Download presentation
Presentation is loading. Please wait.

1
Basic Chest Radiology for the TB Clinician
PRESENTATION MATERIALS Basic Chest Radiology for the TB Clinician Adapted from the ISTC TB Training Modules 2009

2
Basic Radiology for the TB Clinician
Objectives: At the end of this presentation, participants will be able to: Analyze the technical quality of chest X-rays (CXRs) using simple parameters Identify basic normal CXR anatomy on both frontal and lateral views Recognize radiographic patterns of disease and describe using appropriate terminology Describe both the typical and atypical patterns of radiographic presentation for pulmonary tuberculosis 2
 using simple parameters. Identify basic normal CXR anatomy on both frontal and lateral views. Recognize radiographic patterns of disease and describe using appropriate terminology. Describe both the typical and atypical patterns of radiographic presentation for pulmonary tuberculosis. 2.")
3
Basic Radiology for the TB Clinician (2)
Overview: Technical aspects of chest radiography Systematic approach to reading CXR Basic CXR anatomy Patterns of disease Radiographic manifestations of tuberculosis (TB) [Image Credit: Lung Health Image Library/Gary Hampton] 3
 [Image Credit: Lung Health Image Library/Gary Hampton] 3.")
4
Chest Radiography: Basic Principles
X-ray photon: Absorbed / scattered / transmitted X-ray absorption depends on: Beam energy (constant) Tissue density Maximum X-Ray Transmission (least dense tissue) Absorption (densest tissue) Blackest air fat soft tissue calcium bone X-ray contrast metal Whitest 4
 Tissue density. Maximum X-Ray. Transmission. (least dense tissue) Absorption. (densest tissue) Blackest. air. fat. soft tissue. calcium. bone. X-ray contrast. metal. Whitest. 4.")
5
Differential X-Ray Absorption
Why we see what we see: Structures are visible on a radiograph because of the juxtaposition of two different densities creating an interface Silhouette Sign Loss of an expected interface No boundary can be seen between two structures because they now are similar in density Image credit: Curry International Tuberculosis Center, University of California, San Francisco 5

6
Silhouette Sign: RLL Pneumonia
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 6

7
Silhouette Sign: RLL Pneumonia
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 6

8
Assess CXR Technical Quality
Inspiratory effort 9-10 posterior ribs Penetration thoracic intervertebral disc space just visible Positioning / rotation medial clavicle heads equidistant from spinous process 7

9
Image credit: Curry International Tuberculosis Center, University of California, San Francisco
8 9

10
1 2 3 4 5 6 7 8 9 10 Image credit: Curry International Tuberculosis Center, University of California, San Francisco 8 10

11
1 2 3 4 5 6 7 8 9 10 Image credit: Curry International Tuberculosis Center, University of California, San Francisco 8 11

12
1 2 3 4 5 6 7 8 9 10 Image credit: Curry International Tuberculosis Center, University of California, San Francisco 8 12

13
Inspiratory Effort Low Lung Volumes Full Inspiration 9
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 9

14
Exposure Overexposure Proper Exposure 10
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 10

15
Overexposure Proper Exposure 11
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 11 15

16
Rotated (Oblique) Image credit: Curry International Tuberculosis Center, University of California, San Francisco 12 16

17
Basic Radiology for the TB Clinician
A systematic approach to reading a CXR Image Credit: Lung Health Image Library/Gary Hampton 13

18
Approach to Reading a CXR
Be Systematic Lungs Pleural surfaces Cardiomediastinal contours Bones and soft tissues Abdomen Image credit: Curry International Tuberculosis Center, University of California, San Francisco 14

19
Worth a Second Look Apices Retrocardiac areas (left and right)
Hilar regions Below diaphragm 15

20
Apical TB Image credit: Curry International Tuberculosis Center, University of California, San Francisco 16 20

21
Apical TB (2) Image credit: Curry International Tuberculosis Center, University of California, San Francisco 17

22
Left Retrocardiac Opacity
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 18 22

23
Nodule Behind Diaphragm
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 19 23

24
Basic Radiology for the TB Clinician
Basic CXR Anatomy Image credit: Curry International Tuberculosis Center, University of California, San Francisco 20

25
Basic CXR Anatomy Frontal and Lateral Views Heart Aorta
Pulmonary arteries Airways Image Credit: Lung Health Image Library/Pierre Virot 21

