Download presentation
Presentation is loading. Please wait.

1
ANEMIA

2
Key points Anemia is not a specific disease state but a sign of an underlying disorder There are several kinds of anemia. A physiologic approach classifies anemia according to whether ◦ the deficiency in erythrocytes is caused by a defect in their production (hypoproliferative anemia), ◦ by their destruction (hemolytic anemia), or ◦ by their loss (bleeding).
, ◦ by their destruction (hemolytic anemia), or ◦ by their loss (bleeding)..")
3
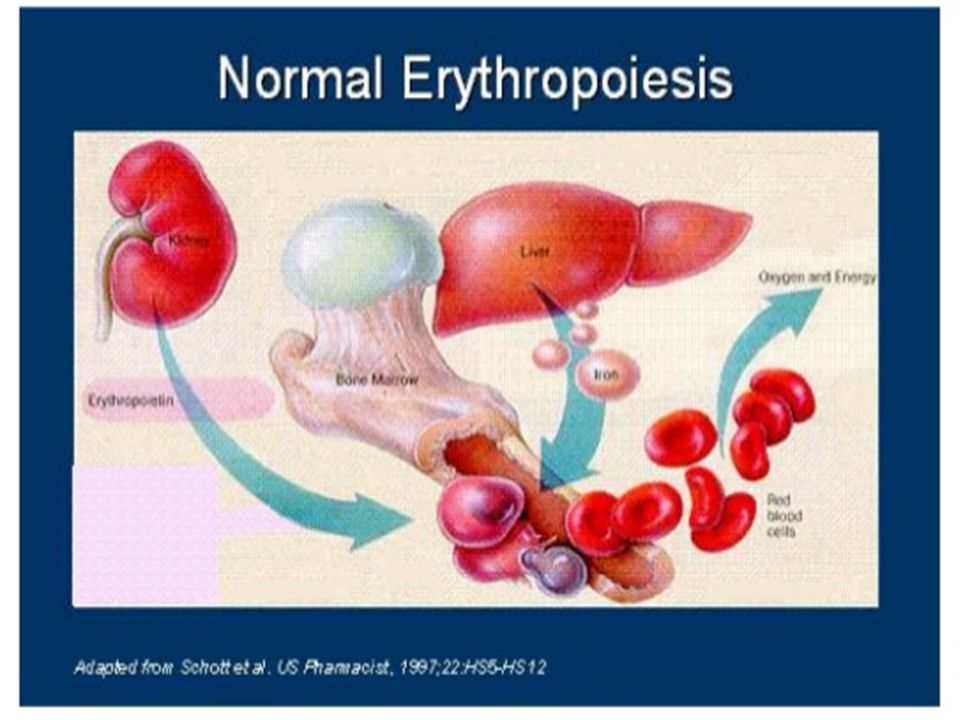
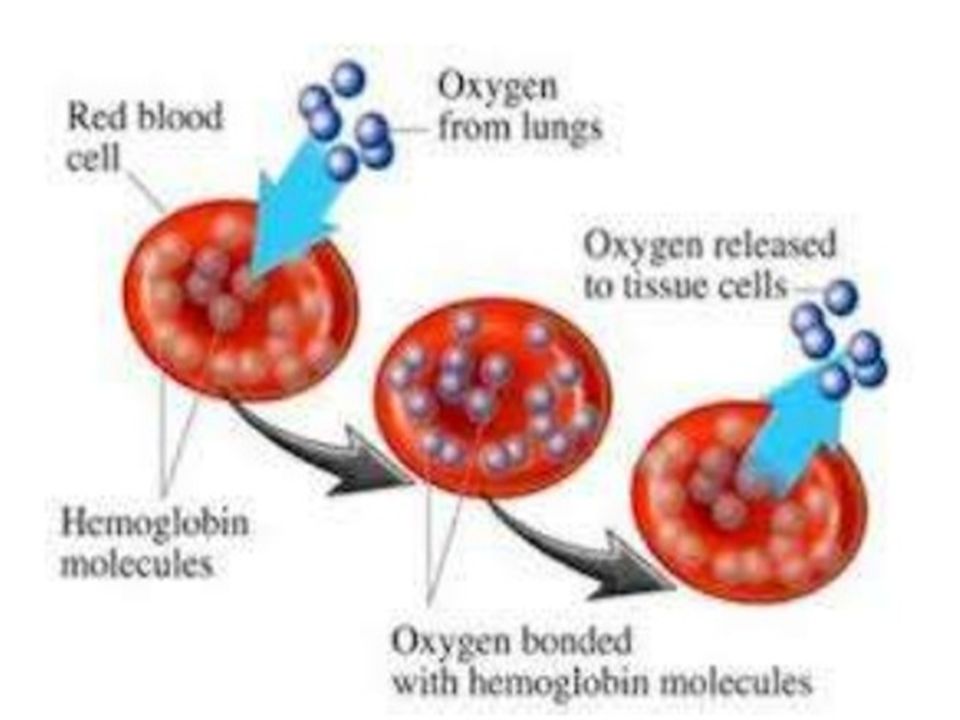
Key points a& Definitions Anemia is an abnormally low amount of circulating RBCs, Hgb concentration, Hct concentration, or all. Anemia results in diminished O2-carrying capacity and delivery to tissues and organs. Therefore, the goal of treatment is to restore and maintain adequate tissue oxygenation. Causes of Anemia: ◦ Blood loss. ◦ Inadequate RBC production. ◦ Increased RBC destruction. ◦ Insufficient or defective hemoglobin. Iron deficiency anemia is the most common anemia.

