Download presentation
Presentation is loading. Please wait.

1
CBRN Disaster Management
Dr. Rakesh Kumar Sharma Additional Director, Institute of Nuclear Medicine and Allied Sciences, Delhi @Training Programme on Chemical (Industrial) Disaster Risk Management, August 2010
 Disaster Risk Management, August")
2
All-Hazards Natural Earthquake Landslides Floods Fires etc… Human-made
Explosive devices Firearms Structural collapse Transportation event Air, Rail, Roadway, Water HAZCHEM / HAZMAT WMD CBRN events etc…

3
CBRN Terrorism Threat: Fact or Fiction?
Radiological: trafficking in radio-isotopes but no incidents Nuclear: trafficking in plutonium and highly enriched uranium – but no incidents with improvised, stolen or sold nuclear device Chemical: Sarin attack in Tokyo’s subway system in April 1005: 12 killed, dozens wounded Biological: Anthrax attack in USA 2001: 5 killed, 22 infected 1

4
‘New’ Elements in ‘ New Terrorism’
Attempts to acquire Weapons of Mass Destruction Religious Fanaticism Catastrophic Terrorism Border Porosity Global Communication Diaspora Bridgeheads (Portable conflicts) Kamikaze Suicide Terrorism Expansion of Range of Targets (Tourists, ICRC, UN) Links with Organized Crime New Sources of Financing Failed and weak states as de facto safe havens New types of weapons (e.g. MANPADs) 1
 Kamikaze Suicide Terrorism. Expansion of Range of Targets (Tourists, ICRC, UN) Links with Organized Crime. New Sources of Financing. Failed and weak states as de facto safe havens. New types of weapons (e.g. MANPADs) 1.")
5
Emergency Vs. Disaster A SUDDEN HAPPENING WHICH REQUIRES PROMPT ACTIONS A SUDDEN & MASSIVE HAPPENING WHICH REQUIRES PROMPT AND HUGE ACTIONS

6
Al Qaeda’s Twenty-Years’ Grand Plan
Phase 1: ( ): “The Awakening”: awake the Islamic nation from its state of hibernation by causing United States to "act chaotically”. Phase 2: ( ): “Eye-Opening”: turn Iraq into a recruiting ground for young men eager to attack America; conduct “electronic jihad” Phase 3 ( ): “Arising and Standing Up” Al Qaeda focus of struggle on Syria and Turkey, also begin of confrontation with Israel Phase 4 ( ): Al Qaeda to bring about demise of Arab governments, continued attacks on oil industry, electronic attacks to undermine U.S. economy, bringing about the collapse of the dollar by promoting gold as exchange medium Phase 5 ( ): “declaration of Islamic caliphate” leading to change of int. balance of power by seeking new economic allies such as China Phase 6 ( ): “total confrontation”: the now established caliphate’s Islamic Army will achieve “definitive victory”. Source: Lawrence Wright. The Master Plan. For the new theorists of jihad, Al Qaeda is just the beginning. The New Yorker , September 11, 2006, pp.7-8; at: as of 08/10/2008.
: The Awakening : awake the Islamic nation from its state of hibernation by causing United States to act chaotically . Phase 2: ( ): Eye-Opening : turn Iraq into a recruiting ground for young men eager to attack America; conduct electronic jihad Phase 3 ( ): Arising and Standing Up Al Qaeda focus of struggle on Syria and Turkey, also begin of confrontation with Israel. Phase 4 ( ): Al Qaeda to bring about demise of Arab governments, continued attacks on oil industry, electronic attacks to undermine U.S. economy, bringing about the collapse of the dollar by promoting gold as exchange medium. Phase 5 ( ): declaration of Islamic caliphate leading to change of int. balance of power by seeking new economic allies such as China. Phase 6 ( ): total confrontation : the now established caliphate’s Islamic Army will achieve definitive victory . Source: Lawrence Wright. The Master Plan. For the new theorists of jihad, Al Qaeda is just the beginning. The New Yorker , September 11, 2006, pp.7-8; at: cur..., as of 08/10/2008.")
7
Al Qaeda on the Path to a Caliphate
Stay alive and active and show that jihad against Crusaders and Zionists is a feasible strategy Transform Al Qaeda from a militant group into a political movement Portray the GWOT as a war on Islam Trap the United States in “bleeding wars” Overthrow the government of Pakistan Crusaders and Zionist armies to leave Muslim lands defeated after the collapse of their economies. Attack with weapon of mass destruction to make USA isolationist. Provoke war between USA and Iran and Israel and Saudi Arabia Overthrow of all apostate rulers in Muslim countries Recover “every stolen Islamic land from Palestine to al-Andalus and other Islamic lands that were lost” Reunite the Ummah and establishment of a Caliphate Introduction of Salafism and Sharia law everywhere. Source: Various,;incl. Bruce Reidel. The Search for Al Qaeda. Its Leadership, Ideology, and Future. Washington, D.C. Brookings Institution Press, 2008, pp.34, 53,113, 121, 124. 1

8
Disaster- dis·as·ter n.
An occurrence causing widespread destruction and distress; a catastrophe. A grave misfortune. Informal- A total failure

9
‘Disaster’ Definition
A disaster is present when need exceeds resources! Disaster = Need > Resources -notice that this definition does not specifically deal with medical needs………….it may address any category of needs ‘Response need’ > ‘Response available’!

10
The DISASTER Paradigm D: Detection I: Incident Command S: Safety & Security A: Assess Hazards S: Support T: Triage & Treatment E: Evacuation R: Recovery This is what each letter stands for. Each action/stage is expanded upon in the following slides. This is not necessarily the order in which these actions would be taken.

11
What is CBRN? CBRN is an acronym referring to Chemical, Biological, Radiological, and Nuclear threats It is in common use worldwide, generally to refer to PROTECTIVE MEASURES taken against CBRN weapons or hazards.