26
Image credit: Curry International Tuberculosis Center, University of California, San Francisco
22 26

27
Right pulmonary artery Left pulmonary artery Trachea & bronchi
Aortic arch Right pulmonary artery Left pulmonary artery Trachea & bronchi Image credit: Curry International Tuberculosis Center, University of California, San Francisco 23

28
Aortic arch Image credit: Curry International Tuberculosis Center, University of California, San Francisco 23

29
Right pulmonary artery
Aortic arch Right pulmonary artery Image credit: Curry International Tuberculosis Center, University of California, San Francisco 23

30
Right pulmonary artery Left pulmonary artery
Aortic arch Right pulmonary artery Left pulmonary artery Image credit: Curry International Tuberculosis Center, University of California, San Francisco 23

31
Right pulmonary artery Left pulmonary artery Trachea & bronchi
Aortic arch Right pulmonary artery Left pulmonary artery Trachea & bronchi Image credit: Curry International Tuberculosis Center, University of California, San Francisco 23

32
Basic Radiology for the TB Clinician
Patterns of disease 24

33
Chest Radiographic Patterns of Disease
Consolidation / air-space opacity Interstitial opacity Nodules and masses Lymphadenopathy Cysts and cavities Pleural abnormalities 25

34
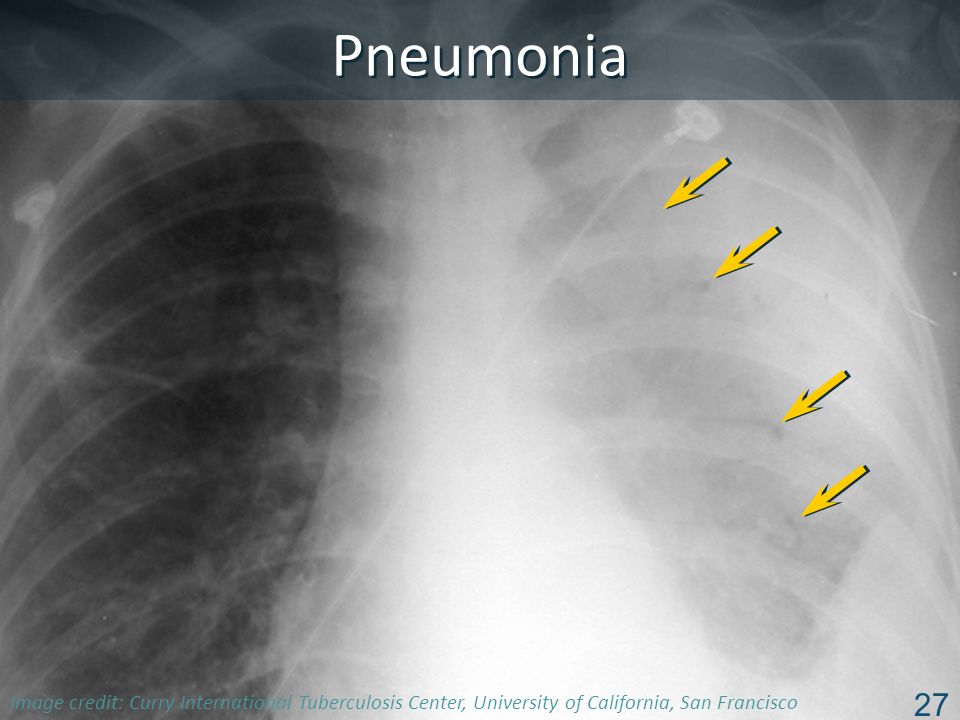
Consolidation / Air-Space Opacity
Caused by filling of alveoli with fluid, pus, blood, cells (tumor), etc. May be diffuse, or isolated to segments or lobes of the lung May be associated with air bronchograms (air-filled bronchus surrounded by opacified lung) 26
, etc. May be diffuse, or isolated to segments or lobes of the lung. May be associated with air bronchograms (air-filled bronchus surrounded by opacified lung) 26.")
35
Pneumonia Image credit: Curry International Tuberculosis Center, University of California, San Francisco 27 35
36
Interstitial Opacity Disease localized to pulmonary interstitium, i.e., the alveolar septae and connective tissues that support the alveoli Hallmarks: Lines and/or reticulation Small, well-defined nodules Miliary pattern DDX: Pulmonary edema, interstitial lung diseases (e.g., idiopathic pulmonary fibrosis), sarcoidosis, infection, tumor (lymphangitic spread), etc. 28
, sarcoidosis, infection, tumor (lymphangitic spread), etc. 28.")
37
Interstitial Opacity: Lines
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 29 37

