Download presentation
Presentation is loading. Please wait.

1
Why Does Population Growth Vary Among Regions?
Chapter 2 Key Issue 3

2
Earth’s Population History
7 billion reached 2011 (12 years later) 6 billion reached 1999 (12 years later) 5 billion reached 1987 (13 years later) 4 billion reached 1974 (15 years later) 3 billion reached 1959 (29 years later) DISCUSSION: * What is the present world population? [get an up-to-date estimate at 2 billion reached 1930 (100 years later) 1 billion reached circa 1830 Source: Kuby, HGIA
 6 billion reached 1999 (12 years later) 5 billion reached 1987 (13 years later) 4 billion reached 1974 (15 years later) 3 billion reached 1959 (29 years later) DISCUSSION: * What is the present world population [get an up-to-date estimate at 2 billion reached 1930 (100 years later) 1 billion reached circa Source: Kuby, HGIA.")
3
Demographic Transition Model
Explaining Spatial Patterns of World Population Growth Many graphics in this powerpoint are from Michael Kuby et al., Human Geography in Action (instructor package) or online materials posted by Keith Montgomery, Dept of Geology and Geography, Univ of Wisconsin - Marathon County (
 or online materials posted by Keith Montgomery, Dept of Geology and Geography, Univ of Wisconsin - Marathon County (")
4
The Demographic Transition
Process of Change in society’s population from high CBR, CDR, and low NIR to a condition of low CBR, CDR, and NIR

5
Demographic Transition Model
DISCUSSION: * Are there countries that do not fit this model?

6
DTM based on historical patterns in Europe & other MDCs

7
DTM only predicts changes in birth/death rates over time
Observed changes in NIR correlate to changes in economic development Thus, DTM implies: The greater the wealth, the lower the NIR... but use caution describing this relationship

8
Stages in Classic 4-Stage Demographic Transition Model (DTM)
(Some books show a 3-stage model; others mention a new 5th stage)
")
9
Stage 1: “Pre-Industrial”
High birth rates and high death rates (both about 40) Population growth very slow Agrarian society High rates of communicable diseases Pop. increases in good growing years; declines in bad years (famine, diseases) No country or world region still in Stage One
 Population growth very slow. Agrarian society. High rates of communicable diseases. Pop. increases in good growing years; declines in bad years (famine, diseases) No country or world region still in Stage One.")
10
Stage 2: “Early Industrial”
High birth rates (over 30) but death rates decline (to about 20) RNIs increase sharply (pop. explosion); growth rate increases thruout Stage Two Growth not from increase in births, but from decline in deaths MDCs = starts early 1800s LDCs = starts after 1950s
 but death rates decline (to about 20) RNIs increase sharply (pop. explosion); growth rate increases thruout Stage Two. Growth not from increase in births, but from decline in deaths. MDCs = starts early 1800s. LDCs = starts after 1950s.")
11
TRANSITION TO STAGE TWO IN CLASSIC DTM
Known as the Epidemiologic Transition Agricultural technology Improvements in food supply: higher yields as agricultural practices improved in “Second Agricultural Revolution” (18th century) In Europe, food quality improved as new foods introduced from Americas Medical technology Better medical understanding (causes of diseases; how they spread) Public sanitation technologies Improved water supply (safe drinking water) Better sewage treatment, food handling, and general personal hygiene Improvements in public health especially reduced childhood mortality
 In Europe, food quality improved as new foods introduced from Americas. Medical technology. Better medical understanding (causes of diseases; how they spread) Public sanitation technologies. Improved water supply (safe drinking water) Better sewage treatment, food handling, and general personal hygiene. Improvements in public health especially reduced childhood mortality.")
12
Declining Infant Mortality Rates

13
When IMR declines, fertility rates drop soon after

14
Stage 3: “Later Industrial”
Birth rates decline sharply (to about 15) Death rates decline a bit more (to about 10 or less) Note growth still occurs, but at a reduced and declining rate MDCs = starts in late 1800s LDCs = starts after 1980s* * Or hasn’t started yet
 Death rates decline a bit more (to about 10 or less) Note growth still occurs, but at a reduced and declining rate. MDCs = starts in late 1800s. LDCs = starts after 1980s* * Or hasn’t started yet.")
15
Measles Mortality, US, since 1900
Stage Three: Further improvements in medicine lower death rates more; raise life expectancies Measles Mortality, US, since 1900 TB Mortality, US, since 1900

16
TRANSITION TO STAGE THREE IN CLASSIC DTM
Known as the Fertility Transition Societies become more urban, less rural Declining childhood death in rural areas (fewer kids needed) Increasing urbanization changes traditional values about having children City living raises cost of having dependents Women more influential in childbearing decisions Increasing female literacy changes value placed on motherhood as sole measure of women’s status Women enter work force: life extends beyond family, changes attitude toward childbearing Improved contraceptive technology, availability of birth control But contraceptives not widely avail in 19th century; contributed little to fertility decline in Europe … Fertility decline relates more to change in values than to availability of any specific technology
 Increasing urbanization changes traditional values about having children. City living raises cost of having dependents. Women more influential in childbearing decisions. Increasing female literacy changes value placed on motherhood. as sole measure of women’s status. Women enter work force: life extends beyond family, changes attitude. toward childbearing. Improved contraceptive technology, availability of birth control. But contraceptives not widely avail in 19th century; contributed little to. fertility decline in Europe … Fertility decline relates more to change in. values than to availability of any specific technology.")
17
Rapidly increasing urbanization in world LDCs today
Population Classified as Urban