15
CBRN Technologies ….. Twenty years ago …..Today
Great Technology in the hands of NATIONS Conventions in place Mainly in Military domain Military Intelligence input and War Gaming Defence Preparedness Prediction technologies Access to Technology in hands of terrorists Force Multipliers : Connections (good networking amongst themselves as well as with rogue nations) Terrorist organizations are Faster and Flexible Requires Force Multiplication for Antiterrorism, Reaction and Response Technologies Requires New Ways/Paradigms of Thinking Technologies Approach
 Terrorist organizations are Faster and Flexible. Requires Force Multiplication for Antiterrorism, Reaction and Response Technologies. Requires New Ways/Paradigms of. Thinking. Technologies. Approach.")
16
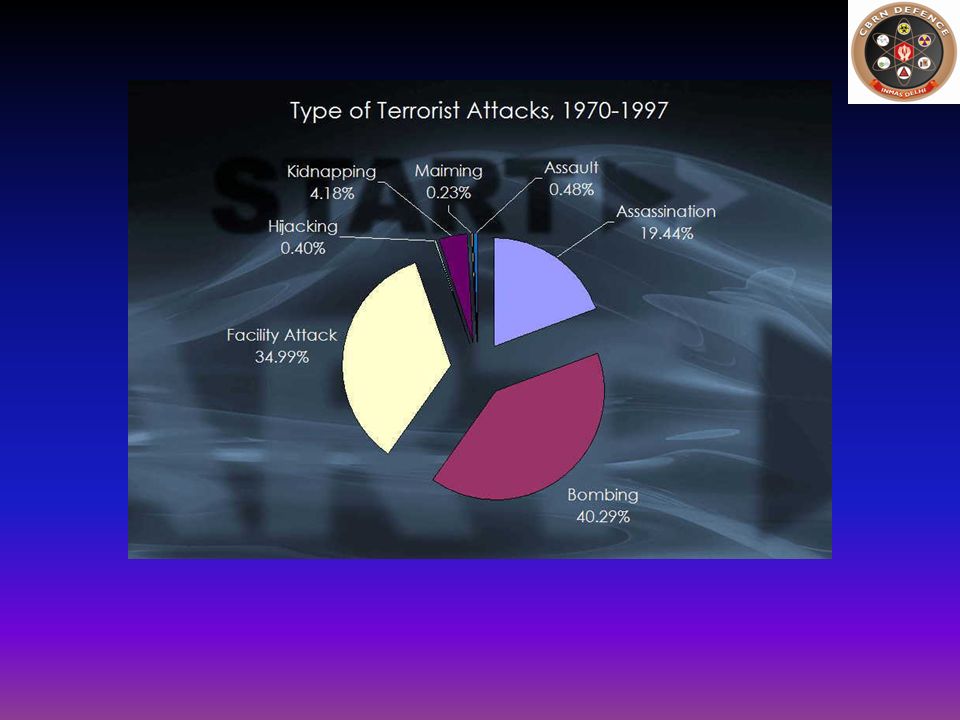
Terrorist Tactics, based on 25,303 terrorist events, 1968-2004
% of all events % of all casualties Bombs Guns Arson Remote control bombs Knives & other blades Chemical Biological Other Total Source: p.49.Kenneth T. Bogen and Edwin D. Jones. Risks of Mortality and Morbidity from Worldwide Terrorism: Risk Analysis Vol. 26, No.1, – Data utilized are from RAND-MIPT. Incidents until 1997 include only international terrorism. 1

18
List of probable agents for terrorist Attack (in descending order of likelihood)
Use of a conventional explosive Release of an industrial chemical Release of a military chemical agent Use of a ‘dirty’ bomb Release of a biological agent Detonation of a nuclear device Sharp et al. Ann Em Med;32(2):214 (1998) CDC Science & Technology Center
:214 (1998) CDC Science & Technology Center.")
19
Disruption CBRN Emergencies are Happening
We are as much a target as any other ………… …. don’t happen to places ….. happen to people ……can happen to us! Disruption CBRN Defence

20
Terrorist Groups and Unconventional Weapons
High C CR CRB CRBN Al Qaeda Danger LTTE Hizbollah AUM FARC (?) HAMAS (?) DHKP/C (?) PKK (?) BKI RIRA ETA MILF AUC IMU N17RO SL ASG Kach Chechen Rebels PIJ GSPC GIA Low High Sophistication of Unconventional Weapons
 HAMAS ( ) DHKP/C ( ) PKK ( ) BKI. RIRA. ETA MILF. AUC. IMU. N17RO. SL. ASG. Kach. Chechen Rebels. PIJ. GSPC. GIA. Low. High. Sophistication of Unconventional Weapons.")
21
Table 29 : Homeland Security Planning Scenarios 2004
1. Nuclear Detonation Can vary widely 2. Biological Attack ,000 fatalities & injuries 3. Biological Disease Outbreak (Pandemic Flu) 87,0000 fatalities, 300, hospitalized 4. Biological Attack – Plague ,500 fatalities;7,000 injuries 5. Chemical Attack – Blister Agent fatalities; 70,000 hospitalized 6. Chemical Attack –Toxic Indust. Chemicals fatalities;1, hospitalizations 7. Chemical Attack – Nerve Agent ,000 fatalities; 350 injuries 8. Chem. Attack –Chlorine Tank Explosion ,500 fatalities; 10,000 injuries 9. Radiological Attach – RDD fatalities;20, contaminations 10. Explosive Attack IED Bombing fatalities; 450 hospitalizations 11. Biological attack – Food Contamination fatalities; 400 hospitalizations
 87,0000 fatalities, 300,000 hospitalized. 4. Biological Attack – Plague 2,500 fatalities;7,000 injuries. 5. Chemical Attack – Blister Agent 150 fatalities; 70,000 hospitalized. 6. Chemical Attack –Toxic Indust. Chemicals 350 fatalities;1,000 hospitalizations. 7. Chemical Attack – Nerve Agent 6,000 fatalities; 350 injuries. 8. Chem. Attack –Chlorine Tank Explosion 17,500 fatalities; 10,000 injuries. 9. Radiological Attach – RDD 180 fatalities;20,000 contaminations. 10. Explosive Attack IED Bombing 100 fatalities; 450 hospitalizations. 11. Biological attack – Food Contamination 300 fatalities; 400 hospitalizations.")
23
The Impact Leaves a long trail of sufferings
Profound sufferings – beyond the range of normal human experience Impact is multi pronged Physical, Psychological, Economical, and Social

24
The Resultant Worst case scenario is much more threatening
Psychological vulnerability and Neuropsychological Sequelae Fear of unknown Fleeing of affected community Exponential spread of disaster victims Overwhelming of hospitals by people believing themselves to be affected Hoardings Decreased efficiency of system Collapse of civil disorder and essential services …feeling of Powerlessness, …., ….., ….. Worst case scenario is much more threatening

25
CHAOS at the Incident Site
are inevitable can not be PREVENTED TRY to Reduce chaos ASAP Organise the CHAOS

26
The Expectations …………….knee jerk reactions

27
The Expectations …………….knee jerk reactions
Overall Preparedness and Risk Reduction at all levels

28
The Expectations …………….knee jerk reactions
Overall Preparedness and Risk Reduction at all levels Contingency Planning Abilities

29
The Expectations …………….knee jerk reactions
Overall Preparedness and Risk Reduction at all levels Contingency Planning Abilities Capacity development Infrastructure Trained Human Resources

30
The Expectations …………….knee jerk reactions
Overall Preparedness and Risk Reduction at all levels Contingency Planning Abilities Capacity development Infrastructure Trained Human Resources Attitudinal Changes

