Download presentation
Presentation is loading. Please wait.

4
Wave, IntervalDuration (msec) P wave duration<120 PR interval120-200 QRS duration<110-120 QT interval (corrected) ≤440-460
 P wave duration<120 PR interval QRS duration< QT interval (corrected) ≤")
7
Retrograde P waves precede onset of the QRS complex. AV junctional rhythm, rate approx. 50 min. Retrograde P wave follows each junctional discharge.

8
A short episode of atrial flutter is followed by 5 seconds of asystole before a junctional escape rhythm resumes. The patient became presyncopal at this point. Intermittent sinus arrest with junctional escape beats at irregular intervals (red circles)
.")
10
ATRIOVENTRICULAR BLOCK (AV Block)
")
12
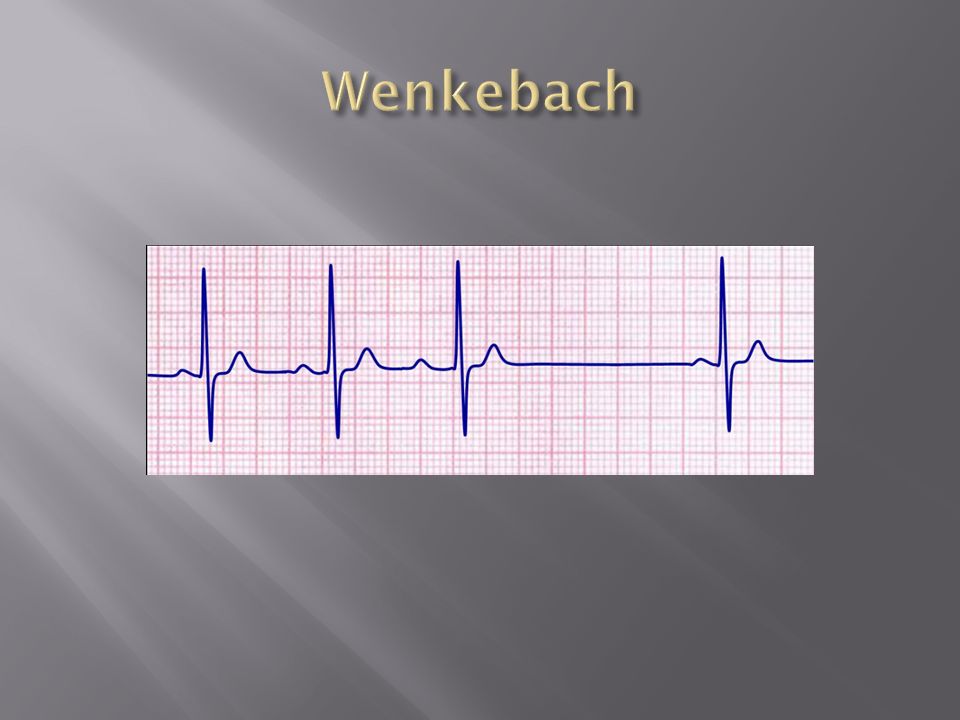
Mobitz type I (2:1) Mobitaz type II (Wenkebach)
 Mobitaz type II (Wenkebach)")
19
1. Left BUNDLE BRANCH BLOCK (LBBB)
")
22
Basic requirements include a prolonged QRS duration to 120 milliseconds or beyond; broad and commonly notched R waves in leads I, aVL, and the left precordial leads; narrow r waves followed by deep S waves in the right precordial leads; and absent septal q waves. R waves are typically tall and S waves are deep.

24
The ST-T waves are, as in LBBB, discordant with the QRS complex, so that T waves are inverted in the right precordial leads (and other leads with a terminal R′ wave) and upright in the left precordial leads and in leads I and aVL.
 and upright in the left precordial leads and in leads I and aVL.")
26
QRS duration ≥ 120 msec Broad, notched R waves (rsr′, rsR′, or rSR′ patterns) in right precordial leads (V 1 and V 2 ) Wide and deep S waves in left precordial leads (V 5 and V 6 )
 in right precordial leads (V 1 and V 2 ) Wide and deep S waves in left precordial leads (V 5 and V 6 )")
28
RBBB with acute anterior MI. Loss of anterior depolarization forces results in QR-type complexes in the right to mid precordial leads, with ST elevations and evolving T wave inversions (V 1 to V 6 ).
..")
29
LBBB with acute inferior MI. Note the prominent ST segment elevation in L II, III, and aVF, with reciprocal ST segment depression in I and aVL superimposed on secondary ST-T changes. The underlying rhythm is AF.

30
With uncomplicated left bundle branch block, early septal forces are directed to the left. Therefore, no Q waves will be seen in leads V 5 and V 6 With left bundle branch block complicated by anteroseptal infarction, early septal forces can be directed posteriorly and rightward

31
Therefore, prominent Q waves may appear in V 5 and V 6 as a paradoxical marker of septal infarction (right panel)., Anterior wall infarction (involving septum) with left bundle branch block. Note the presence of QR complexes in leads I, aVL, V 5, and V 6.

32
Unifascicular Blocks

33
The most characteristic finding is marked left axis deviation. However, LAFB is not synonymous with left axis deviation. Axis shifts to between -30 and -45 degrees commonly reflect other conditions, such as LVH, without conduction system damage and such patterns are best referred to as left axis deviation rather than as LAFB.

35
Frontal plane mean QRS axis of -45 to - 90 degrees rS patterns in leads II, III, and aVF and a qR pattern in lead aVL QRS duration <120 msec

37
Frontal plane mean QRS axis >120 degrees RS pattern in leads I and aVL with qR patterns in inferior leads QRS duration < 120 msec Exclusion of other factors causing right axis deviation (e.g., right ventricular overload patterns, lateral infarction)
")
Similar presentations



































 Heart Blocks>")




:>")


