Download presentation
Presentation is loading. Please wait.

1
Tendonitis and Bursitis Thomas Mullin, MD, CAQSM

2
Neither I, Thomas Mullin, MD, nor any family member(s) have any relevant financial relationships to be discussed, directly or indirectly, referred to or illustrated with or without recognition within the presentation. Disclosure

3
1. What are tendons and bursas and why can they cause pain? 2. What are the commonly affected areas for tendonitis and bursitis? 3. How can I get the pain to go away and get back to my normal activities? Objectives

4
Tendons connect muscle to bone Ligaments connect bone to bone A tendon is a tough band of tissue that connects muscle to bone They are capable of withstanding tension They transmit the force produced by muscles to the bone and cause movement at joints. What is a Tendon?

7
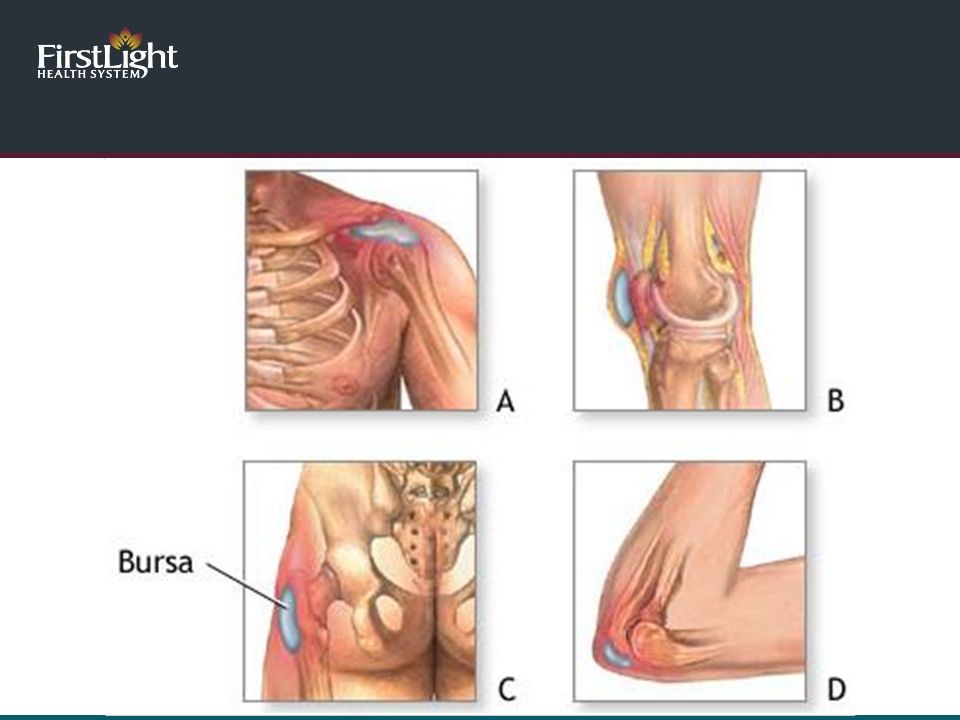
Bursae are flattened sacs that contain fluid Protective layer between bones and muscles or between bones and tendons/skin. Reduce friction and aid in smooth motion Humans have approximately 160 bursae What is a Bursa?

9
Suffix “itis” means inflammation Usually occurs from overuse Little if any inflammation in the tendons when evaluated microscopically Tears Disorganization Change in the cell type Better term is Tendinopathy which indicates an abnormality in the tendon For this talk we will continue to refer to the problem as tendonitis What is Tendonitis?

10
Tendonitis

12
Inflammation or irritation of the bursa May be the result of Overuse Injury Infection Other conditions Gout, arthritis What is Bursitis?