7
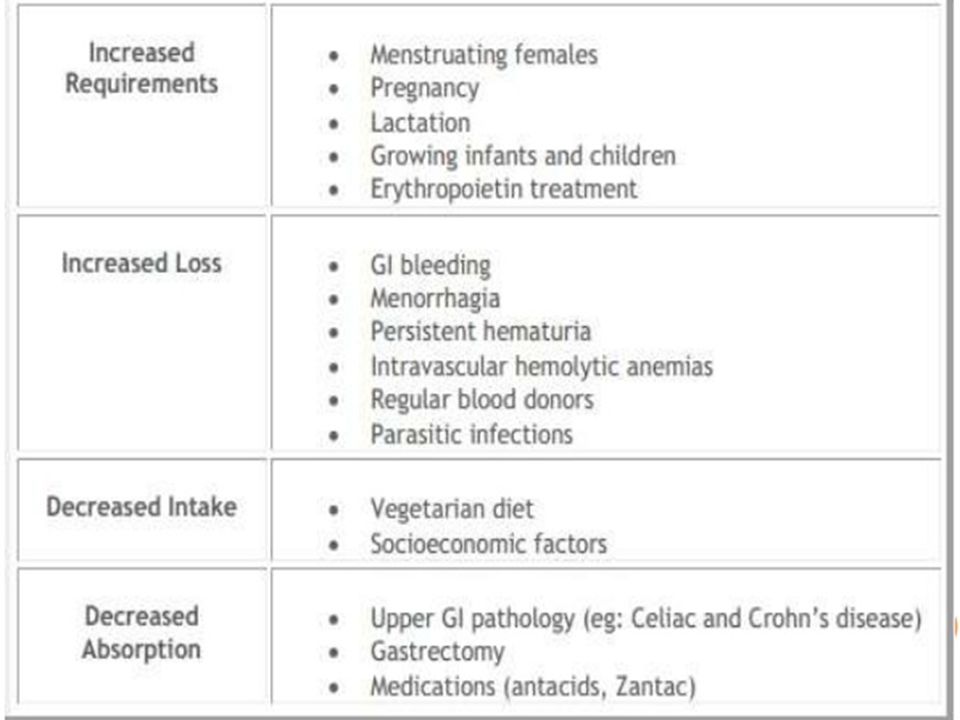
Risk Factors for Anemia Acute or chronic blood loss; menorrhagia, GI bleeding. Increased hemolysis; defective Hgb (sickle cell disease), impaired glycolysis (G6PD) deficiency anemia, immune disorder or destruction (transfusion reactions) Or mechanical trauma to RBCs (mechanical heart valve, cardiopulmonary bypass) Dietary inadequacy; IDA, megaloblastic anemia, pernicious anemia, pica Bone-marrow suppression; exposure to radiation or chemicals, aplastic anemia
, impaired glycolysis (G6PD) deficiency anemia, immune disorder or destruction (transfusion reactions) Or mechanical trauma to RBCs (mechanical heart valve, cardiopulmonary bypass) Dietary inadequacy; IDA, megaloblastic anemia, pernicious anemia, pica Bone-marrow suppression; exposure to radiation or chemicals, aplastic anemia.")