38
Interstitial Opacity: Lines
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 29 38

39
Interstitial Opacity: Lines & Reticulation
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 30 39

40
Nodules and Masses Nodule: discrete pulmonary lesion, sharply defined, nearly circular opacity cm Mass: larger than 3 cm Describe with qualifiers: Single or multiple Size Border characteristics Presence or absence of calcification Location 31

41
Well-Defined Calcification Ill-Defined Mass 32
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 32 41

42
Lymphadenopathy (LAN)
Non-specific terms: Mediastinal widening Hilar prominence Specific patterns: Particular station enlargement (location) Important to know what “normal” should look like in order to recognize “abnormal” 33
 Important to know what normal should look like in order to recognize abnormal 33.")
43
Image credit: Curry International Tuberculosis Center, University of California, San Francisco
34 43

44
Image credit: Curry International Tuberculosis Center, University of California, San Francisco
34 44

45
Image credit: Curry International Tuberculosis Center, University of California, San Francisco
34 45

46
Image credit: Curry International Tuberculosis Center, University of California, San Francisco
34 46

47
Image credit: Curry International Tuberculosis Center, University of California, San Francisco
34 47

48
Lymphadenopathy Infrahilar window (right hilar and/or subcarinal)
Left hilar Subcarinal Image credit: Curry International Tuberculosis Center, University of California, San Francisco 35 48

49
Lymphadenopathy Infrahilar window (right hilar and/or subcarinal) 35
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 35 49

50
Lymphadenopathy Left hilar 35
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 35 50

51
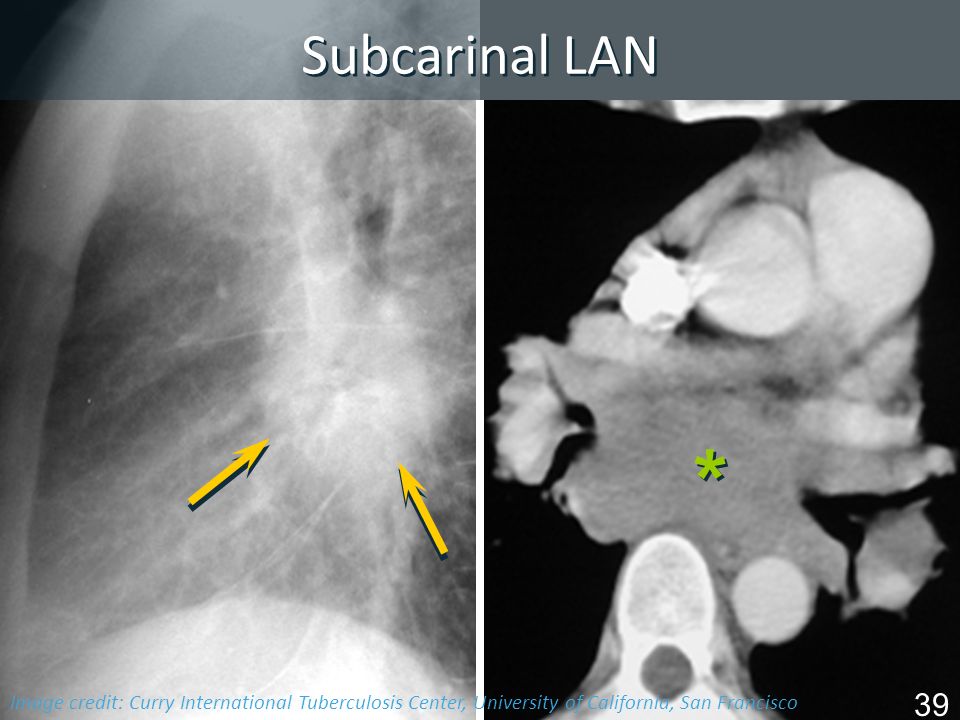
Lymphadenopathy Subcarinal 35
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 35 51

52
Right Paratracheal & Bilateral LAN
Image credit: Curry International Tuberculosis Center, University of California, San Francisco 36 52

53
Right Hilar LAN Image credit: Curry International Tuberculosis Center, University of California, San Francisco 37 53

54
Right Hilar LAN Image credit: Curry International Tuberculosis Center, University of California, San Francisco 38 54

55
Subcarinal LAN * Image credit: Curry International Tuberculosis Center, University of California, San Francisco 39 55
56
AP Window LAN Image credit: Curry International Tuberculosis Center, University of California, San Francisco 40 56

