Download presentation
Presentation is loading. Please wait.

1
Access to the sphenoid Christos Georgalas PhD MRCS DLO FRCS(ORL-HNS) Consultant Otolaryngologist Academic Medical Centre, Amsterdam 1

3
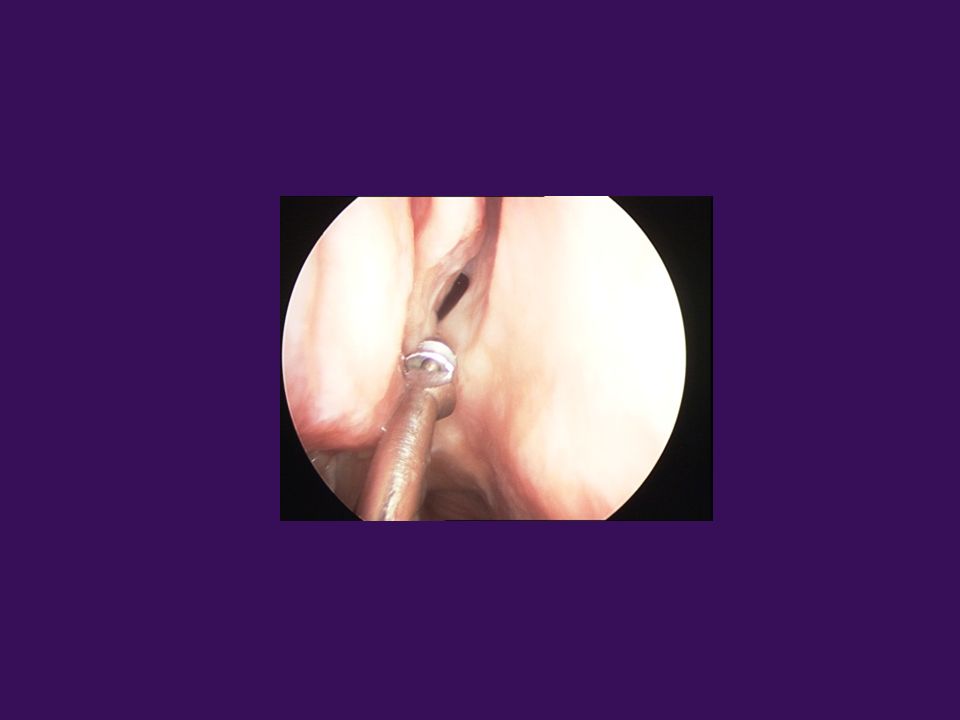
Sphenoidotomy

4
Sphenoid septae Axial CT Coronal CT Pre-clival carotid

5
Internal carotid is vulnerable
Internal carotid may project and may not be covered by bone The septae almost always end on the carotid canal Axial CT Axial CT Sphenoidectomy Septae

6
Dehiscent carotid canal (8%)
Internal carotid is vulnerable!! Dehiscent carotid canal (8%) Axial CT Axial CT !!!
 Axial CT. Axial CT. !!!")
7
Onodi Cell Sagittal CT Axial CT Coronal CT
Sphenoid sinus Surgery posterior ethmoids Coronal CT Posterior ethmoid cell that grows into the sphenoid cell and contains the optic nerve

8
Optic nerve is vulnerable!
Axial CT Sphenoid surgery 1 2 Coronal CT 2 1. Projection of the optic nerve into the sphenoid sinus 2. Dehiscent optic nerve (4%) !!! 8
 !!! 8.")
9
Types of sphenoid pneumatisation
A. Conchal) B. Pre-sellar) C.Sellar
 B. Pre-sellar) C.Sellar.")
10
Sphenoidotomy The anterior surface of the sphenoid sinus is approximately 8 cm from the nasal spine and at 15⁰ angle with the horizontal plane of nasal cavity

