Download presentation
Presentation is loading. Please wait.

1
Emergency Medicine Peri-arrest arrhythmias Assoc.Prof.Diana Cimpoeşu MD,PhD Assoc.Prof.Diana Cimpoeşu MD,PhD 2013 2013 U.M.F. “Gr. T. Popa” Iaşi U.M.F. “Gr. T. Popa” Iaşi

2
Monitoring, Rhythm Recognition and 12-lead ECG Tachycardia, Cardioversion and Drugs Bradycardia, Cardiac Pacing and Drugs

3
Conducting system

4
QRS Complex

5
How to read a rhythm strip 1. Is there any electrical activity? 2. What is the ventricular (QRS) rate? 3. Is the QRS rhythm regular or irregular? 4. Is the QRS width normal (narrow) or broad? 5. Is atrial activity present? (If so, what is it: P waves? Other atrial activity?) 6. How is atrial activity related to ventricular activity?
 rate. 3. Is the QRS rhythm regular or irregular. 4. Is the QRS width normal (narrow) or broad. 5. Is atrial activity present. (If so, what is it: P waves. Other atrial activity ) 6. How is atrial activity related to ventricular activity .")
6
How to monitor the ECG Self-adhesive pads Self-adhesive pads 3-lead monitoring 3-lead monitoring 12-lead monitoring 12-lead monitoring

7
Self-adhesive pads

8
3-lead monitoring

9
ECG recognition

10
Principles of treatment in peri-arrest arthymia In all cases : In all cases : -give oxygen -i.v acces -monitor -12-lead ECG -12-lead ECG -electrolyte abnormalities - correct any abnormalities K, Mg, Ca

11
Tachycardia algorithm (with pulse)
")
12
ADVERSE SIGNS? STABLE OR UNSTABLE? ShockSyncope Myocardial ischaemia Heart failure

13
Tachycardia algorithm

14
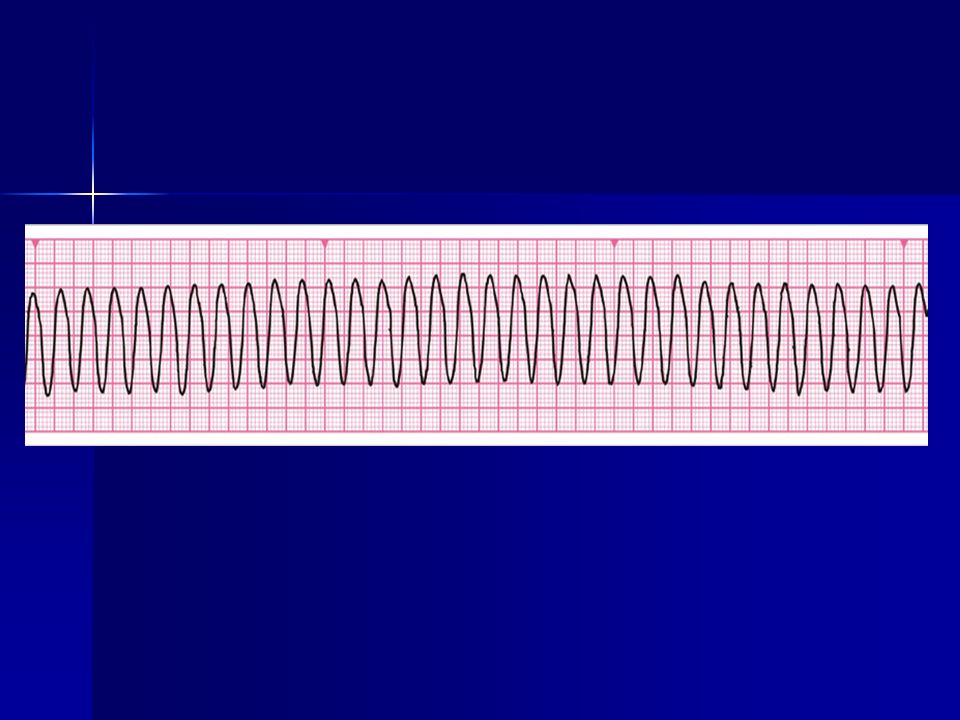
Case study 1 Clinical setting and history Clinical setting and history –65-year-old woman –In monitored bed 3 days after anterior myocardial infarction –Complains to nurse of feeling unwell Clinical course Clinical course –ABCDE A : Clear A : Clear B : Spontaneous breathing, rate 26 min -1 B : Spontaneous breathing, rate 26 min -1 C : Looks pale, HR 200 min -1, BP 70/42 mmHg, CRT 3 s C : Looks pale, HR 200 min -1, BP 70/42 mmHg, CRT 3 s Initial rhythm? D : Alert, glucose 5.6 mmol l -1 D : Alert, glucose 5.6 mmol l -1 E : Nil of note E : Nil of note What action will you take?