31
The Expectations …………….knee jerk reactions
Overall Preparedness and Risk Reduction at all levels Contingency Planning Abilities Capacity development Infrastructure Trained Human Resources Attitudinal Changes Coordination Issues

32
‘When a disaster strikes, the Community (general population) expects branches of local, state, and Central government and NGOs to rapidly mobilize to help the impacted community.’
 expects branches of local, state, and Central government and NGOs to rapidly mobilize to help the impacted community.’")
33
Disturbing Trends of Disaster
The Sarin gas attack on the Tokyo subway, usually referred to in the Japanese media as the subway sarin incident was an act of domestic terrorism perpetrated by members of Aum Shinrikyo on March 20, 1995. Triggered by natural calamities or are man-made (unintentional/deliberate in today’s scenario)
")
34
Disturbing Trends of Disasters
Chemicals are toxic manmade compounds including those designed for warfare use or industrial use TOI dated 21st February 2007 30 120 Genie out of the bottle VERTEX OF EVIL Triggered by natural calamities or are man-made (unintentional/deliberate in today’s scenario)
")
35
Disturbing Trends of Disasters
Chlorine bombings in Iraq began in January 2007, when insurgents in Al Anbar province started using chlorine gas in conjunction with conventional vehicle-borne explosive devices. Low level exposure results in burning sensations to the eyes, nose & throat, usually accompanied by dizziness, nausea and vomiting. Higher levels of exposure can cause fatal lung damage; but because the gas is heavier than air it will not dissipate well after an explosion, and so it is generally considered ineffective as an improvised chemical weapon. Triggered by natural calamities or are man-made (unintentional/deliberate in today’s scenario)
")
36
Disturbing Trends of Disasters
January 28: A suicide bomber drove a dump truck packed with explosives and a chlorine tank into an mergency response unit compound in Ramadi. 16 people were killed in the blast. February 19: A suicide bombing in Ramadi involving chlorine killed two Iraqi security forces and wounded 16 other people. February 20: A bomb blew up a tanker carrying chlorine north of Baghdad, killing nine and emitting fumes that made 148 others ill, including 42 women and 52 children. February 21: A pickup truck carrying chlorine gas cylinders exploded in Baghdad, killing at least five people and hospitalising over 50. March 16: Three separate suicide attacks on this day used chlorine. The first attack occurred at a checkpoint northeast of Ramadi, when a truck bomb wounded one US service member and one Iraqi civilian. A second truck bomb detonated in Falluja, killing two policemen and leaving a hundred Iraqis showing signs of chlorine exposure. Forty minutes later, yet another chlorine-laden truck bomb exploded at the entrance to a housing estate south of Falluja, this time injuring 250 and according to some reports killing six. March 28: Suicide bombers detonated a pair of truck bombs, one containing chlorine, as part of a sustained attack aimed at the Fallujah Government Center. The initial bombings along with a subsequent gun battle left 14 American forces and 57 Iraqi forces wounded. April 6: A chlorine-laden suicide truck bomb detonated at a police checkpoint in Ramadi, leaving 27 dead. Thirty people were hospitalized with wounds from the explosion, while many more suffered breathing difficulties attributed to the chlorine gas. April 25: A chlorine truck bomb detonated at a military checkpoint on the western outskirts of Baghdad, killing one Iraqi and wounding two others. April 30: A tanker laden with chlorine exploded near a restaurant west of Ramadi, killing six people and wounding 10. May 16: A chlorine bomb exploded in an open-air market in the village of Aby Sayda in Diyala province, killing thirty-two people and injuring fifty. Triggered by natural calamities or are man-made (unintentional/deliberate in today’s scenario)
")
37
When evil minds combine, Good minds have to work together and combat.
NDMG CD CHEMICAL TERRORISM

38
When implementing, think
We have to be lucky all the time. They have to be lucky only once!!! When planning, think more than a terrorist! When implementing, think as a ‘poor’ victim!

39
Chemical Use by a Non-State Group or Individual
A non-state group or individual pursuing a chemical weapons capability is more likely to choose Industrial Chemicals; such agents are generally easier to handle and produce and require less specialized production equipment than do Chemical warfare agents.

40
What is the goal of the Terrorist?
If the goal is to kill a single person or small group, there are chemical agents that can accomplish a murder on a small scale. For example, Ricin, produced from castor beans kills by epidermal contact.

41
A Terrorist’s Goal may be Mass Murder
This objective is the most suitable for dissemination of a Toxic Industrial Chemical or a Chemical Weapon Chlorine is readily available. Disseminated in a closed, positive air pressure environment, it could get into the lungs of most people in the environment. In other settings, however, the difficulties of spreading chlorine outdoors and the unlikelihood of it spreading from one victim to another render it a poor open-air, urban-devastating weapon. CW agents carry the most potential to spread quickly and cause more casualties and panic

42
If the Terrorist’s Goal is a WMD
OP compounds has requisite attribute of lethality However, these are available, if at all, only from secured laboratories To obtain and transport it would entail and organized conspiracy and more a kind to an act of war than an act of terrorism Sophisticated CW agents, are similarly effective but require technical assistance in order to be obtained/manufactured

43
Qualitative Severity/ Consequence Criteria
Scale for Grading of Chemical Disasters Grades Qualitative Severity/ Consequence Criteria 1 Injuries requiring first-aid only Contained release with local environmental effect and pollution problem 2 Injuries requiring a physician’s care Uncontained release with potential for minor environment effects Chances of fire and explosion 3 Severe injuries or potential for a fatality Uncontained release with potential for moderate environment effects 4 Multiple life threatening injuries and / or fatality Uncontained release with potential for major environment effects

44
Lessons Learnt… Occurrence of chemical accidents and possibility of these manifesting in a chemical disaster remains a cause of concern Unanticipated events can lead to uncontrollable releases with devastating effects Unprecedented scale of disaster potential of a hazchem incident in terms of loss of life, health injury and evacuation needed The need for an effective Disaster Management approach to lessen disaster impact is increasingly being felt Post-BHOPAL - a new era of restructuring and inducting new hazchem control systems and procedures has emerged Chemical Disaster Management revisited

45
Gaps ……Recognition While considerable progress has been made in the last two decades in the development and implementation of regulations and programmes for the management of chemical disasters, salient gaps still exists in certain areas ……. BETWEEN THE CAPACITIES OF THE VARIOUS AUTHORITIES, LEGISLATION AND ACTUAL REQUIREMENT DURING A DISASTER Pre-disaster planning has to be dealt with at a national and individual level: At the national level this includes a coordinating body between various agencies, medical facilities which includes local ambulance services, local hospitals and a radiation injury treatment centre, preparation of a local civic bodies including the municipal corporation, water and electricity board, and the metro system, and lastly the communication system which includes a training and awareness cell and the telecommunication and telecast department.

