Download presentation
Presentation is loading. Please wait.

2
Speaker: Decca Mohammed, MD

3
Statistics for cervical cancer and HPV Association of HPV to cervical cancer, and other cancers Prevention Screening Recommendations

4
12,000 women in the U.S. get cervical cancer in 2009 4000 women died from it in the U.S. in 2009 It is the most common cause of cancer death in the world where pap tests are not available (240,000 deaths annually) It is the easiest gynecologic cancer to prevent cdc.gov
 It is the easiest gynecologic cancer to prevent cdc.gov.")
5
SEER STAT FACT Sheets: Cervix Uteri;http://seer.cancer.gov/statfacts/html/cervix.html.sept 19,2011 2.Cancer incidence and mortatility in NJ 2004- 2008;http://www.state.nj.us/health/ces/documents/report04-08.pdf; sept 19,2011 3.Cancer incidence rates in NJ’sTen Most Populated Municipalities 1998- 2002;http://www.nj.gov/health/ces/documents/cancer municipalities.pdf; sept 19,2011 Cervical cancer rates -US: 2004-2008 age adjusted incidence rate of 8.1/100,000 population 1 -NJ:2004-2008 age adjusted incidence rate of 9/100,000 population 2 -Newark:1998-2002 age adjusted incidence rate of 17,.6/100,000 population 3

6
Persistent high risk HPV infection Early onset of sexual activity Multiple sexual partner History of STI Smoking Immunosuppression High parity Low socioeconomic status

7
Abnormal vaginal bleeding Post-coital bleeding Malodorous vaginal discharge

8
Estimated incidence-6.2 million women/yr Estimated prevalence-20 million women 9.2 million women age 15-24 yrs are infected currently cdc.gov

9
HPV DNA is found in almost 99% of cervical cancer High risk HPV (ie.16,18,31,33,45) detected in 70% of invasive cervical cancer cases worldwide Persistent infection with HPV is a prerequisite for getting cervical cancer or its precursor cell
 detected in 70% of invasive cervical cancer cases worldwide Persistent infection with HPV is a prerequisite for getting cervical cancer or its precursor cell")
10
% HPV association Cervix96 Oropharynx63 Anus93 Vulva51 Vagina64 Penis Gillison ML Cancer Suppl 2008;113(10):3036-46 36
:")
11
1.http:/www.cancer.org/cancer/analcancer/detailedguide/a nal-cancer-what-is-key-statistics, sept 19,2011 2.Seer stat fact sheets, anal cancer;http://seer.cancer.gov/statfacts/html/anus.html; sept 19,2011 Estimated 5820 new cases of anal cancer in the US in 2011 -~3680 females -~2140 males 1 Between 1975-2008, the annual percentage change for cancer of the anus, anal canal, and anorectum was 2.2% 2 2.5%(males) 2.0%(females)
 2.0%(females)")
12
Non-enveloped double stranded DNA virus >100 types identified 30-40 anogenital types -15-20 oncogenic types, ie 16,18,31,33,45 (HPV 16 and 18 account for the majority of worldwide cervical cancers) -Non-oncogenic types are associated with genital warts, ie HPV 6 and HPV11 cdc.gov
 -Non-oncogenic types are associated with genital warts, ie HPV 6 and HPV11 cdc.gov")
13
Direct sexual contact -condoms may not prevent HPV infection but may protect against HPV related diseases(warts, cancers, pre-cancer cell) Non-sexual routes -mother to newborn(respiratory papillomatosis) -fomites (ie undergarments)
 Non-sexual routes -mother to newborn(respiratory papillomatosis) -fomites (ie undergarments)")
14
Most HPV infections are cleared by 1-2yrs 60-70% will be cleared by 1 yr 90% will be cleared by 3 yrs The longer the HR HPV infection persists, the greater the risk for cervical cancer precursor formation cdc.gov

15
Quadrivalent vaccine (types 6,11,16, &18) -approved by FDA for females age 9-26yrs for the prevention of cervical, vulvar and vaginal cancer cause(2006) -approved by FDA for use in males age 9- 26yrs for the prevention of genital warts caused by HPV types 6 & 11 Bivalent vaccine (type16,18)-2009 cdc.gov
 -approved by FDA for females age 9-26yrs for the prevention of cervical, vulvar and vaginal cancer cause(2006) -approved by FDA for use in males age 9- 26yrs for the prevention of genital warts caused by HPV types 6 & 11 Bivalent vaccine (type16,18)-2009 cdc.gov")
16
Annual pap smear starting at age 21 Pap smear every 2-3yrs at age 30 if three consecutive negative pap smears HPV testing with pap smear after age 30 HPV testing earlier if abnormal pap smear ACOG recommendation

17
No pap smear Counseling about safe sex practice and contraception Counseling and testing for sexually transmitted diseases No speculum exam if pt is asymptomatic ACOG practice bulletin No.109

18
18 yrs young lady, never pregnant, has never had sexual activity comes for annual gyn exam. -no pap smear -no speculum -no HPV testing -HPV vaccine -counseling 16 y/o young lady, 2pregnancy, 1 abortion, comes to see gyn for vaginal discharge -no pap smear -+speculum -+STI screening -no HPV testing -HPV vaccine -counseling

19
27 y/o lady,2 children, for annual gyn exam -pap smear -no HPV HR unless pap shows precursor cells -no vaccine -STI screening 44 y/o lady, 4 children, for annual gyn exam -pap smear with HPV -no pap if last 3 consecutive paps neg. -no vaccine

20
Specimen adequacy- transformation zone must be present Negative for intraepithelial lesion or malignancy Squamous cells (ASC-US, ASC-H, LSIL,HSIL, Squamous Cell Ca, Glandular cell abnormalities)
")
21
www.asccp.org

22
HPV HR + HPV HR - ↓ Colposcopy ↓ Repeat pap in 4-6 mos

23
↓ Colposcopy

24
↓ Colposcopy HPV testing not needed

25
↓ Colposcopy or LEEP HPV testing not needed

26
Cervical cancer still affects thousands of women Millions more are impacted by the HPV related precursor cells Excellent preventive advances 1.vaccines 2.screening with pap and HPV(when indicated) 3.treatment of precursor cells
 3.treatment of precursor cells")
27
Hepatitis B Virus and Cancer Everett Schlam, MD 9/22/2011