16
Stable broad-complex tachycardia

17
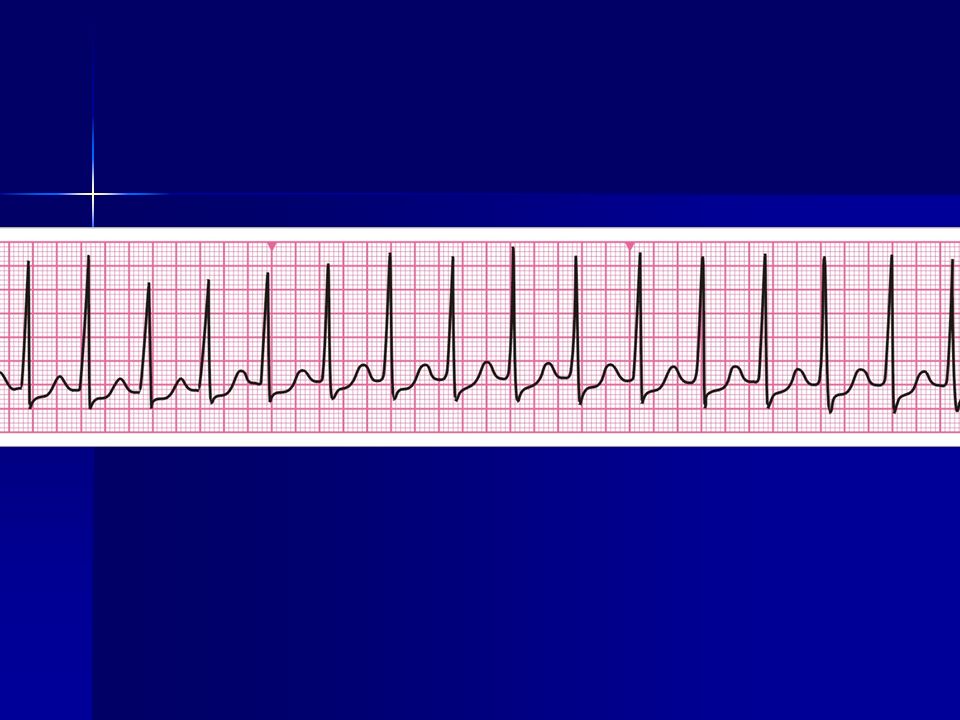
Stable narrow -complex tachycardia

18
Case study 2 Clinical setting and history Clinical setting and history –48-year-old woman admitted to ED –History of palpitation over past 12 h Clinical course Clinical course –ABCDE A : Clear A : Clear B : Spontaneous breathing, rate 16 min -1 B : Spontaneous breathing, rate 16 min -1 C : P 180 min -1, BP 110/90 mmHg, CRT < 2 s C : P 180 min -1, BP 110/90 mmHg, CRT < 2 s Initial rhythm? D : Alert, glucose 5.5 mmol l -1 D : Alert, glucose 5.5 mmol l -1 E : Nil of note E : Nil of note What action will you take?

