Download presentation
Presentation is loading. Please wait.

1
Neoplasia References: Pathologic Basis of Disease by Robbins and Cotran, 8th Ed. (2010)
")
2
Neoplasia (TUMOR) Definitions - “New growth” = Neoplasm - Tumor Oncology - Greek “oncos” = tumor - Study of tumors or neoplasms - Cancer = Malignant tumors
 Definitions - New growth = Neoplasm - Tumor Oncology - Greek oncos = tumor - Study of tumors or neoplasms - Cancer = Malignant tumors")
3
Neoplasia (TUMOR) Tumor - An abnormal mass of tissue - Growth exceeds that of normal tissues - Growth persists after cessation of the stimuli that initiated change - Classified: Benign vs. Malignant

4
What is the relationship of neoplasia to metaplasia and dysplasia?

5
Metaplasia -replacement of one type of cell with another type. found in association with tissue damage, repair, and regeneration. the replacing cell type is more suited to a change in environment

6
Dysplasia –means disordered growth. often occurs in metaplastic epithelium, but not all metaplastic epithelium is also dysplastic - characterized by changes that include a loss in the uniformity of the individual cells as well as a loss in their architectural orientation.

7
When dysplastic changes are marked and involve the entire thickness of the epithelium but the lesion remains confined by the basement membrane, it is considered a preinvasive neoplasm and is referred to as carcinoma in situ Once the tumor cells breach the basement membrane, the tumor is said to be invasive.

8
However, dysplasia does not necessarily progress to cancer. Mild to moderate changes that do not involve the entire thickness of epithelium may be reversible, and with removal of the inciting causes the epithelium may revert to normal. Even carcinoma in situ may take years to become invasive.

9
The growth of cancers is accompanied by progressive infiltration, invasion, and destruction of the surrounding tissue. Malignant tumors are poorly demarcated from the surrounding normal tissue.

10
Metaplasia and dysplasia are still forms of cellular adaptation in response to stress/injury. Neoplasia is not. However, metaplasia and dysplasia may lead to neoplasia.