18
Strong inverse relationship between female literacy and fertility rates, observed globally
Increasing availability and use of modern contraception in most LDCs since 1970s

19
Stage 4: “Post-Industrial”
Birth rates and death rates both low (about 10) Population growth very low or zero MDCs = starts after 1970s LDCs = hasn’t started yet Stage 5 (?): Hypothesized (not in Classic DTM) Much of Europe now or soon in population decline as birth rates drop far below replacement level
 Population growth very low or zero. MDCs = starts after 1970s. LDCs = hasn’t started yet. Stage 5 ( ): Hypothesized (not in Classic DTM) Much of Europe now or soon in population decline. as birth rates drop far below replacement level.")
20
Key Population Indicators for Selected Countries
DISCUSSION: * Are there any countries still in stage 1 of the demographic transition? * What other countries not shown would you expect to find in stages 2, 3, and 4?

21
Differences in DTM experience: MDCs & LDCs
● Faster decline in death rates — Tech improvements diffused from MDCs & applied rapidly in LDCs post-WW2 ● Longer lag between decline in deaths and decline in births — Stage 3 slower start in LDCs where econ growth is delayed ● Higher max rates of growth in LDCs — Over 3.5% peak RNI in Mauritius and Mexico; only 1.3% peak in Sweden

22
Age structures today in LDCs are much younger than MDCs experienced – leading to prolonged “Demographic Momentum” – expected growth of pop. long after fertility declines Percentage of Population Under Age 15

23
The Demographic Transition
Fig. 2-13: The demographic transition consists of four stages, which move from high birth and death rates, to declines first in death rates then in birth rates, and finally to a stage of low birth and death rates. Population growth is most rapid in the second stage.

24
Demographic Momentum (hidden momentum)
Critics Based on England Billions and much faster then ever before Graying Population Medical Revolution- 1900’s Demographic Momentum (hidden momentum)
")
25
Population Pyramid of the U.S.

26
Population Pyramids in U.S. cities
Fig. Population pyramids can vary greatly with different fertility rates (Laredo vs. Honolulu), or among military bases (Unalaska), college towns (Lawrence), and retirement communities (Naples).
, or among military bases (Unalaska), college towns (Lawrence), and retirement communities (Naples).")
27
Rapid Growth in Cape Verde
Cape Verde, which entered stage 2 of the demographic transition in about 1950, is experiencing rapid population growth. Its population history reflects the impacts of famines and out-migration.

28
Moderate Growth in Chile
Chile entered stage 2 of the demographic transition in the 1930s, and it entered stage 3 in the 1960s.

29
Low Growth in Denmark Denmark has been in stage 4 of the demographic transition since the 1970s, with little population growth since then. Its population pyramid shows increasing numbers of elderly and few children.

30
Summary of DTM for LDCs Industrializing LDCs with some economic development follow DTM more closely; now in Stage Three. Most like MDCs in places where female literacy has increased the most. Lowest-income countries have high birth rates and deaths are leveling off at higher rates than DTM predicts (Stage Two). In some LDCs, death rates starting to increase (epidemics, worsening poverty)
. In some LDCs, death rates starting to increase (epidemics, worsening poverty)")
31
Declining Birth Rates CBR declining rapidly since 1990
Two successful Strategies Education and Health Care Contraception Critics

32
Malthus’ Theory of Population Growth
In 1798 Thomas Malthus published his views on the effect of population on food supply. His theory has two basic principles: Population grows at a geometric rate i.e. 1, 2, 4, 16, 32, etc. Food production increases at an arithmetic rate i.e. 1, 2, 3, 4, etc.

33
Malthus (cont.) The consequence of these two principles is that eventually, population will exceed the capacity of agriculture to support the new population numbers. Population would rise until a limit to growth was reached. Further growth would be limited when: preventive checks - postponement of marriage (lowering of fertility rate), increased cost of food etc. positive checks - famine, war, disease, would increase the death rate.
, increased cost of food etc. positive checks - famine, war, disease, would increase the death rate.")
34
Malthus (cont.) Population grows geometrically….
Population exceeds carrying capacity… Population is kept in “check”– preventative and/or positive checks

35
2. The Malthusian Crisis The “Malthusian crisis”
Available agricultural spaces are limited. Technical progresses (machinery, irrigation, fertilizers, and new types of crops) are slow to occur. Increasing incapability to support the population. If this persists, the population will eventually surpass the available resources. The outcomes are “Malthusian crises”: Food shortages. Famines. War and epidemics. “Fix” the population in accordance with available resources. Necessity of a “moral restraint” on reproduction.
 are slow to occur. Increasing incapability to support the population. If this persists, the population will eventually surpass the available resources. The outcomes are Malthusian crises : Food shortages. Famines. War and epidemics. Fix the population in accordance with available resources. Necessity of a moral restraint on reproduction.")
36
2. The Malthusian Crisis Resources Population Quantity
Technological Innovation t1 Resources Overexploitation Time