46
NDMA Mandated to laying down policies, plans and guidelines for the Nation, State, Ministries and departments (Under Section 6 of the Disaster Management (DM) Act, 2005 State, Ministries and departments shall prepare plan for preparedness and response The National and State Disaster Management Plans will finally be approved by NDMA and respective SDMA as specified in Section 11 and Section 23- subsection 3 of DM Act, 2005 respectively NDMA to coordinate and ensure implementation of the guidelines and plans (Section 35 seeks to enjoin upon the Central Government, as it deems necessary or expedient, for the purpose of disaster management)
 Act, State, Ministries and departments shall prepare plan for preparedness and response. The National and State Disaster Management Plans will finally be approved by NDMA and respective SDMA as specified in Section 11 and Section 23- subsection 3 of DM Act, 2005 respectively. NDMA to coordinate and ensure implementation of the guidelines and plans (Section 35 seeks to enjoin upon the Central Government, as it deems necessary or expedient, for the purpose of disaster management)")
47
The role of NDMA and Govt.
The main goal of NDMA and ministries in the Central Government will be to promote the cooperation between the different sections of the government, stakeholders and the society for the promotion of Chemical Disaster-Resilient Society and the implementation of CDM action plan

48
Proactive Activities and Initiatives
Undertaken by NDMA Mainstreaming Disaster Mitigation into all Developmental Programmes; Mitigation Projects Rs Crores earmarked for medical preparedness Techno-legal and techno-financial regime to promote chemical safety and risk reduction NIDM has been tasked to developed various training modules related to chemical (industrial) disaster management Liaison with DRDO and other research organisations for development of advanced equipment / logistics for CDM Chemical Security has been identified as core issue related to chemical terrorism –addressed as separate guidelines
 disaster management. Liaison with DRDO and other research organisations for development of advanced equipment / logistics for CDM. Chemical Security has been identified as core issue related to chemical terrorism –addressed as separate guidelines.")
49
National Disaster Management Guidelines-
Management of Chemical (Terrorism) Disasters
 Disasters.")
50
National Disaster Management Guidelines: Chemical Disaster
NDMG CD

51
Core Group for Chemical Disaster Management
Lt Gen (Dr) JR Bhardwaj, Member, NDMA …… Chairman Mr. KC Gupta, NSC ………………………………. Member Dr. Indrani Chandrashekharan, MoE&F…..….….... Member Dr. KP Mishra, BARC ………………..…..…... ….. Member Maj Gen JK Bansal, DRDO…..…………………… Member Mr. S. Kumar, FICCI…..……. ……………………. Member Dr. Rakesh Dubey, DMI…..………………………. Member Dr. Rakesh Kumar Sharma, DRDO …………….... Member & Co-ordinator
 JR Bhardwaj, Member, NDMA …… Chairman. Mr. KC Gupta, NSC ………………………………. Member. Dr. Indrani Chandrashekharan, MoE&F…..….….... Member. Dr. KP Mishra, BARC ………………..…..…... ….. Member. Maj Gen JK Bansal, DRDO…..…………………… Member. Mr. S. Kumar, FICCI…..……. ……………………. Member. Dr. Rakesh Dubey, DMI…..………………………. Member. Dr. Rakesh Kumar Sharma, DRDO …………….... Member & Co-ordinator.")
52
Core Group for CIDM It is extremely important that the professional or specialised inputs are not confined only to policy-making, but are also used for its dissemination, implementation and monitoring The availability of professional expertise will be a crucial factor for the successful and sustainable implementation of the Chemical disaster management action plan Shall promote the cooperation between the different sections of the government, stakeholders and the community for promoting activities aiming towards Chemical Disaster Resilience and the implementation of CDM action plan.

53
The road map towards developing Chemical Risk Reduction and Safety
The National Disaster Management Guidelines – Chemical Disaster recognizes the following Pillars of Strength: A Rational Chemical Disaster Management Framework Emphasis on risk reduction, mitigation & awareness, while strengthening response Awareness program to sensitise and help preparedness of all stakeholders Capacity development Training, mock drills of emergency plans Compliance of MAH units to regulatory requirements Techno-legal and techno-financial regime to promote chemical safety and risk reduction

54
Focus areas requiring attention
Regulations Capacity Development Coordination Implementation

55
Focus areas requiring attention
Regulations Multiplicity Land Use Policy Codes of Practices and Procedures Safety Audits and Inspections Institutional framework Testing -On-Site and Off-Site Plan Commissioning and Decommissioning Training Capacity Development –Infrastructure & Trained Manpower Poison Centers Database management of Hazchem Control Rooms- EOCs Emergency functionaries–Hazmat Vehicles; Medical Preparedness Hazchem Transport- Highway DMP Research and Development Aspects Institutions – for conducting training and knowledge management Coordination Implementation

56
Focus areas requiring attention
Regulations Multiplicity Land Use Policy Codes of Practices and Procedures Safety Audits and Inspections Institutional framework Testing -On-Site and Off-Site Plan Commissioning and Decommissioning Training Capacity Development –Infrastructure & Trained Manpower Poison Centers Database management of Hazchem Control Rooms- EOCs Emergency functionaries–Hazmat Vehicles; Medical Preparedness Hazchem Transport- Highway DMP Research and Development Aspects Institutions – for conducting training and knowledge management Coordination Within MAH units With other MAH units With all Emergency Functionaries Response mechanisms and linkages between various levels National level Implementation

57
Focus areas requiring attention
Regulations Multiplicity Land Use Policy Codes of Practices and Procedures Safety Audits and Inspections Institutional framework Testing -On-Site and Off-Site Plan Commissioning and Decommissioning Training Capacity Development –Infrastructure & Trained Manpower Poison Centers Database management of Hazchem Control Rooms- EOCs Emergency functionaries–Hazmat Vehicles; Medical Preparedness Hazchem Transport- Highway DMP Research and Development Aspects Institutions – for conducting training and knowledge management Coordination Within MAH units With other MAH units With all Emergency Functionaries Response mechanisms and linkages between various levels National level Implementation Compliance Commensurate infrastructure and trained manpower Financial Arrangements Time bound implementation models

58
Focus areas requiring attention
Regulations Multiplicity Land Use Policy Codes of Practices and Procedures Safety Audits and Inspections Institutional framework Testing -On-Site and Off-Site Plan Commissioning and Decommissioning Training Capacity Development –Infrastructure & Trained Manpower Poison Centers Database management of Hazchem Control Rooms- EOCs Emergency functionaries–Hazmat Vehicles; Medical Preparedness Hazchem Transport- Highway DMP Research and Development Aspects Institutions – for conducting training and knowledge management Coordination Within MAH units With other MAH units With all Emergency Functionaries Response mechanisms and linkages between various levels National level Implementation Compliance Commensurate infrastructure and trained manpower Financial Arrangements Time bound implementation models

