Download presentation
Presentation is loading. Please wait.

1
Fishing for a Diagnosis - “Nervous” infections
Neurology Grand Rounds 08 January 2009 Antony Thomas Consultant Neurologist UHCW & Alexandra hospital Redditch

2
Best Wishes for a Happy, successful, peaceful and prosperous New Year to all.

3
RC 23 years, Right handed, sheep farmer Well until 8/05/08
Occipital headache: severe Nausea, vomiting Blurred vision, double vision Dribbling “behaves as drunk” slurred speech, dizziness and unsteady Weak right face with failure to close right eye

4
RC A&E @ WRH 10/05/08 CT Head: ? Normal Sent home
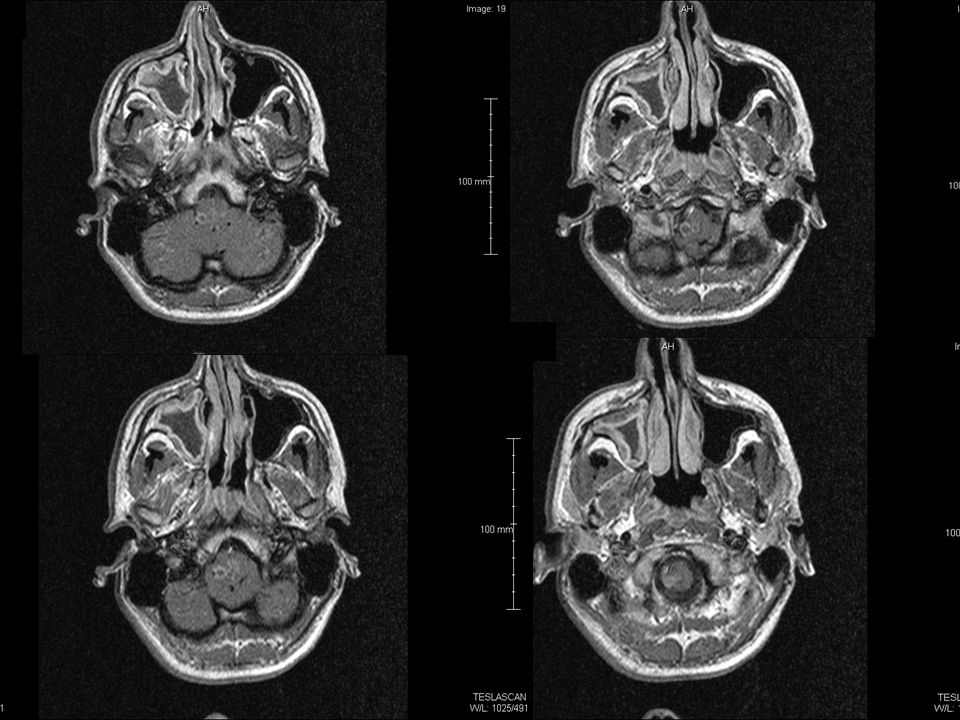
Readmitted at WRH 14/05/08 with deterioration, worsening headache, slurring, decreased swallow, diplopia MR Brain: abnormal

9
Transferred to Neurosurgery UHCW 16th
Pyrexial GCS 15, no papilledema Right V1 sensory impairement Right eye abduction weakness Bilateral nystagmus R>L Right Facial weakness LMN Bulbar paresis, dysarthria, right sided tongue weakness Mild right sided weakness and minimal sensory impairement Right sided cerebellar signs Rest of the systemic examination unremarkable

10
Investigations Leukocytosis, Neutrophilia, Monocytosis Impaired LFT
Deteriorating Renal functions CRP normal 85 172 Autoantibodies: negative HIV: Negative Serum ACE: normal

11
Microbiology @ Worcester
Telephone call Blood culture (14/05 sample): grown Listeria Started on antibiotics after repeating cultures Amoxicillin 2G Q4H Gentamicin
: grown Listeria. Started on antibiotics after repeating cultures. Amoxicillin 2G Q4H. Gentamicin.")
12
Progress Respiratory distress Poor cough, inadequate gag
Throat suction: thick yellowish secretions Hypoxic, hypercapneic Chest crackles more on right lower base CXR: Right lower lobe opacity