28
Pick any number between 2 and 10 Multiply that number x 9 Add the two digits of that number together Subtract 5 from that number Pick the letter which corresponds to that number in the alphabet Ie, A=1 B=2 C=3 D=4 Pick a country which begins with that letter. Now take the second letter of that country and choose a large animal which begins with that letter

30
Viral Hepatitis 5 types: A : fecal-oral transmission B : sexual fluids & blood to blood C : blood to blood D : travels with B E : fecal–oral transmission Vaccine Preventable Adapted from Corneil, 2003

31
Hepatitis B Epidemic jaundice described by Hippocrates in 5th century BC Jaundice reported among recipients of human serum and yellow fever vaccines in 1930s and 1940s Australia antigen described in 1965 Serologic tests developed in 1970s

32
Hepatitis B Complications Fulminant hepatitis Hospitalization Cirrhosis Hepatocellular carcinoma Death

33
Hepatitis B Virus Infection More than 350 million chronically infected worldwide Established cause of chronic hepatitis and cirrhosis Human carcinogen—cause of up to 80% of Hepatocellular carcinomas More than 600,000 deaths worldwide in 2002

35
Natural History of Hep C Adapted from Lauer and Walker, NEJM 2001 Healthy Liver Acute Infection Chronic Infection 20% Clear the Virus 80% Virus Continues to Damage Liver Only 20% will show symptoms Initially !

36
Natural History Con’t Chronic Hepatitis Cirrhosis 20-30% Liver Cancer 1-4%/year Most symptoms begin to show only when liver is more severely damaged

37
Factors Affecting Progression 30yrs or longer if: Young at time of infection Healthy liver at time of infection Female 20yrs or less if: Drinking alcohol Co-infection (HIV, Hep B) Damaged liver before infection Adapted from Bigham, BC Hepatitis Services 2002
 Damaged liver before infection Adapted from Bigham, BC Hepatitis Services 2002")
38
Risk Factors HCV-infected household member/sexual partner (7%) Tattooing piercing (6%) Hospitalization dental work (6%) Transfusion/dialysis blood contact (4%) Incarceration (3%) No RF identified (23%) IDU/snorting (51%) Source: Health Canada Enhanced Surveillance, Oct 98-Oct 99, Calgary, Edmonton, Winnipeg, Ottawa
 Tattooing piercing (6%) Hospitalization dental work (6%) Transfusion/dialysis blood contact (4%) Incarceration (3%) No RF identified (23%) IDU/snorting (51%) Source: Health Canada Enhanced Surveillance, Oct 98-Oct 99, Calgary, Edmonton, Winnipeg, Ottawa")
39
Hepatitis C Affects each person differently No vaccine available Many people have the virus and do not even know it *BC Hepatitis Service 2003 Overall cure rate with new treatment is 55% *

40
Hepatitis C Dispelling Myths Hepatitis C is not spread by: –Casual contact –Hugging/kissing –Sharing eating utensils and drinking glasses –Sneezing/coughing –Shaking hands –Sitting on a toilet seat

41
HBV Disease Burden in the United States Pre-vaccine era –estimated 300,000 persons infected annually, including 24,000 infants and children 2005 –estimated 51,000 infections –Overall cure rate about 55%

42
Hepatitis B Perinatal Transmission* If mother positive for HBsAg and HBeAg –70%-90% of infants infected –90% of infected infants become chronically infected If positive for HBsAg only –5%-20% of infants infected –90% of infected infants become chronically infected *in the absence of postexposure prophylaxis

43
Who should be vaccinated with Hepatitis B Vaccine ?

44
Strategy to Eliminate Hepatitis B Virus Transmission—United States Prevent perinatal HBV transmission Routine vaccination of all infants Vaccination of children in high-risk groups Vaccination of adolescents Vaccination of adults in high-risk groups

45
Risk Factors for Hepatitis B CDC Sentinel Sites. 2001 data.

46
Hepatitis B Vaccine Long-term Efficacy Immunologic memory established following vaccination Exposure to HBV results in anamnestic anti-HBs response Chronic infection rarely documented among vaccine responders

47
Adults at Risk for HBV Infection Sexual exposure –sex partners of HBsAg-positive persons –sexually active persons not in a long-term, mutually monogamous relationship* –persons seeking evaluation or treatment for a sexually transmitted disease –men who have sex with men *persons with more than one sex partner during the previous 6 months

48
Adults at Risk for HBV Infection Percutaneous or mucosal exposure to blood –current or recent IDU –household contacts of HBsAg-positive persons –residents and staff of facilities for developmentally disabled persons –healthcare and public safety workers with risk for exposure to blood or blood-contaminated body fluids –persons with end-stage renal disease

49
Who should have Hepatitis B screening Tests?

50
Prevaccination Serologic Testing Not indicated before routine vaccination of infants or children Recommended for –all persons born in Africa, Asia, the Pacific Islands, and other regions with HBsAg prevalence of 8% or higher –household, sex, and needle-sharing contacts of HBsAg-positive persons –HIV-infected persons Consider for –Groups with high risk of HBV infection (MSM, IDU, incarcerated persons)
")
51
What are the recommended serological screening tests for Hepatitis B?

52
Screening Tests for Hepatitis B HBsAg Anti-HBs Cost for both tests about (150-250 dollars) Further testing and treatment determined by results of HBsAG and Anti-HBs
 Further testing and treatment determined by results of HBsAG and Anti-HBs")
53
Chronic Inactive Hepatitis B Infection Surveillance monitoring for reactivation

54
Chronic Active Hepatitis B Treatment Options Interferons –Interferon alfa-2b –Peginterferon alfa 2-b Nucleotids(t)ide analogs –Lamivudine –Adenovir –Entecavir –Telbivudine –Tenofovir
ide analogs –Lamivudine –Adenovir –Entecavir –Telbivudine –Tenofovir")
56
Who is post vaccination serological testing recommended for and when should the testing be performed?