59
Guidelines for Chemical Disaster Management
NDMG CD Guidelines for Chemical Disaster Management

60
The Guideline focus on all aspects of disaster management cycle
lay stress on preparedness including prevention/ mitigation of Chemical Industrial Disasters while strengthening their emergency response. pertain to industrial installations, storage and transportation of hazardous chemicals. highlight the salient gaps evaluated based upon the critical review of the present status. have also included the latest international best practices and recent developments within the country

61
GUIDELINES for CDM– Major subheads Regulatory framework
Code of Practices, Procedures and Standards Statutory Inspection, Safety Auditing and Testing of Emergency Plans Technical and technological information Preparedness Education and Training Creation of Infrastructure Capacity Development Awareness Generation Institutional Framework Networking and Information Medical Preparedness Research and Development Response, Relief and Rehabilitation

62
Separate focus on… CDM at State and District levels Preparation of On-Site and Off-Site Emergency Plans Industrial (Chemical) Installations and Storages Management of Transport Accidents
 Installations and Storages. Management of Transport Accidents.")
63
The Guidelines………. Besides updation and strengthening of the existing CDM system, some value additions have been proposed………..

64
Issues related to multiplicity of regulations
Value Additions Issues related to multiplicity of regulations National regulation on Occupational Safety and Health National regulation on medical emergency management Regulations on storage and transportation of cryogenics Regulatory framework on safety measures for pipelines and area en-route. Establishment of a National Risk Management Framework Criterion for chemical assessment Empowerment of Factory Inspectorates to take legal actions for non-compliance of MSIHC Rules National Register on Potentially Toxic chemicals and establishment of poison centers Promotion of development and standardization of personal protective equipment

65
Value Additions Information exchange on banned/severely restricted chemicals in International trade Legislation on buffer zone (or to be referred as ‘no man’ zone) around MAH units Rules for units holding quantity marginally lower than those specified limits for MAH units including small and medium entrepreneurs (SMEs) Standardization of safety audits, inspection system and planning aspects- identification and selection of professionals organizations these of for accreditation Issues related to commissioning and decommissioning of chemical industries Promotion of International Chemicals Safety Cards (ICSCs) Critical Analysis and Documentation of major chemical accidents Third party evaluation of CDM plans
 around MAH units. Rules for units holding quantity marginally lower than those specified limits for MAH units including small and medium entrepreneurs (SMEs) Standardization of safety audits, inspection system and planning aspects- identification and selection of professionals organizations these of for accreditation. Issues related to commissioning and decommissioning of chemical industries. Promotion of International Chemicals Safety Cards (ICSCs) Critical Analysis and Documentation of major chemical accidents. Third party evaluation of CDM plans.")
66
Value Additions Promotion of chemical safety studies by the professional bodies identified with in the network of academia, institutions and industry Specialized training and retraining concepts, standardized training modules for all stakeholders Identification, budgeting and time bound provision of infrastructural facilities in installations and at district level for emergency functionaries Inventory of resources and equipment (including PPE, Hazmat etc.) at all levels and networking under a National vision- utilization of IDRN network Resources pertaining to DM and its mobilization shall be in accordance with risks being assessed Augmenting point-to-point ambulance services on Highways ERCs to also cater transport emergencies involving Hazchem Strengthening of National Disaster Response Force, Fire Services, Medical First Responders, paramedics and other emergency responders Revamping of Home Guards and Civil defence for CDM
 at all levels and networking under a National vision- utilization of IDRN network. Resources pertaining to DM and its mobilization shall be in accordance with risks being assessed. Augmenting point-to-point ambulance services on Highways. ERCs to also cater transport emergencies involving Hazchem. Strengthening of National Disaster Response Force, Fire Services, Medical First Responders, paramedics and other emergency responders. Revamping of Home Guards and Civil defence for CDM.")
67
Capacity development of medical preparedness
Value Additions Capacity development of medical preparedness Creation of trained Medical First Responders (MFRs) Initiation of training of paramedics for CDM management Creation of detection, decontamination and decorporation facilities Uniform Causality Profile and Classification of Casualties Risk Inventory and Resources Inventory Proper Chemical Casualty Treatment Kits Crisis Management Plan at Hospitals Mobile Hospitals/ Mobile Teams Medical Response to Long Term Effects Psychosocial Care for management of community behavior and response Issues related to public health response and medical rehabilitation and harmful effects on the environment
 Initiation of training of paramedics for CDM management. Creation of detection, decontamination and decorporation facilities. Uniform Causality Profile and Classification of Casualties. Risk Inventory and Resources Inventory. Proper Chemical Casualty Treatment Kits. Crisis Management Plan at Hospitals. Mobile Hospitals/ Mobile Teams. Medical Response to Long Term Effects. Psychosocial Care for management of community behavior and response. Issues related to public health response and medical rehabilitation and harmful effects on the environment.")
68
Value Additions Promotion of National Initiative of GIS based emergency planning and response by using multi-stakeholder approach Promotion of Community Awareness through: Introduction of mechanisms of surveillance, concepts of emergency action advice, dedicated DM channels and involvement of Community Information Representatives Establishment of Information Networking System by development of an exclusive CDM website for Knowledge management and two-way flow of information with standardized reporting mechanism Establish a register of relevant National and International Institutes and information exchange programme

69
Research & Development Activities –
Value Additions Research & Development Activities – Develop safer and cost effective alternative technologies for operations Development of need-based technologies for detection, protection (including for improving personal protective equipment so as to make suitable for Indian tropical conditions) Development of biosensors and newer biomarkers for detection of exposures, effect and susceptibility Research on risk management criterion for chemical safety management system Pilot Projects of data generation on newly emerging toxicants and its byproducts Mock drills –simulation model development
 Development of biosensors and newer biomarkers for detection of exposures, effect and susceptibility. Research on risk management criterion for chemical safety management system. Pilot Projects of data generation on newly emerging toxicants and its byproducts. Mock drills –simulation model development.")
70
Research & Development Activities –
Value Additions Research & Development Activities – Develop safer and cost effective alternative technologies for operations Development of need-based technologies for detection, protection (including for improving personal protective equipment so as to make suitable for Indian tropical conditions) Development of biosensors and newer biomarkers for detection of exposures, effect and susceptibility Research on risk management criterion for chemical safety management system Pilot Projects of data generation on newly emerging toxicants and its byproducts Mock drills –simulation model development
 Development of biosensors and newer biomarkers for detection of exposures, effect and susceptibility. Research on risk management criterion for chemical safety management system. Pilot Projects of data generation on newly emerging toxicants and its byproducts. Mock drills –simulation model development.")
71
Value Additions Indicators for declaration of different levels of disasters based upon the magnitude of chemical accidents Establishment of post-disaster documentation procedures, epidemiological surveys and minimum criterion for relief and rehabilitation Compensation to the non-governmental people including the community, if they are injured during any humanitarian activity Detailed guidelines for development of State, District DM plans including Off-Site and On-Site planning aspects Roles and responsibilities of different stakeholders – specifically for the districts with MAH units located at the boundary or the overlapping boundaries Mock drills to test these Off-Site and On-Site plans to standardize the response time for different responders Specialized focus on the technical improvements and preventive actions needs to be taken at Installations level Inclusion of isolated storages and storages at installations into the chemical safety management system Promotion of transportation emergency management (development of highway disaster management plans) and pipeline management system)
 and pipeline management system)")
74
National Vision for Management of Chemical Disasters
To prevent Chemical Disasters CD