57
Cysts & Cavities Abnormal pulmonary parenchymal spaces (“holes”), filled with air and/or fluid, with a definable wall (>1 mm) Cyst: congenital or acquired Cavity: caused by tissue necrosis, (inflammatory and/or neoplastic) Characterize: Wall thickness at thickest portion Inner lining Presence / absence of air / fluid level Number and location 41
 Characterize: Wall thickness at thickest portion. Inner lining. Presence / absence of air / fluid level. Number and location. 41.")
58
TB or Not TB? Cysts and Cavities
Are there radiographic features that suggest benign vs. malignant diagnoses? A C B D “45 year old man from China with cough, weight loss” Image credit: Curry International Tuberculosis Center, University of California, San Francisco 42

59
TB or Not TB? Cysts and Cavities (2)
Are there radiographic features that suggest benign vs. malignant diagnoses? Benign cysts: uniform wall thickness, 1mm, smooth inner lining (e.g., PCP) Benign cavities: max. wall thickness 4 mm, minimally irregular inner lining (e.g., TB) Malignant cavities: max. wall thickness 16 mm, irregular inner lining 43
 Benign cavities: max. wall thickness 4 mm, minimally irregular inner lining (e.g., TB) Malignant cavities: max. wall thickness 16 mm, irregular inner lining. 43.")
60
Pleural Disease: Basic Patterns
Effusion Angle blunting to massive Thickening Mass Air Calcification 44

61
Pleural Effusion 45 61

62
Post-TB Pleural Calcification
46

63
Plombage with Lucite balls
47

64
Basic Radiology for the TB Clinician
Radiographic Manifestations of TB 48

65
Can this be TB? “Typical Pattern”: Post-primary TB Distribution
Apical / posterior segments of upper lobes Superior segments of lower lobes Isolated anterior segment involvement unusual for M.tb (think M. avium complex) 49
 49.")
66
“Typical pattern”: Post-Primary TB
Patterns of disease Air-space consolidation Cavitation, cavitary nodule Endobronchial spread Miliary Bronchostenosis Tuberculoma Pleural effusions (empyema most likely in post-primary disease) 50
 50.")
67
Can this be TB? “Atypical pattern”: Primary TB 51
Distribution : any lobe involved (slight lower lobe predominance) Air-space consolidation Cavitation is uncommon (<10%) Adenopathy is common (esp. children and HIV), predilection for right side Miliary pattern Pleural effusions 51
 Air-space consolidation. Cavitation is uncommon (<10%) Adenopathy is common (esp. children and HIV), predilection for right side. Miliary pattern. Pleural effusions. 51.")
68
Can this be TB? Miliary TB
52

69
Radiographic Patterns: Pulmonary TB
TB Pattern “Typical” (Post-Primary) “Atypical” (Primary) Infiltrate 85% upper Upper : Lower 60 : 40 Usually upper in children Cavitation Common Uncommon Adenopathy Children common Adults ~30% Unilateral > bilateral Effusion May be present 53
 Atypical (Primary) Infiltrate. 85% upper. Upper : Lower. 60 : 40. Usually upper in children. Cavitation. Common. Uncommon. Adenopathy. Children common. Adults ~30% Unilateral > bilateral. Effusion. May be present. 53.")
70
CXR Pattern: Early vs. Advanced HIV
Early HIV (CD4>200) Advanced HIV (CD4<200) Pattern “Typical” (Post-primary) “Atypical” (Primary) Infiltrate Upper lobes Lower lobes, multiple sites, or miliary Cavitation Common Uncommon Adenopathy Effusion More common 54
 Advanced HIV. (CD4<200) Pattern. Typical (Post-primary) Atypical (Primary) Infiltrate. Upper lobes. Lower lobes, multiple sites, or miliary. Cavitation. Common. Uncommon. Adenopathy. Effusion. More common. 54.")
71
Can this be TB? “Old / Healed” TB Ca++ granuloma–Ghon lesion
Ca++ granuloma and hilar node calcification–Ranke complex Apical pleural thickening Fibrosis and volume loss 55

72
Basic Radiology for the TB Clinician
Summary: Remember: Technical quality can significantly impact your CXR interpretation Develop a systematic approach (and use it every time!) Practice identifying normal CXR anatomy Important to characterize and describe lesions—this can help with your differential diagnosis Whether typical or atypical TB can always fool you! 56
 Practice identifying normal CXR anatomy. Important to characterize and describe lesions—this can help with your differential diagnosis. Whether typical or atypical. TB can always fool you! 56.")
Similar presentations



