57
Postvaccination Serologic Testing Not routinely recommended following vaccination of infants, children, adolescents, or most adults Recommended for: –Infants born to HBsAg+ women –Hemodialysis patients –Immunodeficient persons –Sex partners of persons with chronic HBV infection –Certain healthcare personnel

58
Postvaccination Serologic Testing Healthcare personnel who have contact with patients or blood should be tested for anti-HBs (antibody to hepatitis B surface antigen) 1 to 2 months after completion of the 3-dose series
 1 to 2 months after completion of the 3-dose series")
59
Management of Nonresponse to Hepatitis B Vaccine Complete a second series of three doses Should be given on the usual schedule of 0, 1 and 6 months Retest 1-2 months after completing the second series

60
Persistent Nonresponse to Hepatitis B Vaccine Less than 5% of vaccinees do not develop anti-HBs after 6 valid doses May be nonresponder or "hyporesponder" Check HBsAg status If exposed, treat as nonresponder with postexposure prophylaxis

61
Needle Prick 1.Do not “milk” prick site 2.Wash the area with soap and water 3.Go to nearest emergency department for assessment and treatment

62
Chronic Hepatitis B and risk of Hepatocellular Cancer Hepatocellular Cancer occurs in up to 25% of men and 15% of women over their lifetimes

63
Hepatitis B and Cancer Hepatocellular Cancer is a devastating complication of Hepatitis B Prevention is the optimal strategy to prevent acquisition of Hepatitis B Immunization and avoidance of high risk activities are of upmost importance

64
Questions??

65
Special Symposium of the Essex County Cancer Coalition September 22, 2011 Can Sex Lead to Cancer? HIV/AIDS and Cancer Drugs and Cancer

66
Presented by: Stanley H. Weiss, M.D. Professor of Preventive Medicine and Community Health, UMDNJ-New Jersey Medical School Professor of Quantitative Methods, School of Public Health Director, Essex County Cancer Coalition 30 Bergen Street Bldg. ADMC 16, Room 1614 Tel: (973) 972-4623 weiss@umdnj.edu www.umdnj.edu/esscaweb © 2011, SH Weiss. All rights reserved. www.umdnj.edu/esscaweb
 © 2011, SH Weiss. All rights reserved.")
67
(c) Stanley H. Weiss MD. Newark NJ66 Sexually transmitted infection and diseases (STI’s & STD’s) What is special about STI’s and STD’s as compared to other infectious agents/diseases?
 What is special about STI’s and STD’s as compared to other infectious agents/diseases .")
68
(c) Stanley H. Weiss MD. Newark NJ67 Sexually transmitted infection and diseases (STI’s & STD’s) “Sex” and Sexual Practices o Reluctance to discuss with partner History may be unknown, even if discussed, or misrepresented o Intimate behavior: Lesions may not be seen Lighting Sexual practices o Infected person may not even know o Reluctance to discuss with healthcare provider, and vice-versa
 Sex and Sexual Practices o Reluctance to discuss with partner History may be unknown, even if discussed, or misrepresented o Intimate behavior: Lesions may not be seen Lighting Sexual practices o Infected person may not even know o Reluctance to discuss with healthcare provider, and vice-versa.")
69
(c) Stanley H. Weiss MD. Newark NJ68 Sexually transmitted infection and diseases (STI’s & STD’s) Lack of immune protection Persistence of certain agents Continual susceptibility to others Lack of vaccines Limitations of barrier methods
 Lack of immune protection Persistence of certain agents Continual susceptibility to others Lack of vaccines Limitations of barrier methods.")
70
HIV/AIDS

71
HHuman IImmunodeficiency VVirus

72
A Acquired IImmuno D Deficiency S Syndrome

73
Once a person is infected they are always infected Medications are available to prolong life but they do not cure the disease Those who are infected are capable of infecting others without having symptoms or knowing of the infection HIV AIDS

81
HIV and Cancer Risk People infected with HIV have a substantially higher risk of some types of cancer compared with uninfected people of the same age. They also often have a multiplicity of other cancer risk factors.

82
HIV’s Effect on Cancer Risks Three cancers are known as “acquired immunodeficiency syndrome AIDS-defining cancers” or “AIDS-defining malignancies”; a diagnosis of any of these marks that HIV infection has progressed to AIDS. Cancer Increased Risk* Kaposi’s sarcoma (KS)> 1,000 Primary CNS lymphoma≈ 1,000 Non-Hodgkin’s lymphoma (NHL) 23-70 Invasive cervical cancer 5 * Standardized incidence ratio (SIR)
> 1,000 Primary CNS lymphoma≈ 1,000 Non-Hodgkin’s lymphoma (NHL) Invasive cervical cancer 5 * Standardized incidence ratio (SIR).")
83
HIV’s Effect on Cancer Risks In addition, people infected with HIV are at higher risk of several other types of cancer, including: Cancer Increased Risk (SIR) Anal20-25 Hodgkin’s lymphoma (HL)10-14 Liver5 Penis8 Lung3 Larynx3 Mouth or pharynx2
 Anal20-25 Hodgkin’s lymphoma (HL)10-14 Liver5 Penis8 Lung3 Larynx3 Mouth or pharynx2")
84
HIV’s Effect on Cancer Risks No evidence of increased risk of these other common cancers: Breast Prostate Colorectal Among the non-AIDS defining tumors, the most common overall in HIV-infected patients is lung cancer because it has a high underlying incidence in the general population.

85
HIV’s Effect on Cancer Risks Infection with HIV weakens the immune system and reduces the body's ability to fight infections that may lead to cancer. Many infected with HIV are also infected with other viruses that cause certain cancers. The most important of these cancer-related viruses: …

86
HIV’s Effect on Cancer Risks Human herpesvirus 8 (HHV-8), also known as Kaposi sarcoma- associated herpesvirus (KSHV), is the cause of Kaposi sarcoma. Epstein Barr virus (EBV) causes some subtypes of non-Hodgkin and Hodgkin lymphoma. Human papillomavirus (HPV) causes cervical cancer and some types of anal, penile, vaginal, vulvar, oropharyngeal and head and neck cancer. Hepatitis B virus (HBV) and hepatitis C virus (HCV) both can cause liver cancer. Human T-cell lymphotropic Virus Type I (HTLV-I), which causes adult T-cell lymphoma; this virus and this disease are rare in the U.S. … Infection with most of these viruses is more common among people infected with HIV than among HIV-uninfected people.
 causes some subtypes of non-Hodgkin and Hodgkin lymphoma. Human papillomavirus (HPV) causes cervical cancer and some types of anal, penile, vaginal, vulvar, oropharyngeal and head and neck cancer. Hepatitis B virus (HBV) and hepatitis C virus (HCV) both can cause liver cancer. Human T-cell lymphotropic Virus Type I (HTLV-I), which causes adult T-cell lymphoma; this virus and this disease are rare in the U.S. … Infection with most of these viruses is more common among people infected with HIV than among HIV-uninfected people..")
87
HIV’s Effect on Cancer Risks Some traditional risk factors for cancer, especially smoking (a known cause of lung cancer) and heavy alcohol use (which can increase the risk of liver cancer), are higher among people infected with HIV.
 and heavy alcohol use (which can increase the risk of liver cancer), are higher among people infected with HIV.")
88
HIV’s Effect on Cancer Risks The introduction of highly active antiretroviral therapy (HAART) in the mid-1990s greatly reduced the incidence of Kaposi sarcoma and non-Hodgkin lymphoma among people infected with HIV. HAART lowers the amount of HIV circulating in the blood, thereby allowing partial restoration of immune system function.