8
Anemia? Production? Survival/Destruction? The key test is the …..

10
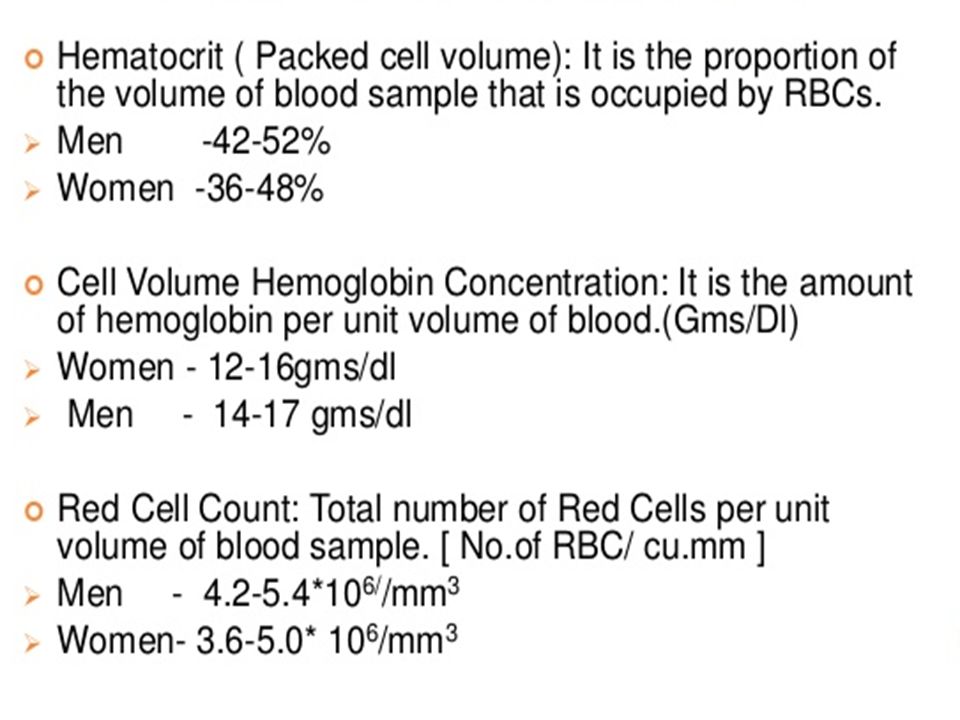
Diagnostic Procedures and Nursing Interventions Laboratory Assessment Complete blood count (CBC) ◦ RBCs ◦ Hemoglobin (Hgb) ◦ Hematocrit (Hct) ◦ WBCs ◦ Platelets
 ◦ RBCs ◦ Hemoglobin (Hgb) ◦ Hematocrit (Hct) ◦ WBCs ◦ Platelets")
13
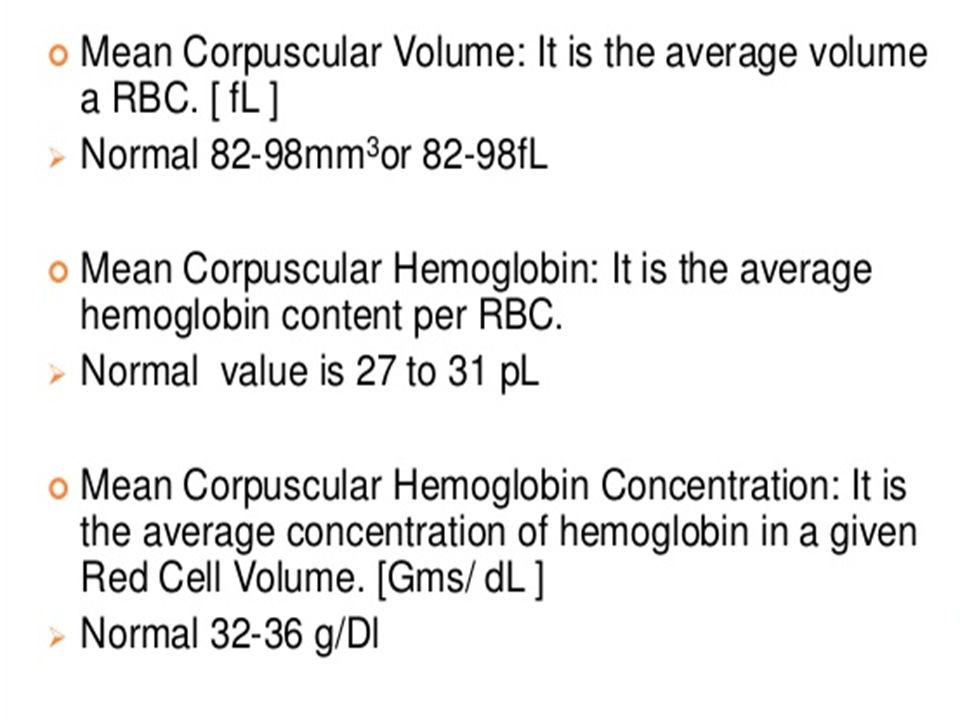
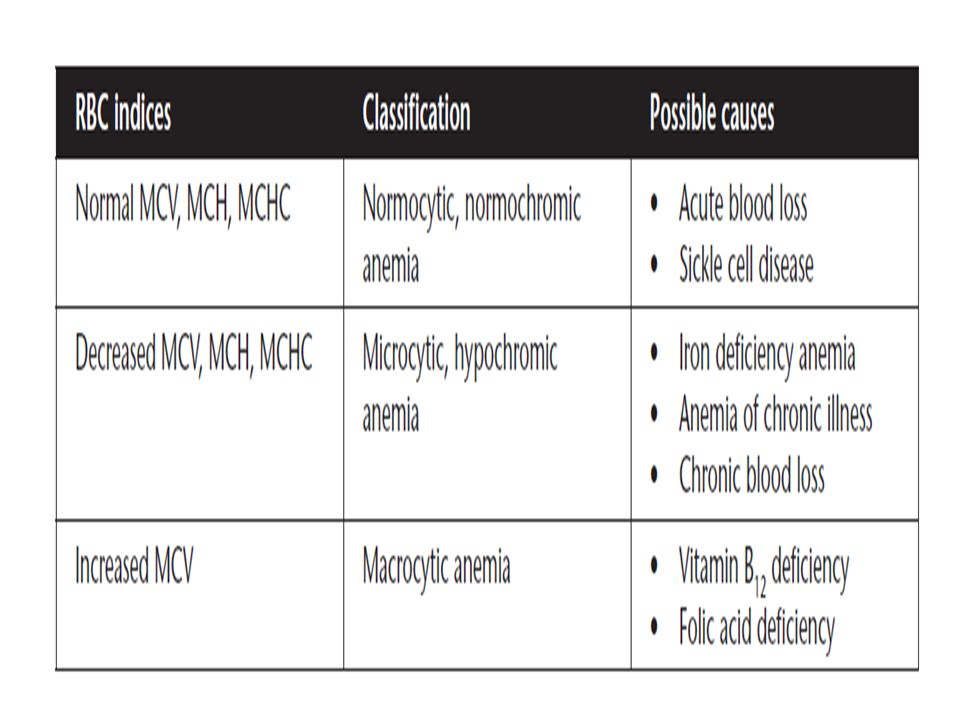
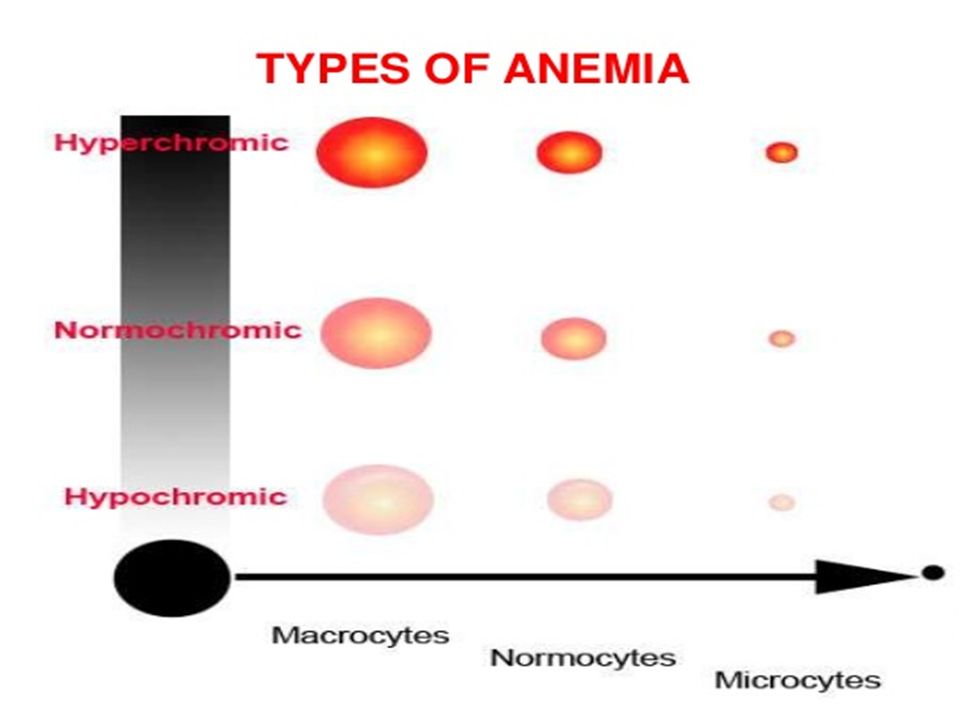
Diagnostic Procedures and Nursing Interventions RBC indices to determine the type and cause of most anemias: Mean corpuscular volume (MCV): size of red blood cells Normocytic – normal size Microcytic – small cells Macrocytic – large cells
: size of red blood cells Normocytic – normal size Microcytic – small cells Macrocytic – large cells")
15