75
National Vision for Management of Chemical Disasters
To prevent Chemical Disasters CD

76
National Vision for Management of Chemical Disasters
In the event of occurrence of CD, various stakeholder shall under take certain pre-planned and established Structural and Non-structural measures so as to minimize risks to health, life and environment Something may go wrong in spite of best system. History repeats itself as we don't learn from it. Many big mishaps have apparently small causes behind, which are likely to be overlooked.

77
Table 29: Possible Scale of Terrorist Attacks (1993 Estimates)
Type of Attack Possible Fatalities Estimated Likelihood Efficient biological attack 1,000,000 Very low Atomic bomb detonated in major US city 100,000 Successful attack on nuclear or toxic chemical plant 10,000 Simple, relatively inefficient biological or chemical attack in one skyscraper or stadium 1,000 Low Conventional attack on a single train or airplane 250 Suicide attack with explosives or firearms in a mall or crowded street 50-100 Modest Source: Office of Technology Assessment. Proliferation of Weapons of Mass Destruction: Assessing the Risks. U.S. Congress, 1993; cit. Michael E. O’ Hanlon et al. Protecting the American Homeland. A Preliminary Analysis. Washington, D.C., Brookings Institution Press, 2002, p.6.

78
Thanks

79
CBRN Disaster Management
Dr. Rakesh Kumar Sharma Additional Director, Institute of Nuclear Medicine and Allied Sciences, Delhi @Training Programme on Chemical (Industrial) Disaster Risk Management, August 2010
 Disaster Risk Management, August")
80
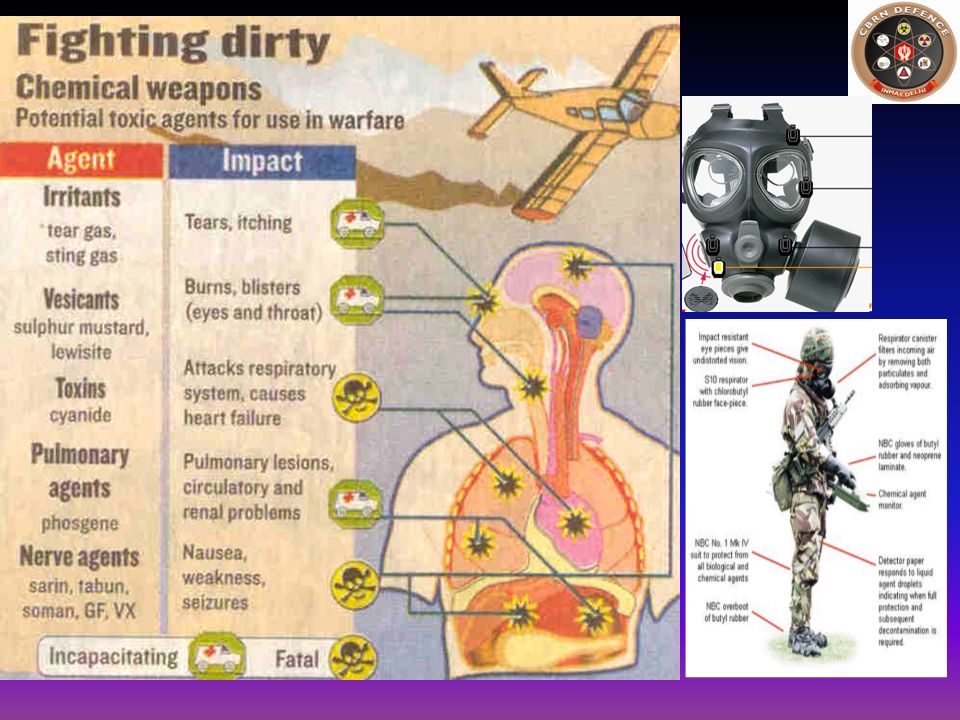
Modes of Chemical Injury
Chemical Burns (strong acids, strong bases) Heat Burns (flammable materials) Poisoning (many chemicals are damaging or fatal if taken internally, whether by swallowing, injection, or leaching through skin) Chronic illness (long-term exposure to even low doses of certain chemical agents can lead to chronic health conditions) Etc.
 Heat Burns (flammable materials) Poisoning (many chemicals are damaging or fatal if taken internally, whether by swallowing, injection, or leaching through skin) Chronic illness (long-term exposure to even low doses of certain chemical agents can lead to chronic health conditions) Etc.")
81
General Signs and Symptoms
Cough Chest pain Lacrimation Eyelid oedema and Unconsciousness Acute lung injury Leads to Cardiac arrest DEATH

82
TARGET ORGANS AND EFFECTS INDUCED BY CHEMICALS
Corneal Opacity Retinal Damage Behavior Changes Peripheral neuro degeneration Locomotion rigidity Narcosis or Depression Respiratory Paralysis Osteoporosis Arthritis Immuno Suppression Corrosiveness Erythemas Irritations Sensitization Pneumoconiosis Fibrosis Adenomas Asphyxiation MFO induction Choleostasis Carcinogenesis Necrotic/Cirrhotic liver Defense system loss Aminoacid urea Uremia Renal failure Bone marrow depression Anaemia Cancer Met hemoglobinemia Miscarriage Neonatal death Fetal abnormalities