20
Case study 2 (continued) Clinical course Clinical course –No response to vagal manoeuvres –Vital signs unchanged What action will you take now?
 Clinical course Clinical course –No response to vagal manoeuvres –Vital signs unchanged What action will you take now")
21
Case study 2 (continued) AdenosineIndications –Narrow-complex tachycardia –Regular broad-complex tachycardia of uncertain nature –Broad-complex tachycardia only if previously confirmed SVT with bundle branch block Contraindications –Asthma Dose –6 mg bolus by rapid IV injection –Up to 2 doses of 12 mg if needed Actions –Blocks conduction through AV node
 AdenosineIndications –Narrow-complex tachycardia –Regular broad-complex tachycardia of uncertain nature –Broad-complex tachycardia only if previously confirmed SVT with bundle branch block Contraindications –Asthma Dose –6 mg bolus by rapid IV injection –Up to 2 doses of 12 mg if needed Actions –Blocks conduction through AV node")
22
Case study 2 (continued) AmiodaroneIndications –Broad-complex and narrow-complex tachycardia Dose –300 mg over 20-60 min IV –900 mg infusion over 24 h –Preferably via central venous catheter Actions –Lengthens duration of action potential –Prolongs QT interval –May cause hypotension
 AmiodaroneIndications –Broad-complex and narrow-complex tachycardia Dose –300 mg over min IV –900 mg infusion over 24 h –Preferably via central venous catheter Actions –Lengthens duration of action potential –Prolongs QT interval –May cause hypotension")
23
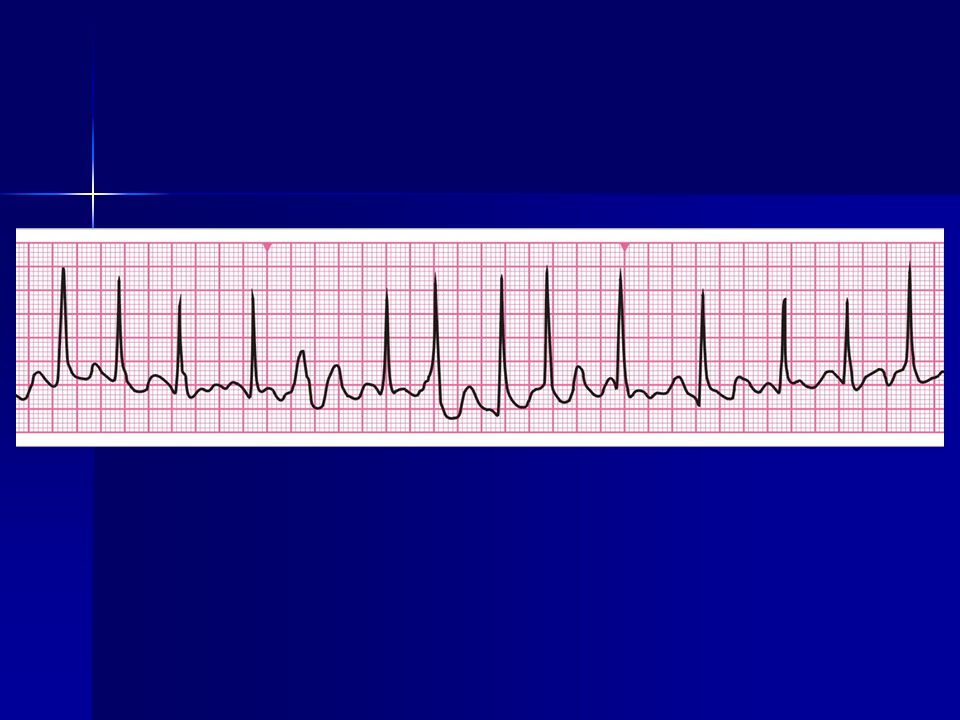
Case study 3 Clinical setting and history Clinical setting and history –76-year-old man –History of hypertension treated with a diuretic –In the recovery area after an uncomplicated hernia repair –Nurses report the sudden onset of tachycardia Clinical course Clinical course –ABCDE A : Clear A : Clear B : Spontaneous breathing, rate 18 min -1 B : Spontaneous breathing, rate 18 min -1 C : P 170 min -1, BP 100/60 mmHg, CRT < 2 s C : P 170 min -1, BP 100/60 mmHg, CRT < 2 s Initial rhythm? D : Alert, glucose 4.0 mmol l -1 D : Alert, glucose 4.0 mmol l -1 E : Nil of note E : Nil of note What action will you take?

24
Case study 3 (continued) Clinical course Clinical course –Patient is given IV metoprolol –30 min later, he complains of chest discomfort –ABCDE A : Clear A : Clear B : Spontaneous breathing, rate 24 min -1 B : Spontaneous breathing, rate 24 min -1 C : HR 170 min -1, BP 85/50 mmHg, CRT 4 s C : HR 170 min -1, BP 85/50 mmHg, CRT 4 s What is the rhythm? What action will you take ?