Diagnostic Procedures and Nursing Interventions Mean corpuscular hemoglobin (MCH): to determine the amount of hemoglobin per RBC ◦ Normochromic – normal amount of Hgb per cell ◦ Hypochromic – decreased Hgb per cell Mean corpuscular hemoglobin concentration (MCHC): to indicate Hgb amount relative to the size of the cell
: to determine the amount of hemoglobin per RBC ◦ Normochromic – normal amount of Hgb per cell ◦ Hypochromic – decreased Hgb per cell Mean corpuscular hemoglobin concentration (MCHC): to indicate Hgb amount relative to the size of the cell")
18
Diagnostic Procedures and Nursing Interventions Iron studies ◦ Total iron-binding capacity (TIBC) reflects an indirect measurement of serum transference. Serum ferritin is an indicator of total body iron stores. Serum iron measures the amount of iron in the blood. Low serum iron and elevated TIBC indicates iron deficiency anemia.

19
Diagnostic Procedures and Nursing Interventions Hemoglobin electrophoresis separates normal hemoglobin from abnormal. It is used to detect thalassemia and sickle cell disease. ◦ Sickle cell test, ◦ Schilling test (vitamin B12)factor, used to differentiate between malabsorption and pernicious anemia. Bone marrow examination diagnoses aplastic anemia. After bone marrow aspiration: ◦ Apply pressure to the site for 5 to 10 min. ◦ Assess VS frequently. ◦ Apply pressure dressing. ◦ Monitor for signs of bleeding and infection for 24 hr.
factor, used to differentiate between malabsorption and pernicious anemia. Bone marrow examination diagnoses aplastic anemia. After bone marrow aspiration: ◦ Apply pressure to the site for 5 to 10 min. ◦ Assess VS frequently. ◦ Apply pressure dressing. ◦ Monitor for signs of bleeding and infection for 24 hr..")