89
HIV’s Effect on Cancer Risks The incidence of several other cancers, particularly Hodgkin’s lymphoma and anal cancer, has been increasing among HIV-infected individuals since the introduction of HAART. The influence of HAART on the risk of these other cancer types is not well understood. The higher incidence of liver cancer among HIV- infected people appears to be related to more frequent infection with hepatitis virus (particularly HCV) and alcohol abuse or dependence than among uninfected people.
 and alcohol abuse or dependence than among uninfected people..")
90
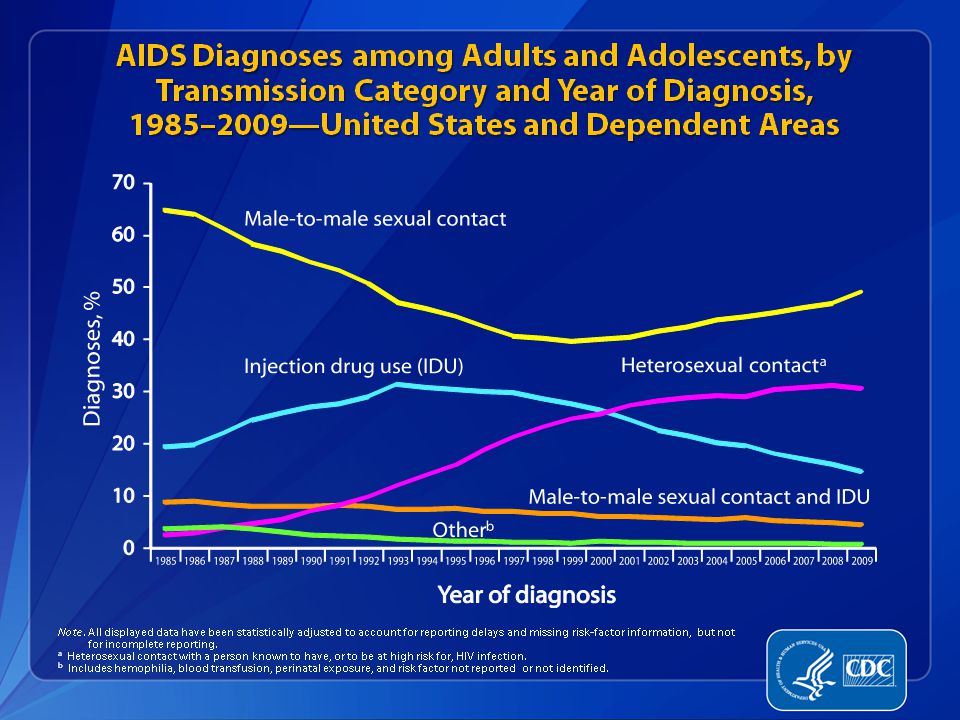
Routes of Transmission of HIV Sexual Contact:Male-to-male Male-to-female Female-to-male Female-to-female Blood Exposure: Injecting drug use/needle sharing Occupational exposure Transfusion of (unscreened) blood products Perinatal: Transmission from mother to neonate Breastfeeding
 blood products Perinatal: Transmission from mother to neonate Breastfeeding")
91
HIV Transmission HIV Parenteral Transmission HIV enters the bloodstream through: – Direct injection – Open cuts – Breaks in the skin – Breaks in mucous membranes – Examples: IDU/contaminated paraphernalia sharps & needlestick exposures prior to screening: blood products (risk is now rare in developed countries due to screening)
")
92
Comparative transmission risks for HIV, HBV and HCV, from a needlestick with blood contaminated with that agent Agent Percutaneous Exposure Transmission Risk (Range) HIV 0.3% (95% CI 0.2–0.5%) HCV 1.8% (range 0–7%) HBV, HBsAg +, Serologic: 23–37% HBeAg negative Clinical hepatitis: 1–6% HBV, HBsAg +, Serologic: 37–62% HBeAg positive Clinical hepatitis: 22–31%
 HIV 0.3% (95% CI 0.2–0.5%) HCV 1.8% (range 0–7%) HBV, HBsAg +, Serologic: 23–37% HBeAg negative Clinical hepatitis: 1–6% HBV, HBsAg +, Serologic: 37–62% HBeAg positive Clinical hepatitis: 22–31%")
93
HIV Transmission HIV Sexual Transmission – From a person infected with HIV to an uninfected person (discordant pair) Anal Genital Oral (rare)
 Anal Genital Oral (rare)")
94
HIV Transmission Body fluids that are a frequent source of transmission: – Blood – Semen – Vaginal Secretions – Breast Milk

95
HIV in Body Fluids Semen 11,000 Vaginal Fluid 7,000 Blood 18,000 Amniotic Fluid 4,000 Saliva 1 Average number of HIV particles in 1 ml of these body fluids

96
HIV Transmission Risk Varies with the Sexual Act (1) Highest Lowest Receptive partner, anal intercourse Insertive partner, anal intercourse Penile-vaginal: greater risk to women than to men Orogenital When the Partners are HIV Discordant:
 Highest Lowest Receptive partner, anal intercourse Insertive partner, anal intercourse Penile-vaginal: greater risk to women than to men Orogenital When the Partners are HIV Discordant:")
97
HIV Transmission Risk Varies with the Sexual Act (2) Known modulating factors: – STI co-infection: ↑ in transmission rate – STI infection: ↑ receptivity rate – Degree of HIV viremia – HAART: ↓ viral titer → ↓ transmission – Barrier methods
 Known modulating factors: – STI co-infection: ↑ in transmission rate – STI infection: ↑ receptivity rate – Degree of HIV viremia – HAART: ↓ viral titer → ↓ transmission – Barrier methods")
98
HIV Transmission Risk Varies with the Sexual Act (3) Possible modulating factors – Rough sex Increased mucosal injury Condom breakage – Blood exposure – ? Intercourse during menses ?