11
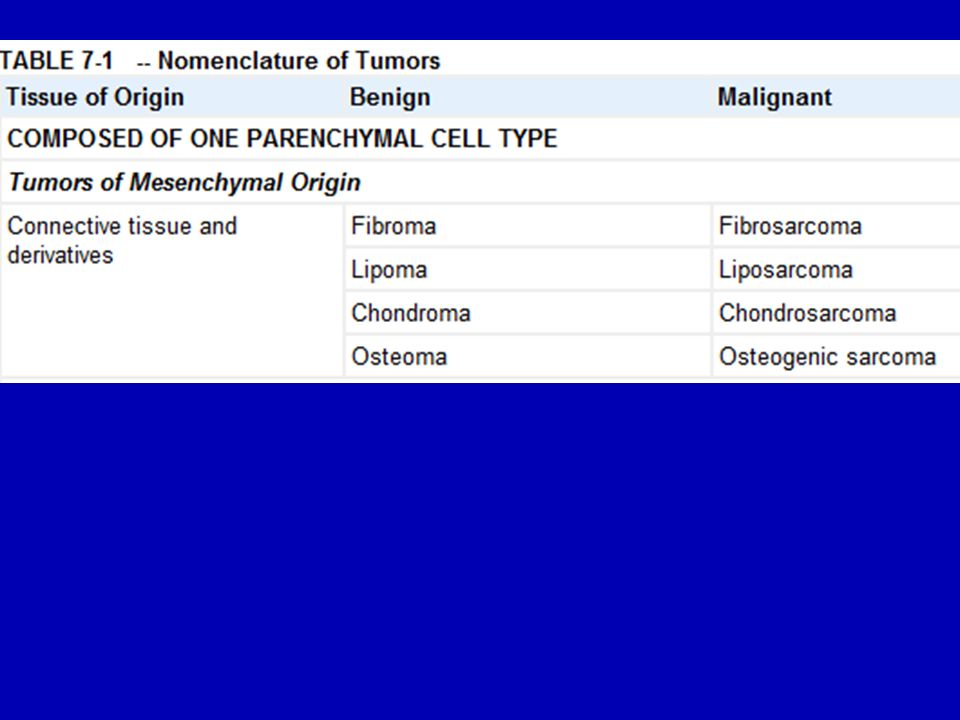
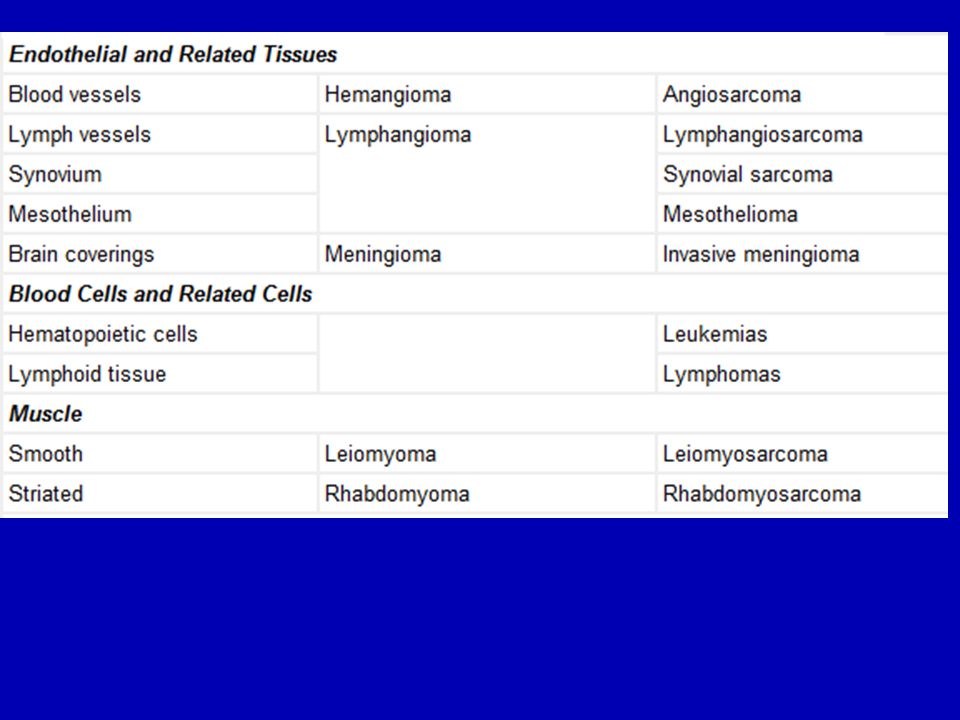
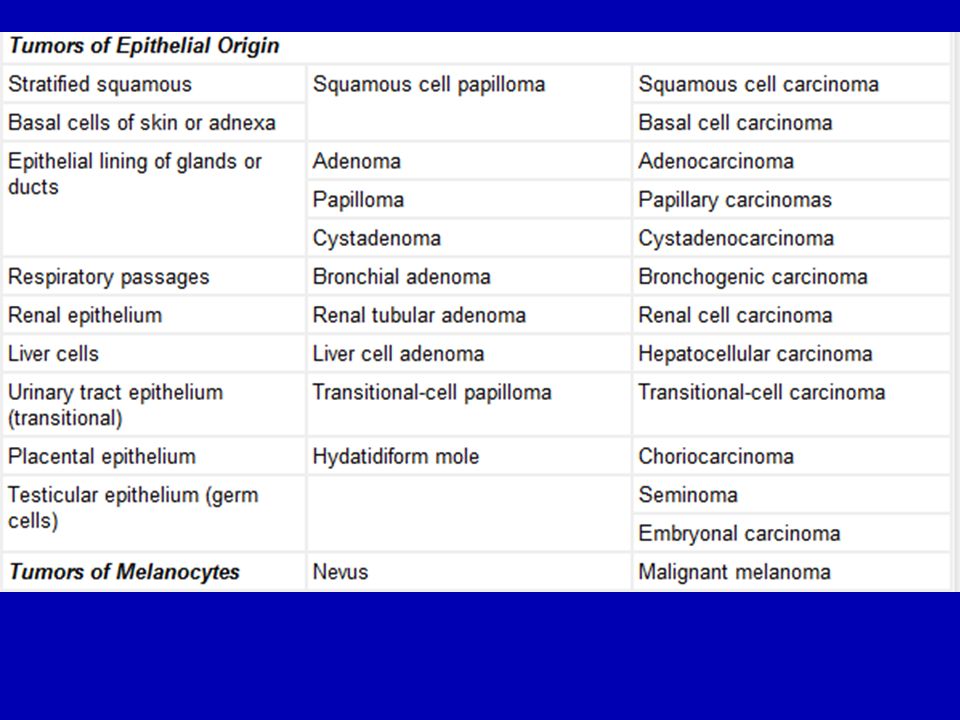
Table on Nomenclature of Tumors a. Origin b. Cell type c. Benign and Malignant types NEOPLASIA Nomenclature