21
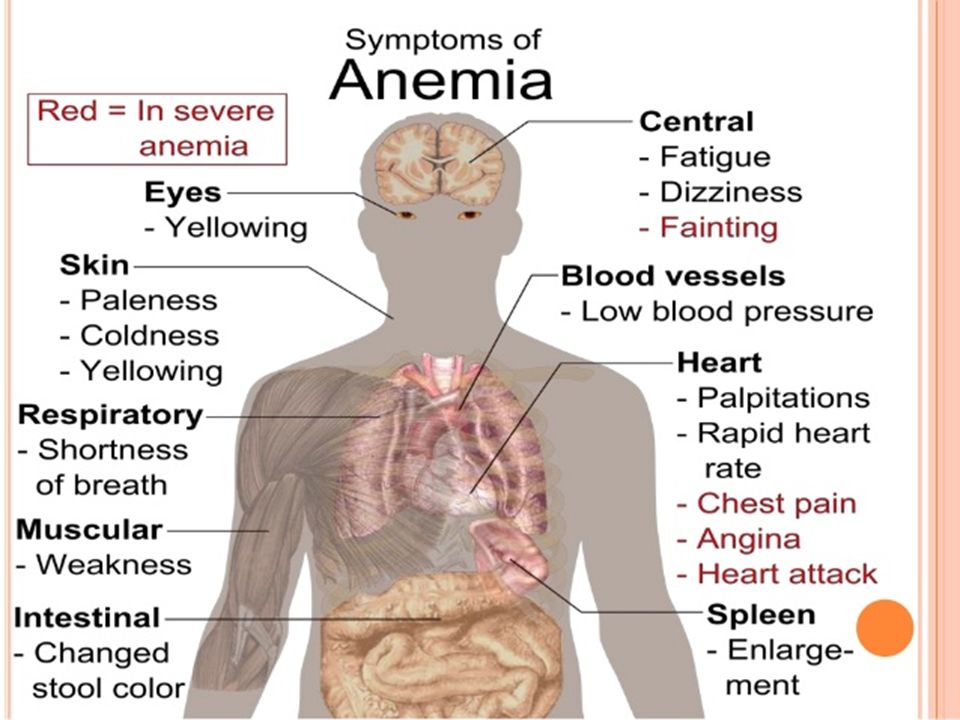
Clinical Manifestation Several factors influence the development of anemia-associated symptoms: ◦ the rapidity with which the anemia has developed, ◦ the duration of the anemia (ie, its chronicity), ◦ the metabolic requirements of the client, ◦ other concurrent disorders or disabilities (eg, cardiac or pulmonary disease), and ◦ complications or concomitant features of the condition that produced the anemia.
, ◦ the metabolic requirements of the client, ◦ other concurrent disorders or disabilities (eg, cardiac or pulmonary disease), and ◦ complications or concomitant features of the condition that produced the anemia.")
22
Moni tor for signs and symptoms May be asymptomatic in mild cases ◦ Pallor ◦ Fatigue ◦ Irritability ◦ Numbness and tingling of extremities ◦ Dyspnea on exertion ◦ Impaired skin healing ◦ Brittle, spoon-shaped nails (Koilonychia) ◦ Cheilosis ◦ Smooth, sore, bright red tongue ◦ Sensitivity to cold ◦ Brittle and ridged nails ◦ Pain and hypoxia with sickle cell crisis ◦ Leg cramps ◦ Pica
 ◦ Cheilosis ◦ Smooth, sore, bright red tongue ◦ Sensitivity to cold ◦ Brittle and ridged nails ◦ Pain and hypoxia with sickle cell crisis ◦ Leg cramps ◦ Pica")
25
Client’s respiratory status, activity tolerance, fatigue Client’s history regarding risk factors for anemia General appearance Laboratory and diagnostic findings

26
NANDA Nursing Diagnoses Risk for injury Activity intolerance Fatigue Self-care deficit Risk for infection Altered nutrition, less than body requirements Altered tissue perfusion Noncompliance with prescribed therapy

27
Nursing Interventions Assess and monitor laboratory results. Assess and monitor activity intolerance. Encourage increased dietary intake of the deficient nutrient (iron, vitamin B12, folic acid). Administer medications as prescribed; instruct the client on side effects. ◦ Iron supplements Oral iron supplements (ferrous sulfate, ferrous fumarate, ferrous gluconate) Parenteral iron supplements (iron dextran) ◦ Take with meals if gastrointestinal side effects occur.
