Download presentation
Presentation is loading. Please wait.

1
ACT in the treatment of chronic illness
JoAnne Dahl, Department of Psychology, University of Uppsala Sweden

2
Why do people get “stuck” in pain?
Riddle about Sweden When pain was unavoidable, it was bearable, when pain became avoidable, it became unbearable The solution becomes the problem.

3
Solutions for chronic pain
Evidence for most common medical treatments for pain is limited or non-existent the greater the access to quick fix solutions, the greater the pain sensitivity those societies offering most attention and solutions are those with greatest prevalence and disability

4
ACT and chronic illness
attempts to control negatively evaluated aspects of an experience may actually increase suffering in the long run: avoiding pain (symptoms) causes pain (suffering) and produces actions: narrow, rigid, less valued symptoms have been allowed to get in the “drivers seat”
 causes pain (suffering) and produces actions: narrow, rigid, less valued. symptoms have been allowed to get in the drivers seat")
5
experiential avoidance of symptoms predicts poorer long-term outcome: if you can’t stand it, you’ve got it

6
clean symptom/dirty symptoms
clean symptoms are those directly elicited by pathology (damaged tissue, dysfunctional brain activity, low insuline, allergene) dirty symptoms are the suffering caused by avoiding symptoms
 dirty symptoms are the suffering caused by avoiding symptoms.")
7
why avoiding the problem becomes the problem
There is a difference between avoiding a dangerous situation or avoiding the thought of a dangerous situation, the first will save you life the second will handicap you for life

8
T

9
Fundamental assumptions
People are capable of living a meaningful life with pain, anxiety and any other discomfort Avoidance of pain or symptoms tends to make us loose sight of valued directions and thus a loss of life quality

10
Aim of Treatment To help the person with pain to identify and act consistently with valued directions, independent of pain symptoms To create psychological flexibility when relating to discomfort generally

11
Treatment principles Valued direction in life dimensions
Exposure in valued directions: previously avoided Acceptance of what cannot be directly changed Defusion of thoughts which are not functional

12
When you alter your life in the service of reducing symptoms, your symptoms flourish and your life quality diminishes

14
Creative hopelessness
Goal Life Värden i livet arbeta vänner intimt Goal: freedom from pain Cost; I may fail Cost: loss of life quality: no friends, no job, no fun What happens when what is important hurts?

15
Mindy chatter: when I feel pain, reasons, predictions consequences
Life Restriction and loss: life skrinks, present moment disappears, vitality is lost control and avoidance cycle: moving down into struggle and away from a values-based vital life Entanglement: taking literally, mindy solutions that call for escape, avoidance, making deals, losing who you are Relief:temporary relief, illusions that mindy solutions may work this time Control and avoidance: complying with mindy solutions and buying these thoughts and engaging in the actual behavior they structure

16
Values: the life directions I choose, what I want my life to be about
Acceptance and being present: making room for pain in the moment it occurs Commitment and flexibility: choosing to take action consistent with my values, enhancing life flexibility ACT: moving up towards a values based vital life Mindfulness and defusion: observing my thoughts as thoughts, taking heed if they are helpful, staying conscous as the observer self, cognitive flexibility Growth and contact with barriers: as I step forward I grow and develop and feel pain