16
2 Basic Components of Tumor The “transformed” neoplastic cells Parenchyma The nontransformed elements such as connective tissues & blood vessels Supporting stroma

17
Characteristics of Benign vs. Malignant Neoplasms Differentiation and Anaplasia Rate of Growth Local Invasion Metastasis

18
Differentiation & Anaplasia Parenchymal cells of neoplasms Differentiation - the extent to which parenchymal cells resemble comparable normal cells - morphologically & functionally

19
Differentiation Well-differentiated - resemble mature normal cells of the tissue origin Poorly differentiated (anaplastic) - Undifferentiated - primitive, unspecialized cells
 - Undifferentiated - primitive, unspecialized cells")
20
Differentiation All benign tumors - well-differentiated Malignant neoplasms - range from well-differentiated to undifferentiated

21
Anaplasia Definition - lack of differentiation - hallmark of malignant transformation - “ to form backward”

22
Lack of differentiation, or anaplasia, is often associated with many other morphologic changes.

23
Pleomorphism. Both the cells and the nuclei characteristically display pleomorphism—variation in size and shape. Cells within the same tumor are not uniform- some are large, some are small.

24
Abnormal nuclear morphology. nuclei contain abundant chromatin and are dark staining (hyperchromatic) nuclei are disproportionately large for the cell, and the nuclear-to-cytoplasm ratio may approach 1 : 1 instead of the normal 1 : 4 or 1 : 6. nuclear shape -variable and irregular
 nuclei are disproportionately large for the cell, and the nuclear-to-cytoplasm ratio may approach 1 : 1 instead of the normal 1 : 4 or 1 : 6. nuclear shape -variable and irregular.")
25
Mitoses undifferentiated tumors possess large numbers of mitoses, reflecting the higher proliferative activity of the parenchymal cells. The presence of mitoses, however, does not necessarily indicate that a tumor is malignant or that the tissue is neoplastic.

26
Loss of polarity anaplastic cells is markedly disturbed (i.e., they lose normal polarity). Sheets or large masses of tumor cells grow in an anarchic, disorganized fashion.

27
Other changes formation of tumor giant cells, some possessing only a single huge polymorphic nucleus and others having two or more large, hyperchromatic nuclei vascular stroma is scant, and in many anaplastic tumors, large central areas undergo ischemic necrosis.

28
Rate of Growth Most malignant tumors grow more rapidly than benign tumors Cancers from hormone sensitive tissues affected by hormone levels E.g. uterus Hormone dependence & adequacy of blood supply

29
Local Invasion Benign tumors - cohesive expansile masses with capsule - do not penetrate capsule & normal tissues - Discrete, readily palpable and easily movable mass - Surgically enucleated

30
Local Invasion Malignant tumors - Invasive, infiltrating and destroying normal tissues - Lack encapsulation - Enucleation is difficult - Surgery requires removal of some healthy, uninvolved tissues

31
Local Invasion Carcinoma in situ - Preinvasive stage - Cytologic features of malignancy without invasion of the basement membrane - e.g. carcinoma of uterine cervix

32
Metastasis Definition - This process involves invasion of the lymphatics, blood veseels and body cavities by the tumor - Tumor implants discontinuous with the primary tumor - Single most important feature that differentiates from benign tumors

