot e g. short tendo achillis, or external rotation of lower limbs (Charlie Chaplin look) .")
15
Rigid club foot

16
High Arched feet (Pes Cavus)
Caused by muscle imbalance usually due to neuromuscular disorder eg. Poliomyelitis. Associated with claw toes. Both feet affected. Often NO treatment required apart from well moulded shoes.

18
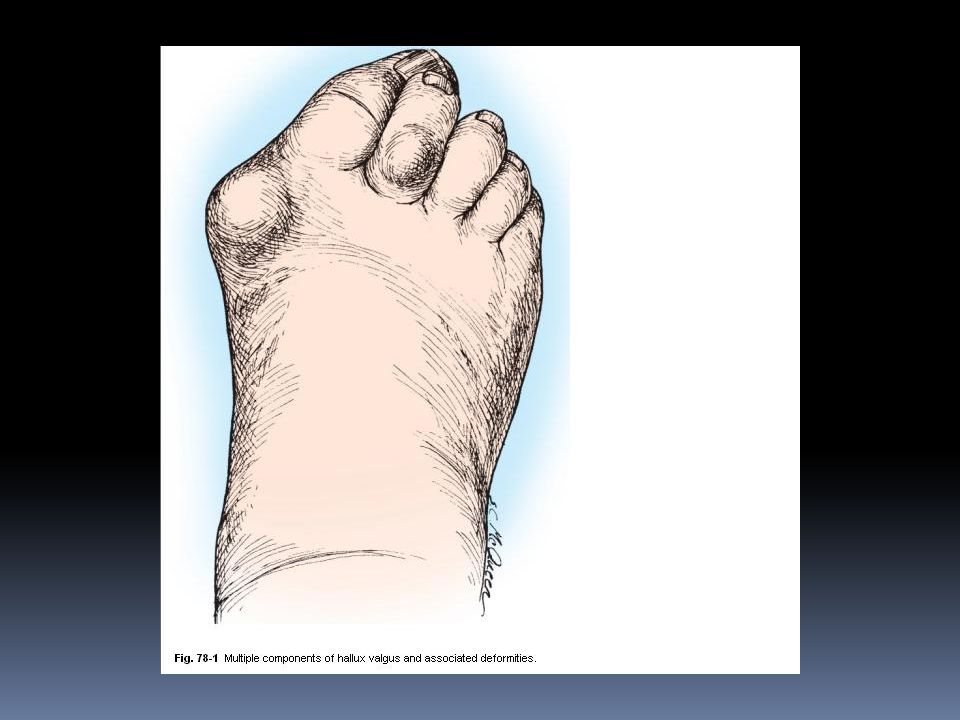
Halux Valgus Lateral angulation of the big toe due to varus angulation of the first metatarsal. Prominent head of first metatarsal (Bunion). In people who wear shoes. Loss of muscle tone in forefoot in elderly. In rheumatoid arthritis. Family history is common.

20
Clinical features In elderly women years or adolescents with positive family history. Usually bilateral. Painless deformity. Pain on inflammed buninion or OA of 1st MPJ. Difficulty in purchasing comfortable shoes.

22
Treatment Asymptomatic, mild and non-progressive deformity; conservative treatment: comfortable footwear with low heels. Severe, progressive and painful deformity requires surgical treatment.

23
Claw Toes Interphalangeal joints are flexed and metatarsophalangeal joint is extended. Seen in poliomyelitis, Rheumatoid arthritis but usually idiopathic. Associated with pes cavus.

25
Hammer Toes Proximal IPJ flexed, distal IPJ and MPJ extended.
Cause is obscure. Shoe pressure produce painful corns and callosities.