99
Understanding changing epidemiologic patterns: unifying concepts and examples [9] HOMOSEXUALITY & BISEXUALITY “Do you have sex only with men, only with women, or with both?” Specific sexual practices with same- and/or opposite-sex partners Specific sexual practices may be associated with specific problems
![Understanding changing epidemiologic patterns: unifying concepts and examples [9] HOMOSEXUALITY & BISEXUALITY Do you have sex only with men, only with women, or with both Specific sexual practices with same- and/or opposite-sex partners Specific sexual practices may be associated with specific problems](http://images.slideplayer.com/12/3502192/slides/slide_99.jpg "Understanding changing epidemiologic patterns: unifying concepts and examples [9] HOMOSEXUALITY & BISEXUALITY Do you have sex only with men, only with women, or with both Specific sexual practices with same- and/or opposite-sex partners Specific sexual practices may be associated with specific problems")
100
“When you have sex with someone, you are having sex with everyone they have had sex with for the last ten years.” Former Surgeon General C. Everett Koop

101
Understanding changing epidemiologic patterns: unifying concepts and examples [5] The incidence of reported non-monogamy among married couples over time is highly relevant to issues of genetic disease and the utility of a "family history" TABLE: reported rates
![Understanding changing epidemiologic patterns: unifying concepts and examples [5] The incidence of reported non-monogamy among married couples over time is highly relevant to issues of genetic disease and the utility of a family history TABLE: reported rates](http://images.slideplayer.com/12/3502192/slides/slide_101.jpg "Understanding changing epidemiologic patterns: unifying concepts and examples [5] The incidence of reported non-monogamy among married couples over time is highly relevant to issues of genetic disease and the utility of a family history TABLE: reported rates")
102
Incidence of NON-monogamy among MARRIED Heterosexual Couples [6]
![Incidence of NON-monogamy among MARRIED Heterosexual Couples [6]](http://images.slideplayer.com/12/3502192/slides/slide_102.jpg "Incidence of NON-monogamy among MARRIED Heterosexual Couples [6]")
103
Prevention Issues Physician awareness; earlier diagnosis Contact tracing Accessibility of healthcare Need for vaginal microbicides Targeted interventions Reportable diseases – statistics in CDC MMWR tables

104
Prevention Issues Safer sex issues: relative risks of sexual practices types of condoms latex, natural “skin” "female condom” lubrication issues (water-based) vaseline, etc. disrupt latex spermicidals (protection vs. irritation/inflammation)
.")
105
Barrier Methods: Condoms Using condoms is not 100 percent effective in preventing transmission of sexually transmitted infections, including HIV Condoms = Safer sex Condoms ≠ Safe sex

106
Condom Use Should be used consistently and correctly Should be either latex or polyurethane Should be discussed with your partner before the sexual act begins Should be the responsibility of both partners for the protection of both partners Male and female condoms are available

107
Condom Efficacy — Limitations (1) Need to put it on properly and in advance of first penetration – Pre-ejaculate emission Psychological issues, including failure to ultimately use Expiration date and storage issues Breakage – Right lubricant – “Rough” sex – Anorectal sex
 Need to put it on properly and in advance of first penetration – Pre-ejaculate emission Psychological issues, including failure to ultimately use Expiration date and storage issues Breakage – Right lubricant – Rough sex – Anorectal sex")
108
Condom Efficacy — Limitations (2) Initial trials of anti-microbial agents and spermicides led to increased HIV transmission rates. – Perhaps due to inflammation – Frequency of use of vaginal antimicrobials and spermicides might be relevant to this increased risk

109
People Infected with HIV Can look healthy Can be unaware of their infection Can live long productive lives when their HIV infection is managed Can infect people when they engage in high-risk behavior

110
HIV Exposure and Infection Some people have had multiple exposures without becoming infected Some people have been exposed one time and become infected

111
HIV and Sexually Transmitted Infections STI’s increase infectivity of HIV – A person co-infected with an STI and HIV may be more likely to transmit HIV due to an increase in HIV viral shedding – More white blood cells, some carrying HIV, may be present in the mucosa of the genital area due to a sexually transmitted infection

112
HIV and Sexually Transmitted Infections STI’s increase the susceptibility to HIV – Ulcerative and inflammatory STI’s compromise the mucosal or cutaneous surfaces of the genital tract that normally act as a barrier against HIV – Ulcerative STI’s include: syphilis, chancroid, and genital herpes – Inflammatory STI’s include: chlamydia, gonorrhea, and trichomoniasis

113
HIV and Sexually Transmitted Infections The effect of HIV infection on the immune system increases the risk of STI’s A suppressed immune response due to HIV can: I ncrease the reactivation of genital ulcers Increase the rate of abnormal cell growth Increase the difficulty in curing reactivated or newly acquired genital ulcers Increase the risk of becoming infected with additional STI’s