11
The 3+1 ways to enter the sphenoid
A. Superior turbinate Lateralise gently medial turbinate Posterior and superior to the middle turbinate you can visualise the superior turbinate - Lateralise it! Medially you will find the sphenoid ostium

12
The 3+1 ways to enter the sphenoid
B. Nasopharynx- posterior choanae Follow nasopharynx Find posterior choanae –(exactly where the posterior wall becomes from vertical horizontal) 1.6 – 2 cm above that you will find the ostium (4 – 5 times the width of a straight suction
 1.6 – 2 cm above that you will find the ostium (4 – 5 times the width of a straight suction.")
13
The 3+1 ways to enter the sphenoid
C. Through the posterior septum – rostrum (safer) Remove the mucosa from the rostrum Follow the bone laterally The ostium is cm from the septum
 Remove the mucosa from the rostrum. Follow the bone laterally. The ostium is cm from the septum.")
14
The 3+1 ways to enter the sphenoid
And the less safe way D: Through the posterior ethmoids Perforate the posterior ethmoids aiming postero medially – NOT recommended!!!!

15
Sphenoidectomy The posterior septal brach of the sphenopalatine artery runs on the frontal wall of the sphenoid – risk of troublesome (but not dangerous) bleeding The same branch is used for nasoseptal flap for skull base defects reconstruction!
 bleeding. The same branch is used for nasoseptal flap for skull base defects reconstruction!")
17
Enlarge the ostium in an inferior and medial direction with Hayeck punch or drill

18
If necessary repeat procedure on other side and combine the two enlarged openings medially. Remove distal part of the bony septum.

19
ON CA . Identify the location of the optic nerve (ON) , carotid canal (CA) and opticocarotid recess (OCR) along the lateral sphenoid wall and sella (SE) on the posterior wall SE CA SE
 , carotid canal (CA) and opticocarotid recess (OCR) along the lateral sphenoid wall and sella (SE) on the posterior wall. SE. CA. SE.")
20
Steps of Surgery NASAL PHASE Diagnostic endoscopy
Localising and opening sphenoid sinus ostium Preparing mucoseptal flap (if extended approach) SPHENOID PHASE Widening of the ostium and exposure of sphenoid sinus Exposure of the anterior sellar wall SELLAR PHASE Opening of the sella Incising the dura Tumor removal Closure of the sella Completion of surgery (application of flap, closure, packs)
 SPHENOID PHASE. Widening of the ostium and exposure of sphenoid sinus. Exposure of the anterior sellar wall. SELLAR PHASE. Opening of the sella. Incising the dura. Tumor removal. Closure of the sella. Completion of surgery (application of flap, closure, packs)")
21
Finding the Sphenoid Lateralize or remove lower half of middle turbinate if necessary– identify superior turbinate. Inferomedially to the superior turbinate is the sphenoid ostium. The sphenoid ostium is mm above the choana

22
The pedicled nasoseptal flap
Hadad G, Bassagasteguy L, Carrau RL, Mataza JC, Kassam A, Snyderman CH, Mintz A. A novel reconstructive technique after endoscopic expanded endonasal approaches: vascular pedicle nasoseptal flap. Laryngoscope Oct;116(10):
:")
23
Repeat on other side Repeat procedure on other side and combine the two enlarged openings medially. Remove distal part of the bony septum and rostrum with blakesley, punch or drill, depending on consistency Identify sella, carotid bulge, optic nerve, opticocarotid recess and planum sphenoidale – rarely also vidian nerve OCR CP S

24
Enlarge the sphenoid ostium
B. Use initially a Stammberger and subsequently a Kerrison punch – always working medially and inferiorly Try to avoid the artery running in face of sphenoid – posterior septal, providing blood supply to septum, branch of sphenopalatine

25
A long way to go In any case, these are questions that form part of the trip and not the end – of whatpromises to be a long and exciting journey, like this one in klein curacao last march. Many thanks…

Similar presentations


















 Root Ala Dorsum>")