37
2. The Malthusian Crisis The Malthusian Crisis has not occurred
Malthus has been criticized on several accounts during the last 200 years. Religious view (Protestantism), racist and elitist. Did not foresee the demographic transition: Changes in the economy that changed the role of children in the industrializing societies. Failed to account for improvements in technology: Enabled food production to increase at rates greater than arithmetic, often at rates exceeding those of population growth. Enabled to access larger amounts of resources. Enabled forms of contraception.
, racist and elitist. Did not foresee the demographic transition: Changes in the economy that changed the role of children in the industrializing societies. Failed to account for improvements in technology: Enabled food production to increase at rates greater than arithmetic, often at rates exceeding those of population growth. Enabled to access larger amounts of resources. Enabled forms of contraception.")
38
Global Growth in Population and Grain (Wheat and Rice) Production, 1961-2005
Source: FAO

39
Esther Boserup’s Theory of Population Growth
In contrast to Malthus, instead of too many mouths to feed, Boserup emphasized the positive aspects of a large population; In simple terms, Boserup suggested that the more people there are, the more hands there are to work; She argued that as population increases, more pressure is placed on the existing agricultural system, which stimulates invention; The changes in technology allow for improved crop strains and increased yields.

40
Anti-populationists vs. pronatalists
Malthus– anti-populationist Echoed in recent debates by Paul Ehrlich, author of The Population Bomb; Ehrlich believed that the earth’s carrying capacity would quickly be exceeded, resulting in widespread famine and population reductions; Boserup– pronatalist (cornucopian) Echoed in recent debates by Julian Simon, who opposed Ehrlich by using economic theories; ie. Resources needed to support populations are becoming more abundant, not scarcer;
 Echoed in recent debates by Julian Simon, who opposed Ehrlich by using economic theories; ie. Resources needed to support populations are becoming more abundant, not scarcer;")
42
Possible Stage 5: Decline
Low CBR Increasing CDR Negative NIR Large Elderly Population Less Young Women having Children High Dependency Ratio---pensions, elder care

44
India’s Population policies
1952- National Family Planning Program Clinics alternative methods of birth control free or subsidized birth control Legalized abortions 1971 Sterilization for compensation---compulsory 1977 Family Planning to Family Welfare, noncompulsory 1980s and beyond Education-limited success

45
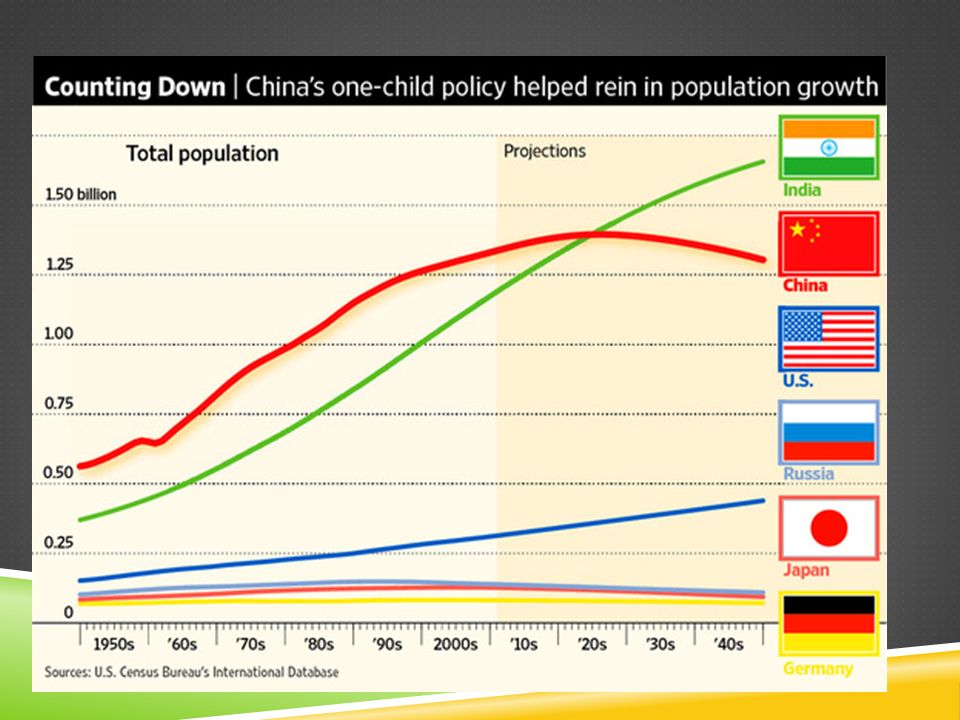
China’s Population Policies
Substantial Progress One Child Policy Permit to have a child Perks if they only have one Free contraceptives, abortions, sterilizations Enforced by the State Family Planning Commission With capitalist economy comes relaxing of rules Second child family planning fee

48
Singapore Population Policy http://hs-esl. ism-online

49
Singapore Population Policy

Similar presentations