27
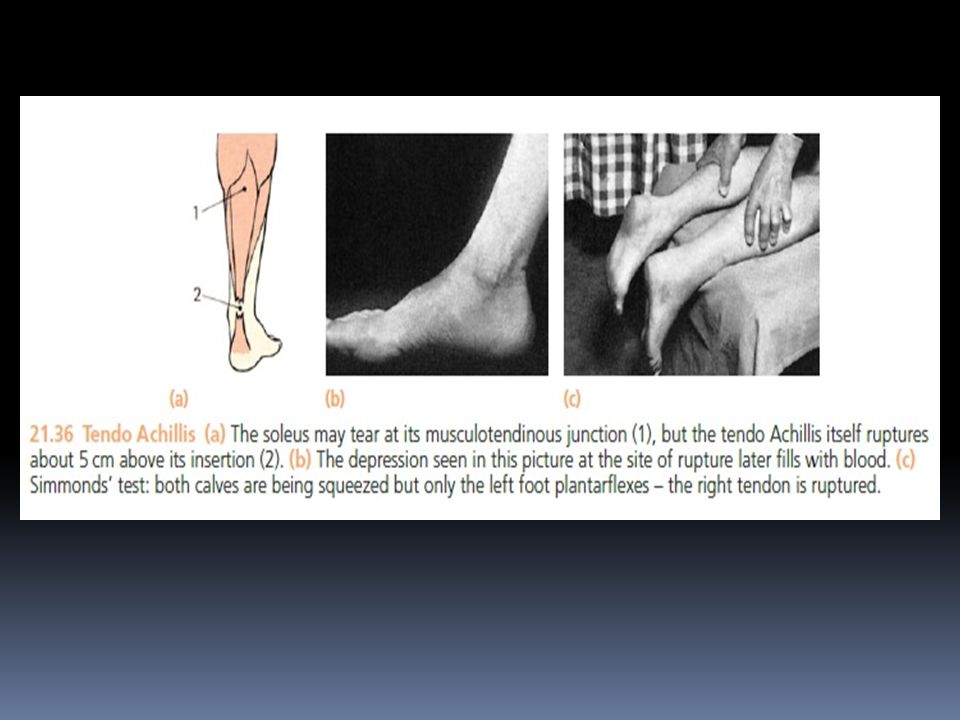
Rupture of Tendo Achillis
Age >40. After running or jumping feels a struck above the heel. Cannot tip toe. Gap is felt 5cm above heel. Simmond’s test: squeezing the calf causes planterflexion of foot normally. Absent planterflexion means rupture of the tendon.

29
Ruptured tendo achillis

30
Treatment Operative repair then POP in equinus for 8 weeks.

31
Traction apophysitis (Sever’s disease)
Pain and tenderness over Achillis tendon insertion. In boys around 10years old. Treat by raising the heel and abandon strenuous exercise.

32
Severs disease

33
Plantar Fasciitis Painful Heel
Common in Males 30-60yrs. Pain with first steps after inactivity (rising from bed). Obesity, prolonged standing, and stiff shoe soles are predisposing factors. Local tenderness. X-ray: boney spur. Treatment: NSAID, pad under heel, local C/S injection.
. Obesity, prolonged standing, and stiff shoe soles are predisposing factors. Local tenderness. X-ray: boney spur. Treatment: NSAID, pad under heel, local C/S injection.")
34
Calcaneal spur

35
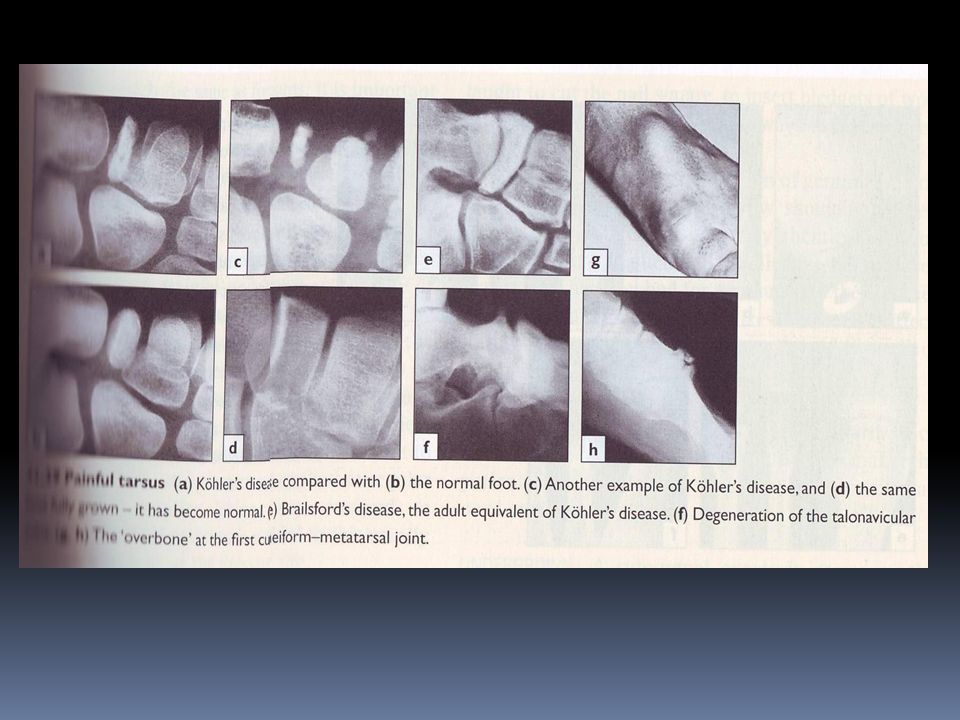
Köhler’s disease Osteochondritis of the navicular
Painful limp and tenderness in midfoot in children <5yrs. X-ray: dense, fragmented navicular bone. Usually resolve spontanuously.

37
Freiberb’s disease Crushing type of osteochondritis.
Affects head of 2nd metatarsal. Usually seen in young adult women.

Similar presentations




















 Dr. Mazloumi MD Associate Professor Pediatric Orthopedic Surgeon.>")