13
Bursitis

14
Tendonitis and Bursitis

15
Shoulder Rotator Cuff Tendonitis and Bursitis Biceps Tendonitis Elbow Tennis Elbow Golfer’s Elbow Olecranon bursitis Wrist DeQuervain’s syndrome Commonly Affected Areas Upper Body

16
Hip Trochanteric bursitis Gluteal Tendonitis Knee Patellar tendonitis Ankle Achilles tendonitis Foot Plantar fasciitis Commonly Affected Areas Lower Body

17
Shoulder

20
Pain in the shoulder and upper arm Usually worse with activity Pain is often worse with overhead motions Risks Repetitive overhead shoulder activity Rotator cuff weakness Overhead athletes Older patients can develop rotator cuff tears from chronic impingement Calcium can be deposited into the rotator cuff that can cause pain Shoulder Rotator Cuff Tendonitis and Bursitis

21
Shoulder

22
Calcific Tendonitis

23
Shoulder

24
Pain in the front of the shoulder Worse with reaching outwards and with lifting objects (grocery bags) Caused by overuse of the biceps Risks Repetitive use of the upper extremities with overhead motion Painting, throwing, swimming, racquet sorts Shoulder Biceps Tendonitis
 Caused by overuse of the biceps Risks Repetitive use of the upper extremities with overhead motion Painting, throwing, swimming, racquet sorts Shoulder Biceps Tendonitis")
25
Elbow

26
Tennis Elbow

27
Elbow Tennis Elbow

28
Tennis Elbow is also called “Lateral Epicondylitis” Pain at the outside part of the elbow Worse with wrist and elbow motion Occurs in dominant arm 75% of the time Risks Risks : age 40 – 60 years old Poor technique or equipment in tennis 90% of tennis elbow precipitated by activities that require repetitive wrist extension Elbow Tennis Elbow

29
Elbow Golfer’s Elbow

30
Elbow Golfer’s Elbow

31
Also known as “Medial Epicondylitis” Pain at the inside aspect of the elbow Dominant hand most often affected Usually due to repetitive flexion and pronation at the wrist and elbow Racquet sports, swimming, golfing, carpenters, plumbers, and butchers may be at risk Elbow Golfer’s Elbow

32
Elbow Golfer’s Elbow

33
Pain and swelling over the back of the elbow Injury or infection irritates the cells of the bursa and causes them to produce an abnormal amount of fluid Can be from injury or repetitive use seen in sports Wrestling, volleyball, football Other activities requiring repetitive use (carpentry) Infection Infections cause ~ 20% of olecranon bursitis Elbow Olecranon Bursitis
 Infection Infections cause ~ 20% of olecranon bursitis Elbow Olecranon Bursitis")
34
Elbow Olecranon Bursitis

35
Elbow Olecranon Bursitis

36
Wrist DeQuervain’s Tenosynovitis

37
Irritation of the tendons that move the thumb and wrist Commonly seen in 30 -50 year olds More common in females Most common tendonitis of the dorsal wrist Pain along the wrist around the thumb, worse with moving the wrist or thumb Risks – activities requiring forceful grasp with excessive ulnar deviation Repetitive use of the thumb Golf, bowling, racquets sports Wrist DeQuervain’s Tenosynovitis

38
Wrist DeQuervain’s Tenosynovitis

39
Lower Body

40
Hip

42
Greater Trochanteric Pain Syndrome

43
Called Greater Trochanteric Pain Syndrome Pain can be from bursitis or it can be from tendonitis of the muscles that attach to the hip Pain at the outside hip, worse with walking, standing, rising after sitting, lying on affected side, squatting, climbing stairs Risks 30 – 60 years old More common in females Common in runners and those with hip arthritis, knee problems, leg length differences, hip replacements, weakness of the hip stabilizers, flat feet Hip Trochanteric Bursitis and Gluteal Tendonitis