26
Case study 3 (continued) Clinical course Clinical course –Cardioversion restores sinus rhythm –Patient is transferred back to the day- case unit What actions may be required as part of discharge planning?
 Clinical course Clinical course –Cardioversion restores sinus rhythm –Patient is transferred back to the day- case unit What actions may be required as part of discharge planning")
27
Peri-Arrest Bradycardia Bradycardia, Cardiac Pacing and Drugs

28
Bradycardia algorithm Includes rates inappropriately slow for haemodynamic state

29
Case study 4 Clinical setting and history Clinical setting and history –60-year-old man referred to admissions unit by GP –Long-term history of heart disease –Feeling light-headed and breathless Clinical course Clinical course –ABCDE A : Clear A : Clear B : Spontaneous breathing, rate 18 min -1 B : Spontaneous breathing, rate 18 min -1 C : Looks pale, P 40 min -1, BP 90/50 mmHg, CRT 3 s C : Looks pale, P 40 min -1, BP 90/50 mmHg, CRT 3 s Initial rhythm? D : Alert, glucose 4.5 mmol l -1 D : Alert, glucose 4.5 mmol l -1 E : Nil of note E : Nil of note What action will you take?

31
Case study (continued) Clinical course Clinical course –No response to atropine –Patient becomes more breathless, cold, clammy and mildly confused –Change in rhythm –ABCDE A : Clear A : Clear B : Spontaneous breathing, rate 24 min -1 B : Spontaneous breathing, rate 24 min -1 widespread crackles on auscultation widespread crackles on auscultation C : Looks pale, HR 35 min -1, BP 80/50 mmHg, CRT 4 s C : Looks pale, HR 35 min -1, BP 80/50 mmHg, CRT 4 s D : Responding to verbal stimulation D : Responding to verbal stimulation E : Nil of note E : Nil of note What will you do now?
 Clinical course Clinical course –No response to atropine –Patient becomes more breathless, cold, clammy and mildly confused –Change in rhythm –ABCDE A : Clear A : Clear B : Spontaneous breathing, rate 24 min -1 B : Spontaneous breathing, rate 24 min -1 widespread crackles on auscultation widespread crackles on auscultation C : Looks pale, HR 35 min -1, BP 80/50 mmHg, CRT 4 s C : Looks pale, HR 35 min -1, BP 80/50 mmHg, CRT 4 s D : Responding to verbal stimulation D : Responding to verbal stimulation E : Nil of note E : Nil of note What will you do now")
32
Case study (continued) Consider need for expert help Consider need for expert help Prepare for transcutaneous pacing Prepare for transcutaneous pacing Consider percussion pacing as interim measure Consider percussion pacing as interim measure Confirm electrical capture and mechanical response once transcutaneous pacing has started Confirm electrical capture and mechanical response once transcutaneous pacing has started
 Consider need for expert help Consider need for expert help Prepare for transcutaneous pacing Prepare for transcutaneous pacing Consider percussion pacing as interim measure Consider percussion pacing as interim measure Confirm electrical capture and mechanical response once transcutaneous pacing has started Confirm electrical capture and mechanical response once transcutaneous pacing has started")
33
Case study (continued) AtropineIndication –Symptomatic bradycardia Contraindication –Do not give to patients who have had a cardiac transplant Dose –500 mcg IV, repeated every 3 - 5 min to maximum of 3 mg Actions –Blocks vagus nerve –Increases sinus rate –Increases atrioventricular conduction Side effects –Blurred vision, dry mouth, urinary retention –Confusion
 AtropineIndication –Symptomatic bradycardia Contraindication –Do not give to patients who have had a cardiac transplant Dose –500 mcg IV, repeated every min to maximum of 3 mg Actions –Blocks vagus nerve –Increases sinus rate –Increases atrioventricular conduction Side effects –Blurred vision, dry mouth, urinary retention –Confusion")
34
Case study (continued) Adrenaline Infusion of 2-10 mcg min -1 titrated to response OR Isoprenaline infusion 5 mcg min -1 as starting dose OR Dopamine infusion 2-5 mcg kg -1 min -1
 Adrenaline Infusion of 2-10 mcg min -1 titrated to response OR Isoprenaline infusion 5 mcg min -1 as starting dose OR Dopamine infusion 2-5 mcg kg -1 min -1")
35
Post-resuscitation care Return of spontaneos circulation ROSC Return of spontaneos circulation ROSC Hypoxia and hypercarbia –contribute to secondary brain injury Hypoxia and hypercarbia –contribute to secondary brain injury