. Administer medications as prescribed; instruct the client on side effects. ◦ Iron supplements Oral iron supplements (ferrous sulfate, ferrous fumarate, ferrous gluconate) Parenteral iron supplements (iron dextran) ◦ Take with meals if gastrointestinal side effects occur..")
28
Nursing Interventions ◦ Vitamin C improves absorption. ◦ Do not take within 2 hr of milk or antacids (Al, Ca, Mg), proton pump inhibitor. ◦ Stools will be black. ◦ May cause constipation; increase intake of fluids and foods high in fiber. ◦ May use sustained release iron tabs ◦ Use a straw with liquid iron to avoid staining of teeth. ◦ Administer parenteral iron using Z-track method. Erythropoietin (Procrit) Cobalamin (vitamin B12) parenterally or intranasally Folic acid supplements Oxygen Vitamin C supplements (to enhance iron absorption) IV fluids (sickle cell crisis, G6PD anemia) Teach the client and family about energy conservation.
, proton pump inhibitor. ◦ Stools will be black. ◦ May cause constipation; increase intake of fluids and foods high in fiber. ◦ May use sustained release iron tabs ◦ Use a straw with liquid iron to avoid staining of teeth. ◦ Administer parenteral iron using Z-track method. Erythropoietin (Procrit) Cobalamin (vitamin B12) parenterally or intranasally Folic acid supplements Oxygen Vitamin C supplements (to enhance iron absorption) IV fluids (sickle cell crisis, G6PD anemia) Teach the client and family about energy conservation..")
29
Nursing Interventions Teach the client the time frame for resolution. ◦ Transfusions – lead to an immediate improvement in blood cell counts and client signs and symptoms. Typically only used when the client has significant symptoms of anemia because of the risk of blood-borne infections. Oral supplements – 4 to 6 weeks for increase in RBCs Vitamin B12 supplements – increased RBCs in 1 week Vitamin B12 supplementation ◦ B12 supplementation can be given orally if the deficit is due to poor dietary intake. ◦ However, with pernicious anemia it must be given parenterally because it won’t be absorbed if given orally. ◦ Administer parenteral forms intramuscularly or deep subcutaneous to decrease irritation. Do not mix other medications in the syringe. Pernicious anemia must be treated for life.

30
Nursing Interventions Folic acid supplementation Can be given orally or parenterally. Large doses will stain urine dark yellow.

31
Complications and Nursing Implications Monitor the client for signs of hypoxemia: dyspnea, decreased oxygen saturation, central cyanosis. Administer oxygen therapy. Monitor SaO2. Administer blood transfusions as ordered. Assess the neurologic status of clients with macrocytic anemias. Vitamin B12 is essential for neurological function. Administer supplements. Notify the provider of any changes in mentation.

32
Complications and Nursing Implications Sickle Cell Crisis An autosomal recessive condition. At least 40% of total hemoglobin is the abnormal hemoglobin S (HbS) in sickle cell disease. When exposed to hypoxic environments, it contracts and clusters together within the cell. Cells become rigid, forming a “sickle” or “C” shape which causes them to clump together and impede blood flow; leading to further tissue hypoxia. S & Sx: cyanosis, abdominal pain, leg and back pain, low-grade fever, seizures, and stroke manifestations (weakness, paresthesia). Administer oxygen and hydration therapy. As well as analgesia. Organ failure can result if left untreated.
 in sickle cell disease. When exposed to hypoxic environments, it contracts and clusters together within the cell. Cells become rigid, forming a sickle or C shape which causes them to clump together and impede blood flow; leading to further tissue hypoxia. S & Sx: cyanosis, abdominal pain, leg and back pain, low-grade fever, seizures, and stroke manifestations (weakness, paresthesia). Administer oxygen and hydration therapy. As well as analgesia. Organ failure can result if left untreated..")
Similar presentations









/ HYPOCHROMIC &/or (NORMO)/ MICROCYTIC ANEMIAS 1. Disorders of iron utilization a. iron deficiency b. anemia of.>")




. Mild forms of anemia may go undiagnosed.>")