44
Hip Greater Trochanteric Pain Syndrome

45
Knee

47
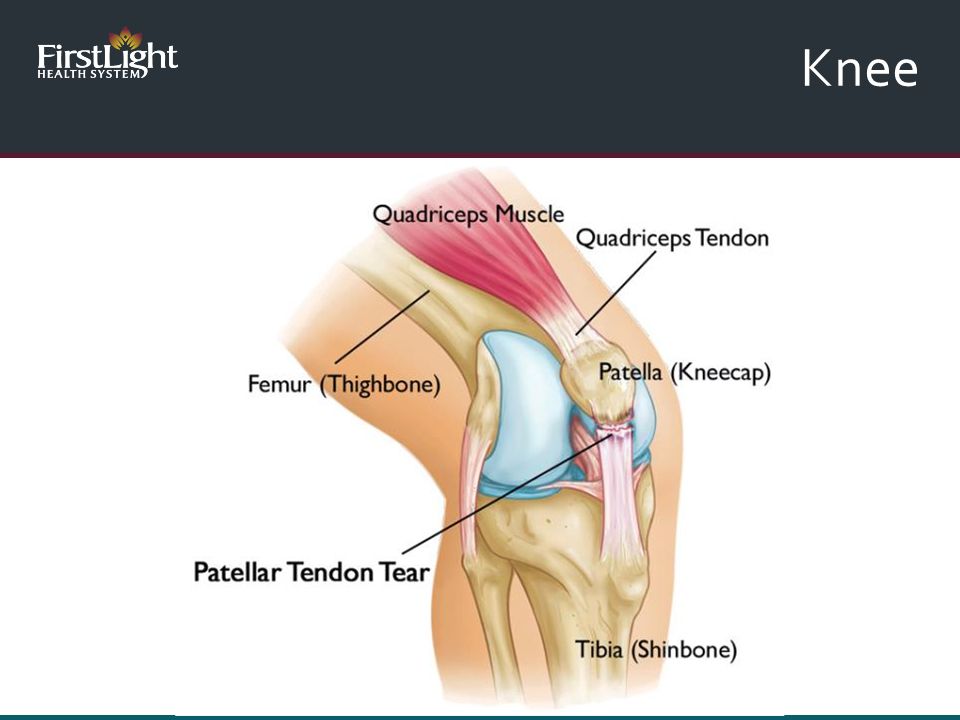
Also known as Patellar Tendonitis Pain in the front of the knee that is worse with activities like running and jumping Common 40-50% among high level volleyball players and 35-40% among elite basketball players Occurs from overuse Common in activities with excessive jumping or running (volleyball, basketball, soccer, track and field) Risks Excessive jumping sports, increasing training volume and intensity, poor flexibility of quads and hamstrings Knee Jumper’s Knee
 Risks Excessive jumping sports, increasing training volume and intensity, poor flexibility of quads and hamstrings Knee Jumper’s Knee")
48
Knee Prepatellar Bursitis

49
Knee

50
Most common knee bursitis Swelling, pain and inflammation at the front of the knee Usually from repeated kneeling or trauma to the knee Carpet layers, carpenters, wrestlers Can be caused by an infection Remove the fluid and send to the lab for analysis Knee Prepatellar Bursitis

51
Ankle

52
Achilles Tendonitis

53
Ankle Achilles Tendonitis

54
Overuse injury of the Achilles tendon that causes pain in the back of the calf and heel. Heel pain that initially gets better with activity but over time pain returns with continued use Morning stiffness is common Risks: In running and jumping sports lifetime incidence is 50% Recent increase in activity level, duration or intensity Inflexibility and tight heel cords Leg malalignment from the hip or the knee Flat feet Worn shoes – change shoes every 250 – 500 miles, pain with running and sprinting Recent use of antibiotics Ankle Achilles Tendonitis

55
Foot Plantar Fasciitis

56
Foot Plantar Fasciitis

57
Foot Plantar Fasciitis

58
Pain at the bottom of the heel Worse with first few steps out of bed in the AM Pain worsens after prolonged sitting, lessens with activity and worsens at the end of the day Can be bilateral 2 million cases in the US, accounts for 80% of patients with plantar heel pain Peak age is 40 – 60 years old Risks – Gait abnormalities, limited flexibility, poor footwear, obesity, prolonged standing Spurs – 50% of patients with Plantar fasciitis have heel spurs, 19% of patients without plantar fasciitis have heel spurs Heel spurs can occur with plantar fasciitis but they are not the cause Foot Plantar Fasciitis