33
Metastasis All cancers can metastasize Few and major exceptions: - Gliomas - Basal cell carcinomas of the skin The more aggressive, the more rapidly growing, the larger the primary neoplasm, the greater likelihood of metastasis

34
Pathways of Spread 1. Spread into body cavities 2. Invasion of lymphatics 3. Hematogenous spread

35
Seeding of body cavities and surfaces Occurs by seeding of surfaces in peritoneal, pleural, pericardial, subarachnoid and joint spaces Example: Carcinoma of the ovary

36
Lymphatic Spread Most common pathway for the initial dissemination of carcinoma Pattern of lymph node involvement follows the natural routed of drainage Lymph nodes are frequently enlarged

37
Hematogenous spread Typical of all sarcomas Favored route for some carcinoma e.g. Kidney (renal cell carcinoma) Veins are more frequently invaded than arteries Lung and liver are common sites Other sites:Brain and bones
 Veins are more frequently invaded than arteries Lung and liver are common sites Other sites:Brain and bones.")
38
Comparisons between benign and malignant tumors Differentiation/anaplasia Benign -well differentiated -structure typical of tissue of origin Malignant -lack of differentiation with anaplasia - structure often atypical

39
Comparisons between benign and malignant tumors Rate of growth Benign -usually progressive and slow -mitotic figures are rare and normal Malignant -erratic and maybe slow to rapid -mitotic figures maybe numerous and abnormal

40
Comparisons between benign and malignant tumors Local Invasion Benign -cohesive and espansile well demarcated masses -do not invade or infiltrate normal tissues Malignant -locally invasive, infiltrating surrounding normal tissues

41
Comparisons between benign and malignant tumors Metastasis Benign -absent Malignant -frequently present - More likely for larger and more undifferentiated masses

42
Grading and Staging of Cancer Grading - classified as grades I to IV with increasing anaplasia - higher grades tumors are more aggressive than lower grade tumors

43
Grade refers to the degree of differentiation of a neoplasm. Grade I (or well differentiated) neoplasms closely resemble the normal tissues from which they are derived. Grade IV(or poorly differentiated) only slightly resemble the tissues they are derived from. Patients with Grade IV tumors have a poorer prognosis than those with Grade I tumors.
 neoplasms closely resemble the normal tissues from which they are derived. Grade IV(or poorly differentiated) only slightly resemble the tissues they are derived from. Patients with Grade IV tumors have a poorer prognosis than those with Grade I tumors..")
44
Grading and Staging of Cancer Staging - (T) based on the size of the primary tumor - (N) extent of spread to regional lymph nodes - (M) presence and absence of blood-borne metastases - TNM system (tumor,node,metastases) - Higher stages -larger, locally invasive, metastatic tumors
 based on the size of the primary tumor - (N) extent of spread to regional lymph nodes - (M) presence and absence of blood-borne metastases - TNM system (tumor,node,metastases) - Higher stages -larger, locally invasive, metastatic tumors")
45
Staging (TNM system) - T1 to T4 (increasing size) - N0 ( no nodal involvement) N1 to N3 (involvement of increasing number and range of nodes) - M0 (no distant metastases) M1 to M2 (presence of metastases)
 - T1 to T4 (increasing size) - N0 ( no nodal involvement) N1 to N3 (involvement of increasing number and range of nodes) - M0 (no distant metastases) M1 to M2 (presence of metastases)")
46
Stage of a tumor refers to the extent of spread. system used is the TNM (tumor, node, metastasis) There are different TNMs developed for various cancers
 There are different TNMs developed for various cancers.")
47
STAGING (TNM) TNM for breast cancer (different for other cancers): Tis - Carcinoma-in-situ T1 - Gross size of tumor is less than 2.0 cm diameter T2 - Gross size of tumor is between 2-5 cm diameter T3 - Gross size of tumor is above 5 cm diameter T4 - Tumor of any size involving chest wall or skin
 TNM for breast cancer (different for other cancers): Tis - Carcinoma-in-situ T1 - Gross size of tumor is less than 2.0 cm diameter T2 - Gross size of tumor is between 2-5 cm diameter T3 - Gross size of tumor is above 5 cm diameter T4 - Tumor of any size involving chest wall or skin")
48
N0 - No axillary node involved N1 - Metastases to axillary nodes that are freely mobile N2 - Metastases to fixed (immobile) axillary nodes N3 - Metastases to internal mammary nodes
 axillary nodes N3 - Metastases to internal mammary nodes")
49
M0 – No metastases outside of local nodes M1 - Metastases present Use of these grading and staging can predict prognosis for an individual patient and also allows comparison of treatment results from one centre to another.