114
SUMMARY: Some issues that were covered were: “HIV/AIDS and Cancer” HIV and AIDS overview of epidemiology HIV and Cancer: Types of cancer, multiplicity of high risk exposures Transmission issues including from men to men and men to women Riskiness of various sexual practices - including to the receptive versus insertive partner (some discussion of rank order of risks), and modification with barriers (condom). Impact of HAART on decreasing transmission of HIV, and on course of HIV infection including on risk of cancer The relationship between cancers and HIV: what is well established - what is suspected; co-factors Human T-cell lymphotropic virus type I (HTLV-I) and adult T-cell leukemia/lymphoma (ATL); HTLV-II “Drugs and Cancer” Spread of HBV, HCV, HIV by injection drug use; also risks from needle sticks. Tobacco and cofactor issues.
 and adult T-cell leukemia/lymphoma (ATL); HTLV-II Drugs and Cancer Spread of HBV, HCV, HIV by injection drug use; also risks from needle sticks. Tobacco and cofactor issues..")
115
References Selected References Grulich AE, van Leeuwen MT, Falster MO, Vajdic CM. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: a meta-analysis. Lancet 2007; 370(9581):59–67. [PubMed Abstract] [PubMed Abstract] Weiss SH, Saxinger WC, Rechtman D, et al. HTLV-III infection among health care workers: association with needle-stick injuries. JAMA 254:2089- 2093, 1985. Weiss SH, Cowan EP. “Laboratory detection of human retroviruses” (Chap 8, pp. 147-183). In: AIDS and Other Manifestations of HIV Infection, fourth edition, ed. Gary P. Wormser, Elsevier Science, London, 2004. Weiss SH, Leschek JD. “HIV era occupational exposures and risks” (Chap 30). In: AIDS and Other Manifestations of HIV Infection, fourth edition, ed. Gary P. Wormser, Elsevier Science, London, 2004. Engels EA, Biggar RJ, Hall HI, et al. Cancer risk in people infected with human immunodeficiency virus in the United States. International Journal of Cancer 2008; 123(1):187–194. [PubMed Abstract] [PubMed Abstract] Powles T, Macdonald D, Nelson M, Stebbing J. Hepatocellular cancer in HIV-infected individuals: tomorrow's problem? Expert Review of Anticancer Therapy 2006; 6(11):1553–1558. [PubMed Abstract] [PubMed Abstract] Angeletti PC, Zhang L, Wood C. The viral etiology of AIDS-associated malignancies. Advances in Pharmacology 2008; 56:509–557. [PubMed Abstract] [PubMed Abstract] Engels EA, Pfeiffer RM, Goedert JJ, et al. Trends in cancer risk among people with AIDS in the United States 1980–2002. AIDS 2006; 20(12):1645– 1654. [PubMed Abstract] [PubMed Abstract] Chaturvedi AK, Madeleine MM, Biggar RJ, Engels EA. Risk of human papillomavirus-associated cancers among persons with AIDS. Journal of the National Cancer Institute 2009; 101(16):1120–1130. [PubMed Abstract] [PubMed Abstract] Silverberg MJ, Abrams DI. AIDS-defining and non-AIDS-defining malignancies: cancer occurrence in the antiretroviral therapy era. Current Opinion in Oncology 2007; 19(5):446–451. [PubMed Abstract] [PubMed Abstract] Grogg KL, Miller RF, Dogan A. HIV infection and lymphoma. Journal of Clinical Pathology 2007; 60(12):1365–1372. [PubMed Abstract] [PubMed Abstract] Simard EP, Pfeiffer RM, Engels EA. Spectrum of cancer risk late after AIDS onset in the United States. Archives of Internal Medicine 2010; 170(15):1337–1345. [PubMed Abstract] [PubMed Abstract] Shiels MS, Pfeiffer RM, Engels EA. Age at cancer diagnosis among persons with AIDS in the United States. Annals of Internal Medicine 2010; 153(7):452–460. [PubMed Abstract] [PubMed Abstract] Spano JP, Costagliola D, Katlama C, et al. AIDS-related malignancies: state of the art and therapeutic challenges. Journal of Clinical Oncology 2008; 26(29):4834–4842. [PubMed Abstract] [PubMed Abstract] Heard I. Prevention of cervical cancer in women with HIV. Current Opinion in HIV and AIDS 2009; 4(1):68–73. [PubMed Abstract] [PubMed Abstract] Macdonald DC, Nelson M, Bower M, Powles T. Hepatocellular carcinoma, human immunodeficiency virus and viral hepatitis in the HAART era. World Journal of Gastroenterology 2008; 14(11):1657–1663. [PubMed Abstract] [PubMed Abstract] McGinnis KA, Fultz SL, Skanderson M, et al. Hepatocellular carcinoma and non-Hodgkin's lymphoma: the roles of HIV, hepatitis C infection, and alcohol abuse. Journal of Clinical Oncology 2006; 24(31):5005–5009. [PubMed Abstract] [PubMed Abstract] Massad LS, Seaberg EC, Wright RL, et al. Squamous cervical lesions in women with human immunodeficiency virus: long-term follow-up. Obstetrics and Gynecology 2008; 111(6):1388–1393. [PubMed Abstract] [PubMed Abstract] Goldie SJ, Kuntz KM, Weinstein MC, et al. The clinical effectiveness and cost-effectiveness of screening for anal squamous intraepithelial lesions in homosexual and bisexual HIV-positive men. Journal of the American Medical Association 1999; 281(19):1822–1829. [PubMed Abstract][PubMed Abstract] Weiss SH. Editorial: The evolving epidemiology of human T lymphotropic virus type II. The Journal of Infectious Diseases 169:1080-1083, 1994.
:59–67. [PubMed Abstract] [PubMed Abstract] Weiss SH, Saxinger WC, Rechtman D, et al. HTLV-III infection among health care workers: association with needle-stick injuries. JAMA 254: , Weiss SH, Cowan EP. Laboratory detection of human retroviruses (Chap 8, pp ). In: AIDS and Other Manifestations of HIV Infection, fourth edition, ed. Gary P. Wormser, Elsevier Science, London, Weiss SH, Leschek JD. HIV era occupational exposures and risks (Chap 30). In: AIDS and Other Manifestations of HIV Infection, fourth edition, ed. Gary P. Wormser, Elsevier Science, London, Engels EA, Biggar RJ, Hall HI, et al. Cancer risk in people infected with human immunodeficiency virus in the United States. International Journal of Cancer 2008; 123(1):187–194. [PubMed Abstract] [PubMed Abstract] Powles T, Macdonald D, Nelson M, Stebbing J. Hepatocellular cancer in HIV-infected individuals: tomorrow s problem. Expert Review of Anticancer Therapy 2006; 6(11):1553–1558. [PubMed Abstract] [PubMed Abstract] Angeletti PC, Zhang L, Wood C. The viral etiology of AIDS-associated malignancies. Advances in Pharmacology 2008; 56:509–557. [PubMed Abstract] [PubMed Abstract] Engels EA, Pfeiffer RM, Goedert JJ, et al. Trends in cancer risk among people with AIDS in the United States 1980–2002. AIDS 2006; 20(12):1645– [PubMed Abstract] [PubMed Abstract] Chaturvedi AK, Madeleine MM, Biggar RJ, Engels EA. Risk of human papillomavirus-associated cancers among persons with AIDS. Journal of the National Cancer Institute 2009; 101(16):1120–1130. [PubMed Abstract] [PubMed Abstract] Silverberg MJ, Abrams DI. AIDS-defining and non-AIDS-defining malignancies: cancer occurrence in the antiretroviral therapy era. Current Opinion in Oncology 2007; 19(5):446–451. [PubMed Abstract] [PubMed Abstract] Grogg KL, Miller RF, Dogan A. HIV infection and lymphoma. Journal of Clinical Pathology 2007; 60(12):1365–1372. [PubMed Abstract] [PubMed Abstract] Simard EP, Pfeiffer RM, Engels EA. Spectrum of cancer risk late after AIDS onset in the United States. Archives of Internal Medicine 2010; 170(15):1337–1345. [PubMed Abstract] [PubMed Abstract] Shiels MS, Pfeiffer RM, Engels EA. Age at cancer diagnosis among persons with AIDS in the United States. Annals of Internal Medicine 2010; 153(7):452–460. [PubMed Abstract] [PubMed Abstract] Spano JP, Costagliola D, Katlama C, et al. AIDS-related malignancies: state of the art and therapeutic challenges. Journal of Clinical Oncology 2008; 26(29):4834–4842. [PubMed Abstract] [PubMed Abstract] Heard I. Prevention of cervical cancer in women with HIV. Current Opinion in HIV and AIDS 2009; 4(1):68–73. [PubMed Abstract] [PubMed Abstract] Macdonald DC, Nelson M, Bower M, Powles T. Hepatocellular carcinoma, human immunodeficiency virus and viral hepatitis in the HAART era. World Journal of Gastroenterology 2008; 14(11):1657–1663. [PubMed Abstract] [PubMed Abstract] McGinnis KA, Fultz SL, Skanderson M, et al. Hepatocellular carcinoma and non-Hodgkin s lymphoma: the roles of HIV, hepatitis C infection, and alcohol abuse. Journal of Clinical Oncology 2006; 24(31):5005–5009. [PubMed Abstract] [PubMed Abstract] Massad LS, Seaberg EC, Wright RL, et al. Squamous cervical lesions in women with human immunodeficiency virus: long-term follow-up. Obstetrics and Gynecology 2008; 111(6):1388–1393. [PubMed Abstract] [PubMed Abstract] Goldie SJ, Kuntz KM, Weinstein MC, et al. The clinical effectiveness and cost-effectiveness of screening for anal squamous intraepithelial lesions in homosexual and bisexual HIV-positive men. Journal of the American Medical Association 1999; 281(19):1822–1829. [PubMed Abstract][PubMed Abstract] Weiss SH. Editorial: The evolving epidemiology of human T lymphotropic virus type II. The Journal of Infectious Diseases 169: ,")
116
Supplemental Material