59
Foot Plantar Fasciitis

60
Treatment Options

61
Rest Ice 20 – 30 minutes, 3 – 4 times per day Activity modification Adequate warm up and cool down routine Stretching Over the counter medications Acetaminophen, ibuprofen, naproxen New or supportive shoes for lower extremity conditions Treatment Common Sense Approach

62
Treatment Options

63
Physical therapy and Occupational therapy Stretching Strengthening Addressing biomechanical causes for the pain Modalities Iontophoresis Kinesiotaping/McConnell Taping Ultrasound Treatment Options Physical Therapy

64
Treatment Options Stretching

65
Treatment Options Eccentric Strengthening

66
Treatment Options Kinesiotaping and McConnell Taping

67
Treatment Options Taping

68
Treatment Options Ionotophoresis

69
Treatment Options Ionotophoresis

70
Bracing and immobilization Prescription strength NSAIDS Short term 1 – 2 weeks Naproxen, Meloxicam, Oral or Topical Diclofenac Treatment Options

83
Topical nitroglycerin patch Improves blood flow Good success when combined with physical therapy Headache is a common side effect Treatment Options Topical Nitroglycerin

84
Treatment Options

86
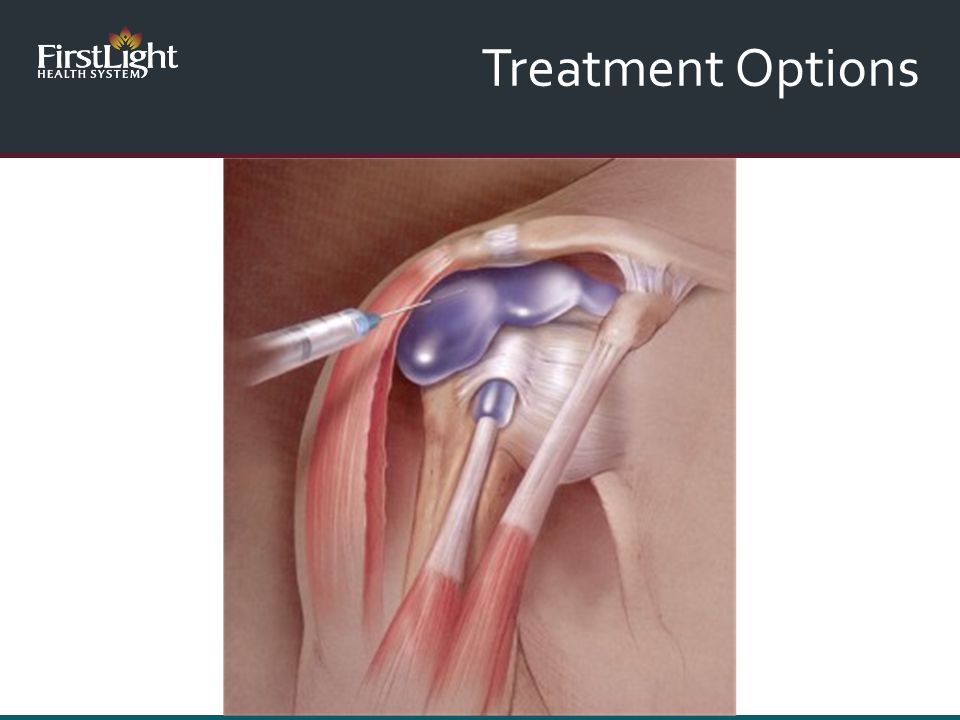
Injections “Cortisone Injections” More commonly used for the shoulder, hip and wrist Never for the Achilles tendon Use to improve pain so physical therapy is tolerated PRP, autologous blood, stem cells Ongoing research, some looks promising, stay tuned Insurance does not currently cover this procedure Cost ~$500 - $7,000 Treatment Options