14
Transfer to ITU Intubated and ventilated ARDS: on oscillator
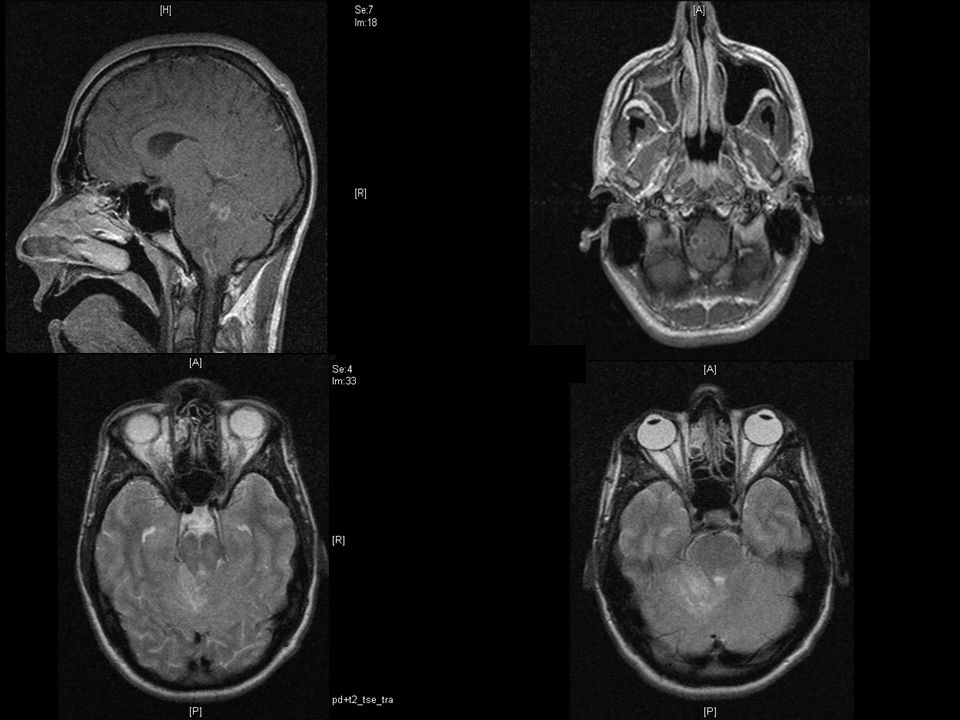
Hydrocortisone Co-trimoxazole added Repeat MR Brain: similar findings

17
BLOOD CULTURE REPORT POSITIVE :Gram positive bacilli Erythromycin S
Erythromycin S Fusidic Acid R Gentamicin S Penicillin R Trimethoprim S Vancomycin S Listeria monocytogenes isolated

18
Progress Cardiorespiratory arrest x 2 Succesful CPR Amiodarone
Gradually improved CXR got better

20
Progress Unfortunately………………… Desaturating
More ventilatory requirements Worsening respiratory, liver and renal functions Pupil unequal and dialated R.I.P

21
Listeria Monocytogenes
Meningo-encephalitis: common Immunocompromised & debilitated individuals In new born, well known and often fatal CSF – pleocytosis (initially polymorphonuclear) Rarely normal CSF Rhombencephalitis
 Rarely normal CSF. Rhombencephalitis.")
23
Listeria Early CT scan normal Multiple abscesses in the brain
Monocytosis

24
CNS Infections Meninges and subarachnoid space can be infected by viruses, bacteria, spirochaetes and fungi Virus and bacteria: seasonal variation Classic case unmistakable But subtle presentations can lead to fatal delay in diagnosis

25
Typical acute meningitis
Pyrexia Severe headache Phtophobia Rapid development of neck stiffness Kernig’s sign, Brudzinski sign If untreated vomiting, drowsiness and eventually coma

26
Viral causes Meningitis Encephalitis Entero ((Echo,polio, coxsackie)
HSV2 Lymphocytic choriomeningitis VZ Mumps HIV Encephalitis HSV VZ CMV EBV HIV Mumps Measles Rabies Arbo

27
Typical Cerebrospinal Fluid Findings in Various Types of Meningitis
Test Bacterial Viral Fungal Tubercular Opening pressure Elevated Usually normal Variable Variable WBC ≥1,000 per mm3 <100 per mm3 Variable Variable Cell differential Predominance of Predominance of Predominance Predominance PMNs* lymphocytes† of lymphocytes of lymphocytes Protein Mild to marked Normal to elevated Elevated Elevated elevation CSF-to-serum glucose Normal to marked Usually normal Low Low ratio decrease CSF = cerebrospinal fluid; PMNs = polymorphonucleocytes. *—Lymphocytosis present 10 percent of the time. †—PMNs may predominate early in the course.

Similar presentations