36
Post resuscitation care The goal is to restore: Normal cerebral function Normal cerebral function Stable cardiac rhythm Stable cardiac rhythm Adequate organ perfusion Adequate organ perfusion Quality of life Quality of life

37
Post cardiac arrest syndrome Post cardiac arrest brain injury: Post cardiac arrest brain injury: –Coma, seizures, myoclonus Post cardiac arrest myocardial dysfunction Post cardiac arrest myocardial dysfunction Systemic ischaemia-reperfusion response Systemic ischaemia-reperfusion response –‘Sepsis-like’ syndrome Persistence of precipitating pathology Persistence of precipitating pathology

38
Airway and breathing Ensure a clear airway, adequate oxygenation and ventilation Ensure a clear airway, adequate oxygenation and ventilation Consider tracheal intubation, sedation and controlled ventilation Consider tracheal intubation, sedation and controlled ventilation Pulse oximetry: Pulse oximetry: –Aim for SpO 2 94 – 98% Capnography: Capnography: –Aim for normocapnia –Avoid hyperventilation

39
Airway and breathing Look, listen and feel Look, listen and feel Consider: Consider: –Simple/tension pneumothorax –Collapse/consolidation –Bronchial intubation –Pulmonary oedema –Aspiration –Fractured ribs/flail segment

40
Airway and breathing Insert gastric tube to decompress stomach and improve lung compliance Insert gastric tube to decompress stomach and improve lung compliance Secure airway for transfer Secure airway for transfer Consider immediate extubation if patient breathing and conscious level improves quickly after ROSC Consider immediate extubation if patient breathing and conscious level improves quickly after ROSC

41
Circulation Pulse and blood pressure Pulse and blood pressure Peripheral perfusion e.g. capillary refill time Peripheral perfusion e.g. capillary refill time Right ventricular failure Right ventricular failure –Distended neck veins Left ventricular failure Left ventricular failure –Pulmonary oedema ECG monitor and 12-lead ECG ECG monitor and 12-lead ECG

42
Disability Neurological assessment: Glasgow Coma Scale score Glasgow Coma Scale score Pupils Pupils Limb tone and movement Limb tone and movement Posture Posture

43
Further assessment History Health before the cardiac arrest Health before the cardiac arrest Time delay before resuscitation Time delay before resuscitation Duration of resuscitation Duration of resuscitation Cause of the cardiac arrest Cause of the cardiac arrest Family history Family history

44
Further assessment Monitoring Vital signs Vital signs ECG ECG Pulse oximetry Pulse oximetry Blood pressure e.g. arterial line Blood pressure e.g. arterial line Capnography Capnography Urine output Urine output Temperature Temperature

45
Further assessment Investigations Arterial blood gases Arterial blood gases Full blood count Full blood count Biochemistry including blood glucose Biochemistry including blood glucose Troponin Troponin Repeat 12-lead ECG Repeat 12-lead ECG Chest X-ray Chest X-ray Echocardiography Echocardiography

46
Chest X-ray

47
Transfer of the patient Discuss with admitting team Discuss with admitting team Cannulae, drains, tubes secured Cannulae, drains, tubes secured Suction Suction Oxygen supply Oxygen supply Monitoring Monitoring Documentation Documentation Reassess before leaving Reassess before leaving Talk to family Talk to family

48
Out-of-hospital VF arrest associated with AMI Pacing Cooling IABP Defibrillator Inotropes Ventilation Enteral nutrition Insulin

49
Optimising organ function Heart Post cardiac arrest syndrome Post cardiac arrest syndrome Ischaemia-reperfusion injury: Ischaemia-reperfusion injury: –Reversible myocardial dysfunction for 2-3 days –Arrhythmias

50
Optimising organ function Heart Poor myocardial function despite optimal filling: Poor myocardial function despite optimal filling: –Echocardiography –Cardiac output monitoring –Inotropes and/or balloon pump Mean blood pressure to achieve: Mean blood pressure to achieve: –Urine output of 1 ml kg -1 hour -1 –Normalising lactate concentration