19
Figure 8. 3. The two cycles pain clients can choose
Figure 8.3. The two cycles pain clients can choose. The choice at the top cycles upward toward vitality, the choice at the at the bottom cycles downward into struggle. Note that both cycles involve repeated, perhaps even frequent, contact with pain. Adopted from an idea by David Chantry and modified by Hayes and Smith (in press). Pain The Acceptance and Commitment Cycle -- Moving Up Toward a Values-Based Vital Life The Control and Avoidance Cycle -Moving Down into Struggle and Away from a Values-Based Vital Life Mindfulness and defusion (Observing my thoughts as thoughts; taking heed if they are helpful; staying conscious as an observing self; enhanced cognitive flexibility) Values (The life direction I choose; what I want my life to be about) Control and Avoidance (Complying with mindy solutions by buying these thoughts and engaging in the actual behavior they structure) Acceptance and being present (Making room for pain in the moment when it occurs) Entanglement (Taking literally mindy solutions that call for escape, avoidance, making deals; losing who you are) Mindy chatter (When I feel pain my mind chatters with reasons, predictions, and comparisons) Growth and Contacted Barriers (When I step forward, especially into new territory, I grow I also often again encounter ...) and Commitment and Flexibility (Choosing to take action consistent with my values; enhancing life flexibility) Relief (A temporary respite from pain; the illusion that the mindy solutions may work this time) Life Restriction and Loss (Life shrinks; the present moment disappears; I lose vitality; and I often notice even more ...)
. Pain The Acceptance and Commitment Cycle -- Moving Up Toward a Values-Based Vital Life The Control and Avoidance Cycle -Moving Down into Struggle and Away from a Values-Based Vital Life Mindfulness and defusion (Observing my thoughts as thoughts; taking heed if they are helpful; staying conscious as an observing self; enhanced cognitive flexibility) Values (The life direction I choose; what I want my life to be about) Control and Avoidance (Complying with mindy solutions by buying these thoughts and engaging in the actual behavior they structure) Acceptance and being present (Making room for pain in the moment when it occurs) Entanglement (Taking literally mindy solutions that call for escape, avoidance, making deals; losing who you are) Mindy chatter (When I feel pain my mind chatters with reasons, predictions, and comparisons) Growth and Contacted Barriers (When I step forward, especially into new territory, I grow I also often again encounter ...) and Commitment and Flexibility (Choosing to take action consistent with my values; enhancing life flexibility) Relief (A temporary respite from pain; the illusion that the mindy solutions may work this time) Life Restriction and Loss (Life shrinks; the present moment disappears; I lose vitality; and I often notice even more ...)")
25
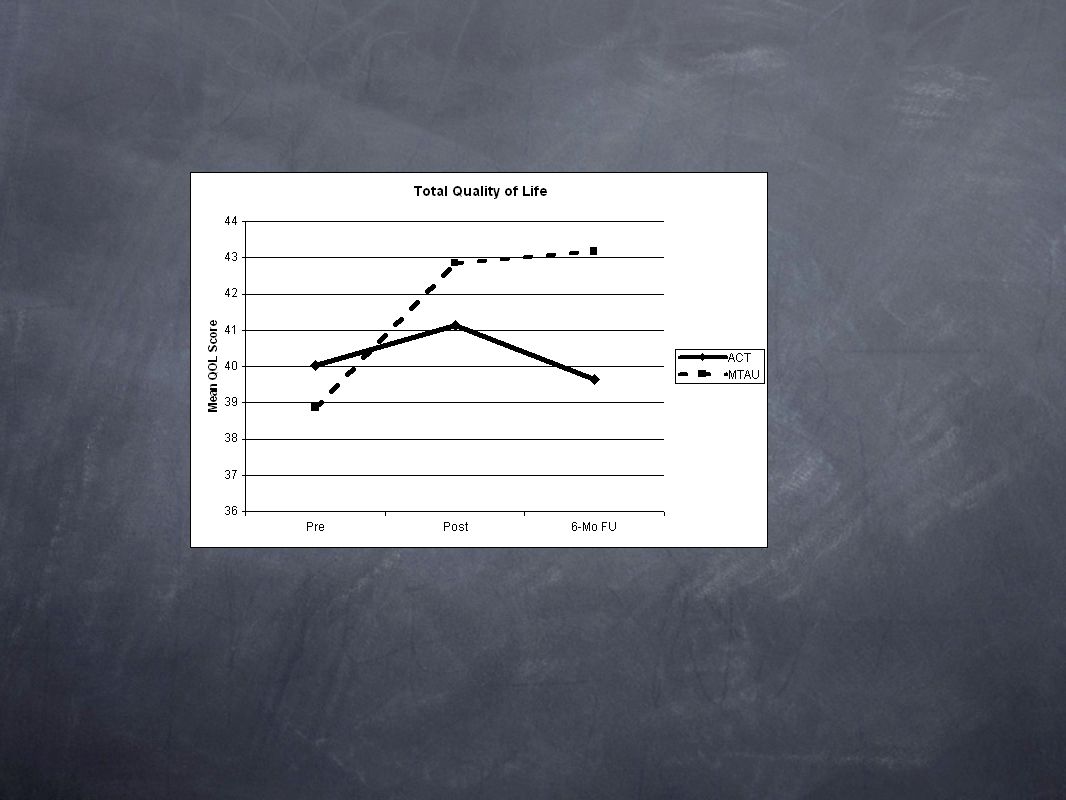
conclusions Acceptance based treatment compared to controlled based appears to lead to more promising long-term results The person with chronic pain is more interested in getting his/her life back than simply getting rid of the pain.