83
Chemical Disaster Action Plan
Getting initial alert from: Police, casualty and telephone Initiate preparation All the dept & designated staff get into readiness to attend casualties Crisis expansion of hospital beds. Preparation for decontamination area Notify to Key Personnel Gather information regarding: place, time and type of emergency also type of chemical, chemical toxicity, route of exposure Mobilization of Resources Manpower: Disaster Management Team medical , nursing and other Personnel Material and supply eg: antidotes Transportation means Transport to the critical patients for medical care / hospitals Decontamination done at decontamination area in the hospital Triage Documentation done at reception Treatment to the patient (Emergency Dept.) OT IPD / ICU OPD Discharge Diagnostic Services Other support services On site treatment / operations Mass decontamination Transported in a safe place Provide necessary treatment , first aid and antidote administration to chemical contaminated patients
 OT. IPD / ICU. OPD. Discharge. Diagnostic Services. Other support services. On site treatment / operations. Mass decontamination. Transported in a safe place. Provide necessary treatment , first aid and antidote administration to chemical contaminated patients.")
84
Management of Chemical accident
Pre-hospital Hospital Post-hospital Preventive

85
CBRN Disasters Are we Prepared?

86
Predictable Surprises and System challenges
Improbable scenarios emerges every time Planning mostly fails with every new disasters We don’t have proper Plans (rudimentary!) Capacity Development not matching (un-/under Preparedness) Vibrant institutional system are not in place (tendency to maintain status quo) Regular rehearsal of Plans to check efficiency? Good Practices and Lessons Learnt not imbibed Tunnel Vision Authorities at various levels yet to incorporate and come up with implementable plans with dedicated resources
 Capacity Development not matching (un-/under Preparedness) Vibrant institutional system are not in place (tendency to maintain status quo) Regular rehearsal of Plans to check efficiency Good Practices and Lessons Learnt not imbibed. Tunnel Vision. Authorities at various levels yet to incorporate and come up with implementable plans with dedicated resources.")
87
Are We Prepared? But... Is the Healthcare System Prepared?
We appear to be… each Hospital, EMS agency, Law enforcement agency, Fire & Emergency Services, and Community has… … a disaster plan … properly documented mock exercises … annual training documented But...

88
Are We Prepared? Interagency communication failures!
Why do we all treat a cardiac arrest the same? …because there is an agreed-upon approach.

89
Are We Prepared? Critical to healthcare preparedness uniform
coordinated approach mass casualty management from any cause NEED: A need based and standardized training program As important as that is in the treatment of a cardiac arrest, it is even MORE important in the event of a large-scale, multi-agency response to a disaster. -Interoperability failures may lead to; Miscommunication / confusion / chaos Errors of omission (“I thought you guys already handled____.”) Duplication of efforts Wasted time and resources Less efficient response ( = more victims die) Injuries / deaths to responders If every is “on the same page” concerning disaster response, it greatly simplifies a potentially complex and difficult process. The best way to get everyone “on the same page” is thru a standardized, system-wide series of courses for ALL potential responders
 Duplication of efforts. Wasted time and resources. Less efficient response ( = more victims die) Injuries / deaths to responders. If every is on the same page concerning disaster response, it greatly simplifies a potentially complex and difficult process. The best way to get everyone on the same page is thru a standardized, system-wide series of courses for ALL potential responders.")
90
Why are we not prepared? Traditional approach fails
Need unique equipment and training Rupiya, Rs., ……… Fear of the unknown It can’t happen here

91
Levels of Disasters The levels of disasters have already been categorised and disseminated as L0, L1, L2 and L3, based on the ability of various authorities to deal with them. Colour codes relating to the level of alerts.

92
‘L0’ Level denotes normal times which are expected to be utilised for close monitoring, documentation, prevention, mitigation and preparatory activities. This is the planning stage where plans at all levels from community to the State shall be put in place. Training on search and rescue, rehearsals, evaluation and inventory updation for response activities will be carried out during this time.

93
‘L1’, ‘L2’, & ‘L3’ Levels L1 specifies disasters that can be managed at the district level. L2 specifies disaster situations that may require assistance and active participation of the state, and the mobilisation of resources at the state level. L3 disaster situations arise from large scale disasters where districts and the state may not have the capacity to respond adequately and require assistance from the central government for reinstating the state and district machinery. Even though there cannot be watertight compartmentalization of responsibilities between states and the centre, especially in the case of man-made disasters, the participation by the Centre will normally be at the L3 level.

94
ZONING REFERENCE TERMINOLOGY TO HELP DEFINE A SCENE LAYOUT
Permitted ENTRY - Not Dangerous - Not operational - Authorities, Media - 2nd level Triage - ICP - Fire with ordinary protect. - Medical Post - Support - 1st level Triage - Not Dangerous - Operational - Potentially Dangerous - Operational Decontamination - Fire CBRN protected - Medics CBRN prot. - Support / Backup - Dangerous - Operational - Dangerous - Not operational (not accessible) - ONLY CBRN trained & fully protected TEAMS - NOBODY closed area ( immediate danger)
 - ONLY CBRN trained & fully protected TEAMS. - NOBODY closed area ( immediate danger)")
95
ZONING REFERENCE LAYOUT
- Not Dangerous - Not operational - Authorities, Media - 2nd level Triage WIND Command Post - ICP Fire with ordinary protect. - Medical Post.. - Support - 1st level Triage - Not Dangerous - Operational DECON Decontamination - Fire CBRN protected - Medics CBRN prot. - Support / Backup - Potentially Dangerous - Operational - Dangerous - Operational - Dangerous - Not operational (not accessible) - ONLY CBRN TEAMS fully protected - NOBODY closed area ( immediate danger)
 - ONLY CBRN TEAMS fully protected. - NOBODY closed area ( immediate danger)")
96
Scenario Emergency Site Triage Area Retriage Hospitals Hot Cold Warm
Decontamination Areas, Basic First Aid Warm Retriage Cold Hospitals

98
Cardoning off the Chemical Disaster area
Wind direction Site of Disaster Medical Aid Post Control HQrs No incoming traffic except for disaster management POLICE CHECK POST No incoming traffic No incoming traffic Outer Cardon Inner Cardon No incoming traffic No incoming traffic

99
Response by DDMA in a Post-Disaster Scenario
Instantaneous instruction for forthwith movement of rescue team with personal protective equipment (PPE) Simultaneously, QRMT with PPE on will reach to Mishap site immediately along with Resuscitation, protection, detection and decontamination equipment and material. Resuscitation, triage and evacuation work must be done as per sops. DDMA will immediately inform State and National Disaster Management Authorities appraising about situation and extent of damage so that SDMA & NDMA can plan to send relief teams
 Simultaneously, QRMT with PPE on will reach to Mishap site immediately along with Resuscitation, protection, detection and decontamination equipment and material. Resuscitation, triage and evacuation work must be done as per sops. DDMA will immediately inform State and National Disaster Management Authorities appraising about situation and extent of damage so that SDMA & NDMA can plan to send relief teams.")
100
Response by DDMA in a Post-Disaster Scenario (contd)
4. Hospitals must be alerted to be ready to receive casualties 5. If there is a major chemical disaster and management is beyond the capacity of District resources. In that situation DC can request for help from adjacent district, state DMA and NDRF 6. Simultaneously, DDMA will instruct other agencies to plunge into action as per the responsibilities assigned to them

