Download presentation
Presentation is loading. Please wait.

1
TOOTH DEPOSITS Dr. Majambo M.

2
DEPOSITS Hard or soft deposit on the tooth surface
Hard = calculus + stain Dental stain Can be either Intrinsic extrinsic

3
Dental deposits Material alba Plaque Calculus Stains Intrinsic
extrinsic

4
stains

5
Stain cont.

6
Causes Causes Extrinsic dental deposits/stains
multiple local conditions systemic conditions Extrinsic dental deposits/stains Dental plaque and calculus, Foods and beverages, Tobacco, Chromogenic bacteria, Metallic compounds, Topical medications.

7
Intrinsic dental stains
Causes Dental materials Dental conditions and caries Trauma Infections Medications Nutritional deficiencies Genetic Amelogenesis imparfecta. (AI) Dentinogenesis imparfecta. (DI) Dentinal dysplasia (DD)
 Dentinogenesis imparfecta. (DI) Dentinal dysplasia (DD)")
8
Extrinsic stains Definition Predisposing factors
stains located on the outer surface of the tooth structure and caused by topical or extrinsic agents. Predisposing factors Enamel defects pits, fissures, and defects in the outer surface of the enamel are susceptible to the accumulation of stain-producing food, beverages, tobacco, and other topical agents Salivary dysfunction Poor oral hygiene

9
Other factors Plaque and calculus
Tannin (tea, coffee, and other beverages) betel nut chewing
 betel nut chewing.")
10
Extrinsic stain

11
Intrinsic stains Causes Numerous Stain distribution varies
localized (e.g., 1 or 2 teeth) Pre-eruptive or post-eruptive processes generalized - involvement of primary and secondary teeth. indicates a deviation in normal tooth formation.
 Pre-eruptive or post-eruptive processes. generalized - involvement of primary and secondary teeth. indicates a deviation in normal tooth formation.")
12
Morbidity If tooth discoloration is not treated, it can affect NB
person's smile (esthetics) social and psychological sequelae. NB Smiling End result of a complex: neurological, muscular, sensory, and psychological process. Unattractive smile, due to discolored teeth, can have negative psychological, social, and clinical implications.
 social and psychological sequelae. NB. Smiling. End result of a complex: neurological, muscular, sensory, and psychological process. Unattractive smile, due to discolored teeth, can have negative psychological, social, and clinical implications.")
13
Clinical History The patient's history of tooth discoloration provides useful information regarding the etiology. Chief complaint and history of chief complaint Aesthetics pain

14
Medical history: A history of maternal or childhood diseases or the use of medications (see Causes) . This may explain tooth discoloration because the conditions can adversely influence normal tooth development

15
Family history: Several genetic diseases are associated with tooth-associated disorders the most common include AI, DI, and DD. Patients may be unaware of the diseases but often confirm that a family member had similar tooth discoloration.

16
Social history: The use of tobacco and similar products, such as the chewing of areca (betel) nuts, commonly leads to staining of the teeth. Determining the type of tobacco habit (eg, smoking vs chewing) is important because the distribution of the stain may vary.
 is important because the distribution of the stain may vary.")
17
Dental history: Diet history:
The dental history can reveal useful information regarding the Last dental cleaning Previous dental treatments Oral hygiene practices Use of mouthwash Traumatic events involving dentition. Diet history: A history of nutritional deficiencies or ingestion of foods that can stain teeth is important. Querying patients about the quality of their dietis always useful.

18
Physical Extrinsic stain/discoloration
Usually, discoloration colors include brown, black, gray, green, orange, and yellow on occasion, a metallic sheen is present. The scratch test is usually used to distinguish between extrinsic and intrinsic discoloration.

19
intrinsic discoloration
Intrinsic discoloration cannot be removed by using the scratch test.

23
Amelogenesis imparfecta

24
Material alba Material alba = white material composition
microorganisms, desquamated epith. cells, Disintegrated WBC food debris MA is loosely adherent to surfaces of plaques, teeth, gingiva or dental appliances.

25
Plaque Plaque is a soft, sticky accumulation that occurs on dental and various other intra-oral surfaces. It is the host to a complex micro-system of micro-organisms whose pathogenicity and virulence cause inflammatory diseases of the gingival & periodontal tissues.

26
Plaque cont. Plaque can be removed from tooth surfaces by direct brushing. It is possible to have a mouth with plaque but no calculus. Calculus acts as a focal point for plaque accumulation, a nidus of bacteria and hinders complete removal of plaque. It is almost impossible to have a mouth with calculus but no plaque.

27
Plaque Formation Passes through several stages Pellicle formation ↓
Bacterial Colonization Growth and Maturation of Plaque: Plaque Retention Factors

28
Plaque Retention Factors
These are conditions that favor plaque accumulation and hinder plaque removal by the patient and the dental professional. Examples of these are: Orthodontic Appliances Partial Dentures Malocclusions Faulty Restorations Calculus Deep Pockets Mouth Breathing Tobacco Use Certain Medications

30
Calculus In dentistry, calculus or tartar refers to calcified deposits on the teeth, formed by the continuous mineralization of presence of dental plaque. Its rough surface provides an ideal medium for further plaque formation, threatening the health of the gingiva. Calculus absorbs unaesthetic stains far more easily than natural teeth.