51
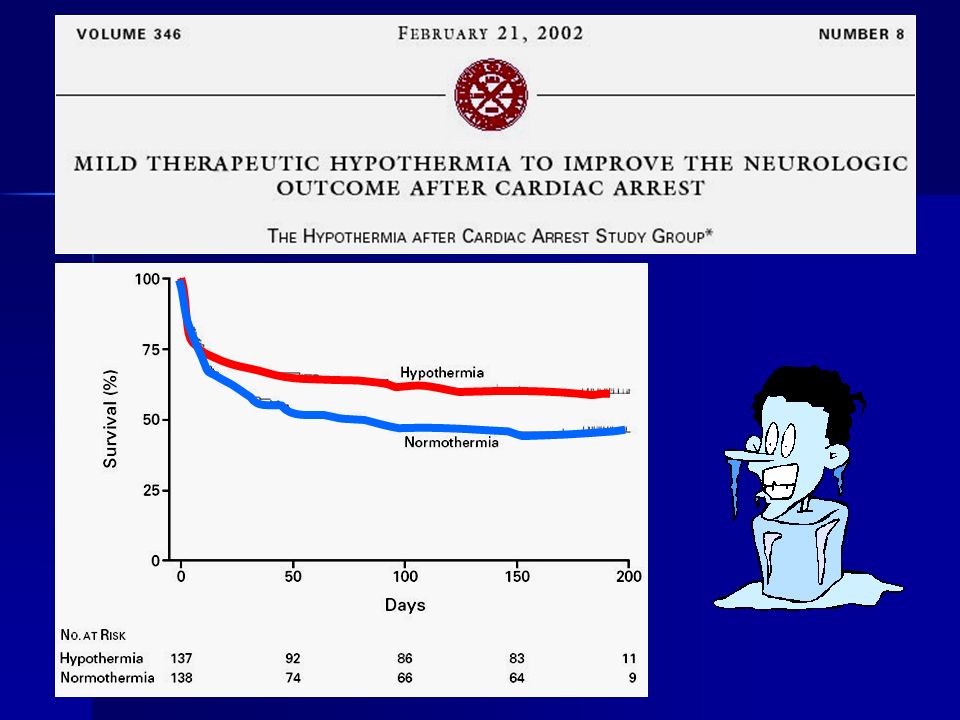
Optimising organ function Brain Impaired cerebral autoregulation – maintain ‘normal’ blood pressure Impaired cerebral autoregulation – maintain ‘normal’ blood pressure Sedation Sedation Control seizures Control seizures Glucose (4-10 mmol l -1 ) Glucose (4-10 mmol l -1 ) Normocapnia Normocapnia Avoid/treat hyperthermia Avoid/treat hyperthermia Consider therapeutic hypothermia Consider therapeutic hypothermia
 Glucose (4-10 mmol l -1 ) Normocapnia Normocapnia Avoid/treat hyperthermia Avoid/treat hyperthermia Consider therapeutic hypothermia Consider therapeutic hypothermia")
52
Therapeutic hypothermia Who to cool? Unconscious adults with ROSC after VF arrest should be cooled to 32-34 o C Unconscious adults with ROSC after VF arrest should be cooled to 32-34 o C May benefit patients after non-shockable/in- hospital cardiac arrest May benefit patients after non-shockable/in- hospital cardiac arrest Exclusions: severe sepsis, pre-existing medical coagulopathy Exclusions: severe sepsis, pre-existing medical coagulopathy Start as soon as possible and continue for 24 h Start as soon as possible and continue for 24 h Rewarm slowly 0.25 o C h -1 Rewarm slowly 0.25 o C h -1

53
Therapeutic hypothermia How to cool? Induction - 30 ml kg -1 4 o C IV fluid and/or external cooling Induction - 30 ml kg -1 4 o C IV fluid and/or external cooling Maintenance - external cooling: Maintenance - external cooling: –Ice packs, wet towels –Cooling blankets or pads –Water circulating gel-coated pads Maintenance - internal cooling Maintenance - internal cooling –Intravascular heat exchanger –Cardiopulmonary bypass

55
Assessment of prognosis No clinical neurological signs can predict outcome < 24 h after ROSC No clinical neurological signs can predict outcome < 24 h after ROSC Poor outcome predicted at 3 days by: Poor outcome predicted at 3 days by: –Absent pupil light and corneal reflexes –Absent or extensor motor response to pain But limited data on reliability of these criteria after therapeutic hypothermia But limited data on reliability of these criteria after therapeutic hypothermia

56
Organ donation Non-surviving post cardiac arrest patient may be a suitable donor: Non-surviving post cardiac arrest patient may be a suitable donor: –Heart-beating donor (brainstem death) –Non-heart-beating donor
 –Non-heart-beating donor")
57
Questions?

Similar presentations




















>")