118
Cancers developed do not necessarily contribute to the final cause of death because of competing risks of mortality from infection and other causes including treatment

119
HIV patients have an increased risk of developing malignancies besides KS. HAART has decreased AIDS related illnesses but has increased the number of people living with AIDS. HIV is not cured and this means a cumulative risk of developing malignancies.

120
HIV’s Effect on Cancer Risks Positron-emmission tomography (PET) scan of the head of a patient with HIV- associated central nervous system (CNS) lymphoma.
 scan of the head of a patient with HIV- associated central nervous system (CNS) lymphoma.")
121
Prognostic factors in HIV related malignancies Extent and bulk of tumour CD4 count (worse if less than 200) Weight loss of more than 10% over 6 months Night sweats
 Weight loss of more than 10% over 6 months Night sweats")
122
Understanding changing epidemiologic patterns: unifying concepts and examples [7] PROPAGATED SPREAD AND CHANGING PATTERNS: HIV and "THE AIDS BRIDGE"
![Understanding changing epidemiologic patterns: unifying concepts and examples [7] PROPAGATED SPREAD AND CHANGING PATTERNS: HIV and THE AIDS BRIDGE](http://images.slideplayer.com/12/3502192/slides/slide_122.jpg "Understanding changing epidemiologic patterns: unifying concepts and examples [7] PROPAGATED SPREAD AND CHANGING PATTERNS: HIV and THE AIDS BRIDGE")
123
The AIDS Bridge

124
Specific Tumors Kaposi’s Sarcoma – First described by Moriz Kaposi in 1872 on five patients presenting with ‘sarcoma idiopaticum multiple hemorrhagicum’ – In 1912 Sternberg termed this disease Kaposi’s sarcoma-now refered as classsical KS An indolent tumour seen typically in men of mediterranean or east European Jewish origin

125
In 1914 Hallenberg described the first case of African or endemic KS In 1960 the first report of KS following organ transplant and immuno-suppressive therapy In 1981 Hymes described the epidemic form associated with AIDS

126
Etiology and pathogenesis KS associated with gamma-2 herpes virus known as HHV-8(KSHV) Virus identified using PCR-based techniques in all forms of KS – Classical (especially occurred in certain ethnic groups) – Endemic African – Pediatric – Epidemic = HIV related
 Virus identified using PCR-based techniques in all forms of KS – Classical (especially occurred in certain ethnic groups) – Endemic African – Pediatric – Epidemic = HIV related")
127
HHV-8 transmitted in saliva In MSM rate of HHV-8 is related to the number of sexual partners Evidence from Africa on HHV-8 prevalence in children suggests infection is acquired there through normal social contacts within the family

128
In developed countries seroprevalence of HHV-8 in general population is between 5 and 15%. For HIV positive MSM it is 30% In Africa prevalence is higher and increases with age: – <2% under the age of 5; – 15% for ages between 15 and 40 and – >27% for older than 40

129
Action of HHV-8 in development of KS – Production of an analogue of cyclin D which increase the proportion of cycling cells – Production of a bcl-2 analogue(vbcl-2) and a protein (vFLIP) both which will prevent apoptosis – Stimulation of angiogenesis mediated by a G protein coupled receptor (GPCR) Production of angiogenic proteins which are also inhibitory to macrophages (vMIPs)
 and a protein (vFLIP) both which will prevent apoptosis – Stimulation of angiogenesis mediated by a G protein coupled receptor (GPCR) Production of angiogenic proteins which are also inhibitory to macrophages (vMIPs)")
130
Epidemiology of Epidemic KS Most frequent neoplasm in AIDS patients First malignancy to be described in AIDS Indirectly contributed to the identification of AIDS itself – A previously rare disease newly found to be occurring commonly and at an increasing rate: something unexpected was happening – Unexpected event was the HIV epidemic