32
Calculus accumulations occur in the absence of adequate oral care.
Once formed, it is generally too firmly adherant to teeth to be removed with anything available to an individual at home Patients with calculus must therefore visit their dental professionals so that the calculus can be removed (Scaling)
")
33
Clinical significance
Plaque accumulation causes the gingiva to become irritated and inflamed leading to gingivitis. When the gingiva become so irritated that there is a loss of the connective tissue fibers and bone that surrounds then it leads to periodontitis. Dental plaque is the most important cause of periodontitis and it is referred to as the primary etiology. Plaque that remains in the oral cavity long enough will eventually calcify and become calculus.

34
Calculus is detrimental to gingival health because it serves as a trap for increased plaque formation and retention Thus, calculus, along with everything else that causes a localized build-up of plaque, is referred to as a secondary etiology of periodontitis.

35
Types Supragingival calculus
Calculus formed on the tooth surface above the gum line. Supra-gingival calculus is adherent to the crown. Found mostly on the lingual surfaces of the mandibular incisors in relation to the opening of Wharton's ducts and on the buccal surfaces of maxillary molars in relation to the opening of Stensen's ducts.

36
Subgingival calculus Subgingival calculus forms on root surfaces below the gingival margin and can extend deep into periodontal pockets. A more irregular subgingival cemental surface allows deposits to form into the cemental irregularities. This makes the attachment of the subgingiva calculus more tenacious and difficult to remove. It also tends to be darker or black in color. All calculus can however absorb extrinsic stains (coffee; tea; tobacco;etc) and appear dark brown or black.
 and appear dark brown or black.")
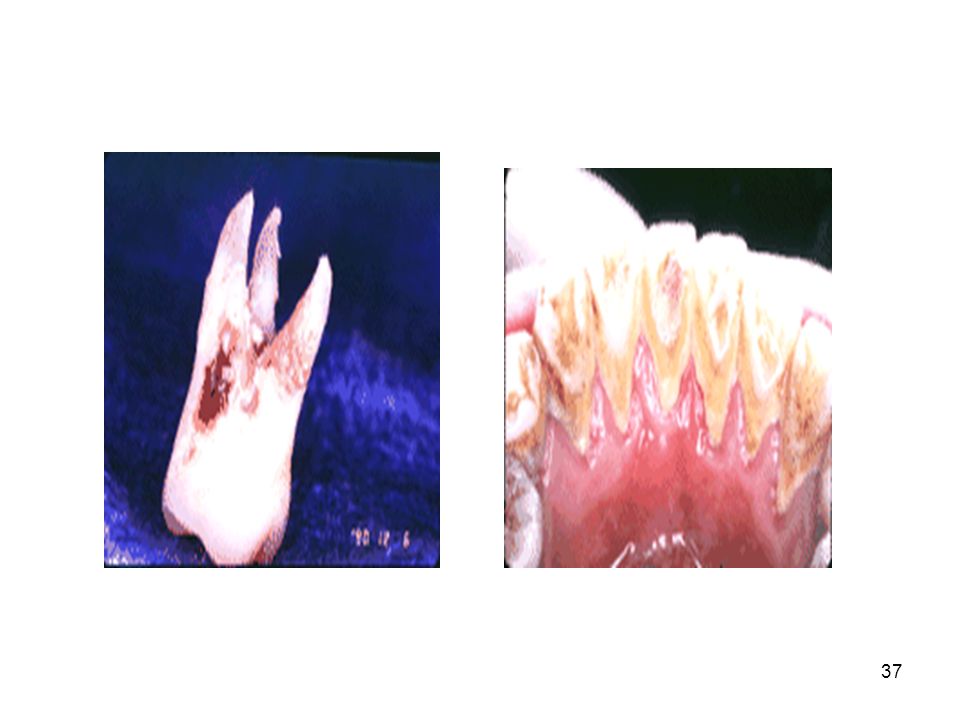
38
Subgingival calculus can often be seen on radiographs on the mesial and distal aspect of teeth (proximal surfaces) but explorer detection is needed to evaluate the amount of calculus present
 but explorer detection is needed to evaluate the amount of calculus present")
39
Calculus formation Calculus is formed by the deposition of calcium and phosphate salts in bacterial plaque. These salts are present in salivary and gingival crevicular fluids. Plaque mineralization begins within hours and takes an average of 12 days to mature. Calculus contributes to the disease by providing foci for plaque accumulation. It is not the causative or etiologic factor.

40
Rate of Calculus Formation
It is known that certain people form calculus faster than others. The following factors increase the rate of calculus formation. Elevated salivary pH. Elevated salivary calcium concentration. Elevated bacterial protein and lipid concentration. Low individual inhibitory factors. Higher total salivary lipid levels.

41
Microbiology of Dental Plaque
Dental plaque is a soft deposit that accumulates on the teeth. Plaque can be defined as a complex microbial community, with greater than 1010 bacteria per milligram.

42
SELECTED BACTERIAL SPECIES FOUND IN DENTAL PLAQUE
Facultative Gram-Positive Streptococcus mutans Streptococcus sanguis Actinomyces viscosus Gram-negative Actinobacillus actinomycetemcomitans Capnocytophypa species Eikenella corrodens Anaerobic Porphyromonas gingivalis Fusobacterium nucleatum Prevotella intermedia Bacteroides forsythus Campylobacter rectus SpirochetesT reponema denticola (Other Treponema species)
")
43
Thank you!!!

Similar presentations










 Click here to launch video Click here to download print activity.>")

>")