26
A development and evaluation of an integrative health model in treatment of epilepsy: Two randomized controlled trials investigating the effects of a short-term ACT intervention compared to attention control in India and South Africa. Tobias Lundgren, JoAnne Dahl and Lennart Melin Department of psychology, Uppsala University, Sweden

27
Design Randomized Controlled Trial Participants in South Africa = 27 Two conditions, ACT and Attention Control. Inclusion criteria: 4 seizures in the last 3 months Able and willing to participate No other ongoing illnesses Age 15 – 50

28
Evaluation of an empowerment program: ACT
Cooperative project between Epilepsy South Africa, Uppsala University Sweden and the International Bureau for Epilepsy IBE Application of an integrative health model, acceptance based behavior therapy in Epilepsy South Africa Grietha Van Wyk, Tobias Lundgren & JoAnne Dahl Department of psychology, Uppsala University, Sweden Grietha Van Wyk, Epilepsy South Africa Prof. JoAnne Dahl, Commission Chair IBE, Uppsala Univeristy Tobias Lundgren, Uppsala University, Sweden

29
• Accept your “tendency to seize” • Choose your valued direction
A Simpler Version of the Goals of ACT • Accept your “tendency to seize” • Choose your valued direction • Take action to regain your quality of life in the face of all difficulties

30
Increase in life quality for ACT group

31
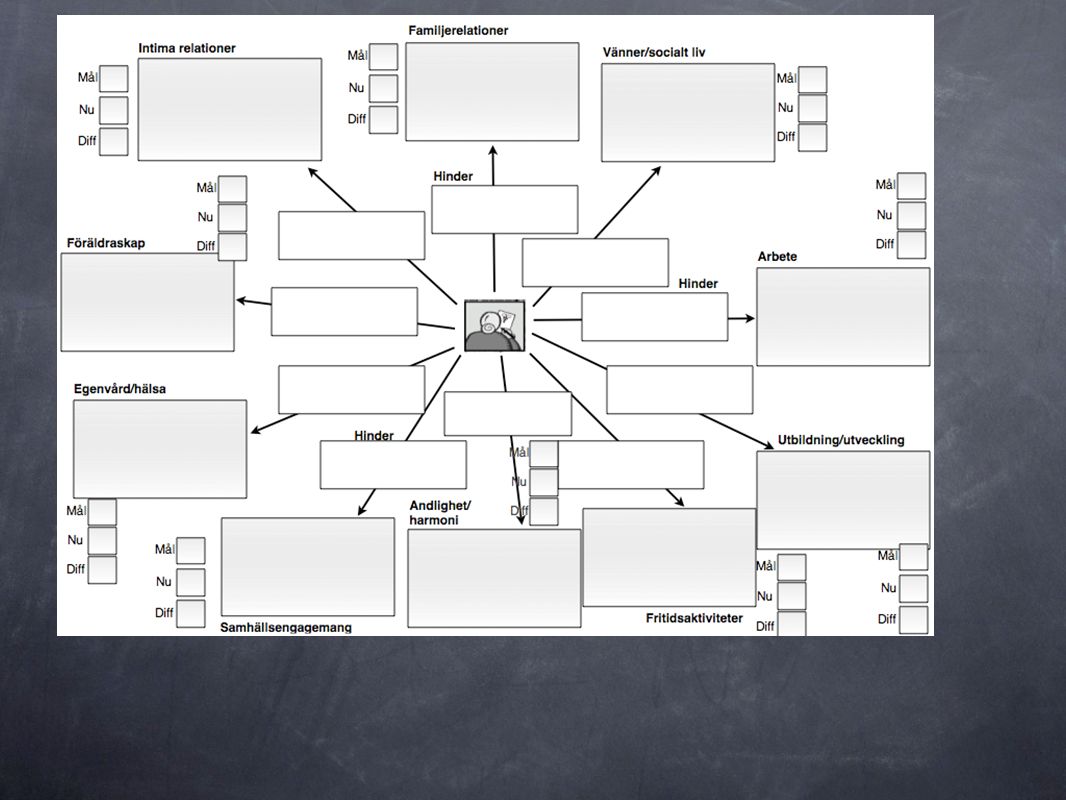
Measure of persistency in striving for living a vital life in the face of difficulties

32
Self-rating evaluation of where you place your activity level today in relation to the bull’s eye of vitality you want

33
Self rated evaluation of the degree to which epilepsy and thoughts about epilepsy is accepted or avoided

34
Future research Develop an integrative health model with a focus on empowerment of human resources to act consistent towards long term valued living. Look for the mechanism in behavior change. Training the trainers in ACT program in several Epilepsy South Africa Centers Text

Similar presentations























 233-3480 Using Creative Hopelessness to Break the Treatment Failure.>")