131
KS Clinical Features Classic lesion of KS is a raised macule purplish in color Lesions may coalesce into plaques and may ulcerate and bleed KS may develop at sites of previous trauma Edema almost always a feature Visceral

132
Examples of KS lesions

134
Non-Hodgkin Lymphoma (NHL) Recognised as part of AIDS in 1982 Characteristically aggressive and often involve extra nodal sites
 Recognised as part of AIDS in 1982 Characteristically aggressive and often involve extra nodal sites")
135
Lymphomas develop against a background of chronic antigenic stimulation and most are of B-cell origin Cytokines stimulate expansion once malignant transformation has occurred(IL-6, TNF-beta and IL-10) Chemokines produced by HIV infected macrophages and monocytes produce autocrine stimulation of the abnormal clone
 Chemokines produced by HIV infected macrophages and monocytes produce autocrine stimulation of the abnormal clone")
136
Clinico-pathological categories of HIV related lymphomas Diffuse large cell lymphoma(DLCL) – Large non cleaved (LNCCL) – EBV 40% – Immunoblastic plasmacytoid (IBPL) 90% Burkitt’s lymphoma (BL) - EBV 30% Primary lymphomas of the central nervous system(PCNSL) - EBV 100% Primary effusion lymphomas (PEL) – EBV 90%, HHV-8 100%
 – Large non cleaved (LNCCL) – EBV 40% – Immunoblastic plasmacytoid (IBPL) 90% Burkitt’s lymphoma (BL) - EBV 30% Primary lymphomas of the central nervous system(PCNSL) - EBV 100% Primary effusion lymphomas (PEL) – EBV 90%, HHV-8 100%")
137
Degree and duration of HIV affects type of lymphoma that developes Primary CNS lymphomas are associated with profound immunosuppression and occur late in the course of HIV The other types may occur early

138
Epidemiology of AIDS-Associated Cancers Less than 5% AIDS defining diagnosis in developed countries, but cause 15% of AIDS related deaths (occurs late in the course) HAART has changed the pattern Extranodal lymphomas more common in AIDS patients
 HAART has changed the pattern Extranodal lymphomas more common in AIDS patients")
139
Clinical features Primary CNS – 75% develop in known AIDS patients – 50% have CD4 of less than 50/dl – Symptoms similar to SOL (headache, change in consciousness, focal neurological symptoms, visual disturbances) – Rapid onset and therefore difficult to differentiate from infection
 – Rapid onset and therefore difficult to differentiate from infection")
140
Nodal NHL including Burkitt’s – Wide spread nodal disease – Unusual nodal sites Occipital Epitrochlear parotid – Involvement of bone marrow present in 25% – Direct involvement of overlying skin

141
Gastrointestinal NHL – Tumours can be anywhere from posterior pharyngeal wall to rectum – Upper GIT present with dysphagia, nausea, vomiting, and anorexia – Small bowel lymphoma causes symptoms of malabsorption, weight loss and subacute obstruction

142
Rectal tumors will cause bleeding, discharge, change in bowel habit, pain and tenesmus Meningeal NHL – Cranial nerve palsies, backache, spinal root pain, confusion

143
Primary effusion lymphomas (body cavity lymphomas) – Pleural effusion or ascites without evidence of bulk disease – Thickening of pleural or peritoneal membranes with no evidence of tumour masses Symptoms are from accumulation of fluid – Dyspnea, chest or abdominal discomfort
 – Pleural effusion or ascites without evidence of bulk disease – Thickening of pleural or peritoneal membranes with no evidence of tumour masses Symptoms are from accumulation of fluid – Dyspnea, chest or abdominal discomfort")
144
Castleman’s disease – Multifocal lymphadenopathy with splenomegaly – Fever and splenomegaly are the cardinal features – Hepatomegaly, edema, cough,dyspnoea – Hypersplenism and anemia, leukopenia and thrombocytopenia

145
Diagnosis Biopsy CT or MRI for CNS +- biopsy

146
Cancer of the cervix Most common cancer in women in sub-Sahara Association with HIV noted in 1983 but criteria for defining AIDS were modified to include cervical cancer in 1993

147
Etiology and pathogenesis Human papilloma virus (HPV) 16 qnd 18 Risk factors – Low socio-economic status – First intercourse at early age – Sexual promiscuity – Large number of pregnancies – HIV
 16 qnd 18 Risk factors – Low socio-economic status – First intercourse at early age – Sexual promiscuity – Large number of pregnancies – HIV")
148
Clinical features Post coital bleeding Intermenstrual bleeding Excessive menstrual bleeding Fowl smelling discharge and backache are late symptoms Vesico-vaginal or recto-vaginal fistulae Metastasis

149
Cervical Cancer: Detection and Diagnosis PAP smear Colposcopy Biopsy

150
Other Tumors Conjunctival squamous cell carcinoma (SCC) A tumor of the thin membrane that covers the white of the eye Uncommon even in countries with high exposure to the sun, but incidence now manifests in epidemic – High incidence in sub-Sahara especially Uganda & Rwanda 2 tumors per million population from 1970 to 1988 Ten fold increase from 1988 to 1992 – Common in age group of 40 and above before the advent of HIV epidemic, but now shifted to 20s Associated with HIV Possible association with HPV
 A tumor of the thin membrane that covers the white of the eye Uncommon even in countries with high exposure to the sun, but incidence now manifests in epidemic – High incidence in sub-Sahara especially Uganda & Rwanda 2 tumors per million population from 1970 to 1988 Ten fold increase from 1988 to 1992 – Common in age group of 40 and above before the advent of HIV epidemic, but now shifted to 20s Associated with HIV Possible association with HPV")
151
Anal Cancer Incidence of premalignant lesions common in HIV patients Not an AIDS-defining illness but occurence in HIV warrants consideration in the context of HIV infection Etiology – HPV 16 18 31 33 35 45 51 52 56

Similar presentations