50
Predisposition to cancer Geographic and Racial factors Environmental and cultural influences Age and childhood cancer Heredity Acquired preneoplastic disorders

51
Race and Geographic locale Leading cause of death in males - cancers of the lung, colon & prostate Leading cause of death in females - cancers of the lung, breast & colon Environmental factors influence occurrence of specific forms of cancer in different parts of the world

52
Environmental influences examples of environmental factors * increased risk with occupational exposure to asbestos, vinyl chloride and naphthylamine * association of CA of the oropharynx, larynx and lung with cigarette smoking * alcohol abuse – risk of CA in esophagus and liver carcinoma

53
Age Most common = > 55 years of age Common in children < 15 years e.g. leukemias and lymphomas neuroblastomas, Wilm’s tumor, retinoblastomas and sarcomas of bone and skeletal muscle

54
Heredity Close relatives of cancer patients have a higher than normal incidence of the same neoplasm Approximately 40% of retinoblastomas are familial Some defect in DNA repair e.g. xeroderma pigmentosum

55
Acquired Preneoplastic Disorders Clinical conditions associated with increased risk of cancers Cirrhosis of liver – hepatocellular CA Atrophic gastritis – stomach CA Chronic ulcerative colitis – colon CA Leukoplakia of the oral and genital mucosa – squamous cell CA

56
Acquired Preneoplastic Disorders Association between - Endometrial hyperplasia and endometrial carcinoma - Cervical dysplasia and cervical carcinoma - Bronchial mucosal metaplasia and dysplasia and bronchogenic CA

57
Clinical Manifestations Varied and inconstant Asymptomatic lesions or nonspecific symptoms 2 categories for advancing neoplasms: Abnormalities from the tumor mass Physiologic derangements produced indirectly

58
Cancer’s 7 Warning Signals 1. Change in bowel or bladder habits 2. A sore that does not heal 3. Unusual bleeding or discharge 4. Thickening or lump in breast or elsewhere 5. Indigestion or difficulty in swallowing 6. Obvious change in wart or mole 7. Nagging cough or hoarseness

59
Signs of expansile growth Near or on the surface of the body - visible or palpable mass GIT,GUT, Respiratory -obstruction, vomiting, jaundice, cough, urinary retention CNS - pain, paralysis or sensory loss

60
Signs of infiltrative growth Pain Numbness Paralysis Signs of nerve invasion are also signs of incurability

61
Signs of tumor necrosis Tumor necrosis, ulceration, bleeding Fatigue and weakness (signs of anemia) Edema, pain, tenderness and fever Fever, leukocytosis, elevation of ESR, anorexia and malaise
 Edema, pain, tenderness and fever Fever, leukocytosis, elevation of ESR, anorexia and malaise")
62
Cachexia Loss of body fat, wasting, and profound weakness Cancer cachexia Multifactorial 1. Loss of appetite 2. Infections due to immunosuppression 3. Bleeding from ulcerative lesions 4. Production of cachectin

63
PAP SMEAR A cytologic screening (cells are collected and examined) which aims for cervical cancer prevention and control Short for Papanicolaou test to detect potentially pre-cancerous and cancerous processes of the cervix recommended for females 21 yrs old and above to be done every 3 years
 which aims for cervical cancer prevention and control Short for Papanicolaou test to detect potentially pre-cancerous and cancerous processes of the cervix recommended for females 21 yrs old and above to be done every 3 years")
64
THE END

Similar presentations






>")