88
Injection for Calcific Tendonitis

89
Treatment Options

90
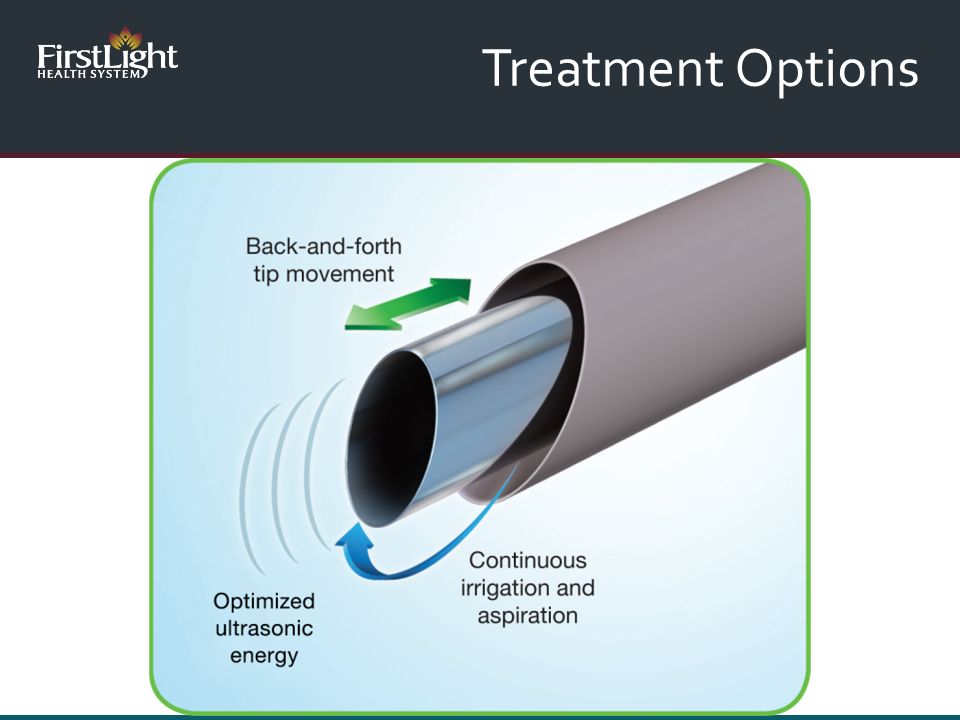
Tenex Ultrasound guided percutaneous needle tenotomy Option if symptoms don’t resolve after 4 months Minimally invasive procedure done under local anesthetic (numbing) Remove the diseased tissue and stimulate a response for the body to heal and repair the damaged tendon Can usually resume all activities about 6 weeks after the procedure Treatment Options
 Remove the diseased tissue and stimulate a response for the body to heal and repair the damaged tendon Can usually resume all activities about 6 weeks after the procedure Treatment Options")
91
Tenex Shoulder Calcific Tendonitis Elbow Tennis Elbow Golfer’s Elbow Knee Jumper’s Knee/Patellar Tendonitis Ankle Achilles Tendonitis Foot Plantar Fasciitis Treatment Options Tenex

92
Treatment Options

97
https://www.youtube.com/watch?v=avv36GEE8Sw Treatment Options

98
Tendonitis and bursitis are common Usually the pain resolves within 6 months If it persists the chance of it resolving without intervention is low Physical therapy can help Oral medications can be helpful for short term pain relief Cortisone injections have varying levels of success depending on the problem Topical nitroglycerin and Tenex can be helpful if symptoms do not resolve in 4 – 6 months Summary

99
Questions?

Similar presentations


































 and pulsating in nature, lasting from 4 to 72 hours; symptoms include.>")

 that causes pain, tenderness and occasionally,>")