101
Standard Operating Procedures for Disaster Site
Rescue & Quick Reaction Medical Team must put on full protective gear Cordon off the Disaster Site Do not allow Entry within five kms of Disaster site Find out the wind direction & Clear the down wind side immediately Detect & Identify the Chemical Substance Demarcate the area of Contamination Do not crowd near the victim to avoid further contamination Carryout Rescue, Resuscitation & Evacuation work properly

102
Augmentation of Incident Site Management Capabilities
MANAGEMENT OF CONTAMINATION PROTECTION DETECTION DECONTAMINATION Detection/Protection Equipment (conditioned to be useful in Indian climatic conditions) Decontamination
 Decontamination.")
103
On-Site Emergency Medical Care
Health Care Centers ~ Two in perpendicular directions Inhabited with Qualified Medical Officer and male nurses ~ 24X 7 services Dedicated well equipped Ambulance with driver~ safe transportation of victim 10 bedded clinic Equipments- Oxygen Cylinders, masks, Ambu bags, First aid box, essential medicines, antidotes specific to particular hazard Minor O.T. and small laboratory to analyze routine blood samples Legal Requirements

104
Off-Site Medical Preparedness
Emergency Management at the incident Site: Personal Protective Equipment will be made available Temporary decontamination facility On-Site Triage, Resuscitation and safe transportation Safe transportation of the chemical casualties in ambulances fitted with chemical filters Evacuation Plans from Plants and nearby affected communities

105
Off-Site Medical Preparedness
Earmarking of health care facilities able to cater different types of chemical casualties like chemical burns, respiratory problems etc. Hospital disaster management plans to deal with mass casualty events caused due to chemical disasters Creation of Trained Medical First Responders Uniform Casualty Profile & their classification Risk and Resource Inventories

106
Off-Site Emergency Medical Care
Proper Chemical Causality Treatment Kits including essential medicines and antidotes Dedicated Group of Specialists to manage multi- organ dysfunctions caused by chemical exposures Provisions for mobile hospitals and teams, if needed National and Regional Poison Information Centers for information about various antidotes and treatment profiles Preparedness for Public Health and Environmental Effect Response Mechanism to follow up the long term medical care to the numerous victims

107
Guidelines for public during chemical disaster
Report about mishap to police or fire station Stay upwind & uphill Self protection by stopping breathing immediately and closing eyes Then put on the NBC protective mask Avoid contact with chemical agents Seek qualified medical advice for those persons who have been harmed by chemicals Do not eat, drink or smoke on contaminated terrain

108
POST TRAUMATIC STRESS DISORDER & ITS MANAGEMENT
PTSD is a psychological response to the experience of intense trauma due to Disaster.PTSD is characterized by Intrusive symptoms include distressing memories or images nightmares sweating, heart racing or muscle tension Avoidance symptoms of PTSD trying to avoid any reminders of the trauma, such as thoughts, feelings, conversations, activities, places and people. Arousal symptoms of PTSD include sleep disturbances, anger and irritability, concentration problems, constantly on the lookout for signs of danger

109
Post-disaster Public Health Response
Prime responsibility of medical authorities They must ensure safe water supply, clean food availability Maintenance of hygiene and sanitation by proper bio- waste disposal Water testing and food inspection must be carried out

110
Post-disaster Epidemiological Study
It must include accurate estimation of chemical exposure of effected population, correlation of environment and human exposure data, relationship of chemical and dose to the observed effect, Sub clinical effects, morbidity and mortality must also be analyzed Epidemiological studies be conducted for assessment of psychosocial effect of disaster Analysis to find out the success and failure of Disaster Management Plan and failure must be addressed Epidemiological studies team should have Clinician, Epidemiologist, Toxicologist, Pathologist, Environmental scientists and reps from Industry

111
Medical Response to Long Term Effects
In post-disaster scenario some of the casualties will develop sequel due to chemical injuries These cases may need regular follow-up, medical care, reconstructive surgery and rehabilitation Close monitoring is required to see any long term health effects like blindness, interstitial lung fibrosis and neurological deficiencies etc., and need to be treated as well

112
Post Disaster Documentation and Analysis
Information will be prepared by a medical administrator During response in hospital an information centre will provide information to public, to relatives of victims and media Warning guidelines, “DOs and DON’Ts” and condition of patients in the hospital dissemination of information to electronics and prints media will also be carried out by medical team Documentation, follow up and research programs should be used as feedback for future improvement and lessons learnt

113
Rehabilitation It involves providing temporary shelters with minimal hygiene sanitation to the affected, restoring “normalcy” through ensuring resumption of family’s daily living patterns Psychological impact of chemical disaster manifested as post traumatic stress disorders (PTSD) in displaced people due lo disaster, needs care by a psychologist and psychiatrist
 in displaced people due lo disaster, needs care by a psychologist and psychiatrist.")
114
Recovery Decontamination of the area, equipment, vehicles and disposal of left over contaminants, removal of dead bodies from site has to be carried out in the Post-disaster Scenario. It also involves restoring life of victims to normalcy.

115
Post-Disaster Emergency Medical Response
Activate resuscitation, first aid and triage system. Provide immediate relief to seriously ill and injured. Carry out resuscitation followed by decontamination Collect biological samples of casualties and sample from environment as well. Carry out proper diagnosis and proper antidote administration. Carry out simultaneous documentation of the patients. Provide accurate information to public health authority and public.

116
Develop the Dreaded Disaster Plan and Sleep Well

117
EM Plan Testing, Training & Mitigation- A Continuum
Failure to prepare is preparing to fail John Wooden

118
What Needs to be Done? Professionalizing disaster risk management
Filling knowledge gaps through information sharing, training and capacity building initiatives Networking and building partnerships among all institutions Creating environment for disaster risk management capacity Development Developing research and knowledge management systems Professionalize training and capacity development Sustainability of Initiatives

120
CBRN Emergency Scenarios
Common Indicators of CBRN Emergencies Dos and Don’ts for incident Site Management

121
Eight Sections; 177 pages; 9 Figs; 42 Tables; 8 Annexure
An Overview What to Expect? What to do in Initial Phase? Managing Afterwards Future Perspectives Conclusions Suggested Readings Annexure

122
Thanks

Similar presentations






,>")












 South Eastern Europe (SEE) PUBLIC HEALTH PREPAREDNESS SUPERCOURSE NETWORK Elisaveta Stikova,>")
 program helps train people to be better prepared to respond to emergency.>")


