Download presentation
Presentation is loading. Please wait.

1
Primary Postpartum haemorrhage
DR. FIROUZABADI

2
Postpartum Hemorrhage
EBL > 500 cc 10% of deliveries If within 24 hrs. pp = 1 pp hemorrhage If 24 hrs. - 6 wks. pp = 2 pp hemorrhage

3
Postpartum Hemorrhage
Incidence 3% of all births 6.4% of cesarean deliveries 3rd most common cause of maternal mortality Third most common cause of death behind hypertensive disease and embolism Accounts for 30% of the 500,000 annual pregnancy related deaths worldwide Postpartum hemorrhage occurs in 5% of all deliveries. slightly less common in vaginal deliveries, slightly more common in cesarians. It is the third most common cause of maternal death in the United States behind hypertensive disease and pulmonary embolism, and accounts for 30% of the 500,000 annual pregnancy related deaths worldwide.

4
Postpartum Hemorrhage
Definition greater than 500cc blood loss (vaginal delivery) or 1000cc blood loss (cesarean) decrease in HCT of 10 or greater obstetrical emergency that can follow vaginal or cesarean delivery with clinical instability leading to transfusion, shock, renal failure, acute respiratory distress, and coagulopathy Blood loss underestimated by 30-50% Blood volume expansion compensates for NORMAL loss. Diseases like preeclampsia have less expansion and tend to bleed more, putting them at risk. Postpartum hemorrhage is defined in the literature as a greater than 500 cc blood loss during a vaginal delivery, or, alternatively, as a 1000cc blood loss during a cesarian delivery. Unfortunately, these numbers are the same ones used to define normal, expected, blood loss, an indication of our collective tendency to underestimate the amount of bleeding associated with delivery. Some sources go so far as to state that blood loss is routinely underestimated by 30-50%. Thus a more objective manner of defining postpartum hemorrhage may be by serial measurements of hematocrit, or, ultimately, by the need for transfusion.
 or 1000cc blood loss (cesarean) decrease in HCT of 10 or greater. obstetrical emergency that can follow vaginal or cesarean delivery with clinical instability leading to transfusion, shock, renal failure, acute respiratory distress, and coagulopathy. Blood loss underestimated by 30-50% Blood volume expansion compensates for NORMAL loss. Diseases like preeclampsia have less expansion and tend to bleed more, putting them at risk. Postpartum hemorrhage is defined in the literature as a greater than 500 cc blood loss during a vaginal delivery, or, alternatively, as a 1000cc blood loss during a cesarian delivery. Unfortunately, these numbers are the same ones used to define normal, expected, blood loss, an indication of our collective tendency to underestimate the amount of bleeding associated with delivery. Some sources go so far as to state that blood loss is routinely underestimated by 30-50%. Thus a more objective manner of defining postpartum hemorrhage may be by serial measurements of hematocrit, or, ultimately, by the need for transfusion.")
5
Hemorrhage is the underlying causative factor in at least 25% of maternal deaths in industrialized and underdeveloped countries

6
Peripartum Hemorrhage
Causes of maternal death in US (9.1/100,000) hemorrhage: 28.7% (*) embolism: 19.7% (*) PIH: 17.6% (*) infection: 13.1% (*) anesthesia: 2.5% (*)
 hemorrhage: 28.7% (*) embolism: 19.7% (*) PIH: 17.6% (*) infection: 13.1% (*) anesthesia: 2.5% (*)")
7
Hospitalization for delivery and Availability of blood for transfusion have reduced the maternal mortality rate death from hemorrhage . It remains a cause of maternal mortality.

8
Hemorrhage is a reason for admission of pregnant women to intensive care units.
Hemorrhage has been identified as the single most important cause of maternal death, accounting for almost half of all post partum death in developing countries.

9
Incidence of obstetrical hemorrhage can not be determined precisely
Defined by a post partum HCT drop of 10 volumes percent or need for transfusion. 3.9% NVD 6-8% C/S

10
increase in blood volume . hypercoagulable state.
Maternal physiology is well prepared for hemorrhage: increase in blood volume . hypercoagulable state. the “tourniquet” effect of uterine contractions.

11
vital signs may remain near normal until more than 30% of blood volume is lost .
tachycardia can be attributed to pregnancy, stress, pain, and delivery.

12
5% of women delivering vaginally last more than 1000 ml of blood
5% of women delivering vaginally last more than 1000 ml of blood. Estimated blood loss is commonly only about half the actual loss. The effect of hemorrhage depend to a degree on the non pregnant blood volume, magnitude of PIH, degree of anemia at the time of delivery.

13
blood supply to the pelvis

14
blood supply to the pelvis
internal iliac (hypogastric) a. ovarian arteries . Are The main vascular supply to the pelvis . connected in a continuous arcade on the lateral borders of the vagina, uterus, and adnexa.
 a. ovarian arteries . Are The main vascular supply to the pelvis . connected in a continuous arcade on the lateral borders of the vagina, uterus, and adnexa.")
15
blood supply to the pelvis
/The ovarian arteries : are direct branches of the aorta beneath the renal arteries. They traverse bilaterally and retroperitoneally to enter the infundibulopelvic ligaments.

16
blood supply to the pelvis
/The hypogastric artery: retroperitoneally posterior to the ureter it divides into an anterior and posterior divisions.

17
The hypogastric artery
anterior division 5 visceral branches Uterine superior vesical middle hemorrhoidal inferior hemorrhoidal vaginal 3 parietal branches Obturator inferior gluteal internal pudendal

18
The hypogastric artery
posterior division important collateral to the pelvis. Iliolumbar lateral sacral superior gluteal

19
PHYSIOLOGY OF COAGULATION

20
PHYSIOLOGY OF COAGULATION
The four components of coagulation that continuously interrelate are (1) the vasculature, (2) platelets, (3) plasma-clotting proteins, (4) fibrinolysis.
 the vasculature, (2) platelets, (3) plasma-clotting proteins, (4) fibrinolysis.")
21
the vasculature A disruption in the vessel wall removes the protective covering of the endothelial cells and releases tissue thromboplastin, which activates the clotting mechanism.

22
platelets Activation of surface receptors causes morphologic changes in the platelets (changing first to a sphere and then to a spiderlike structure with pseudopods) and the generation of thromboxane A2 These lead to platelet aggregation and eventual formation of a platelet plug.
 and the generation of thromboxane A2 These lead to platelet aggregation and eventual formation of a platelet plug.")
23
plasma-clotting proteins
Activation of the clotting system is initiated in two ways: the intrinsic or extrinsic pathway.

24
Intrinsic Pathway requires no extravascular component for initiation and begins with Factor XII, which is activated by contact with injured epithelium.

25
Extrinsic Pathway is activated by the tissue factor thromboplastin (which subsequently activates Factor VII) when vascular disruption occurs. Prothrombin is converted to thrombin, which catalyzes the conversion of fibrinogen to fibrin. A clot is eventually formed at the site of vascular injury.
 when vascular disruption occurs. Prothrombin is converted to thrombin, which catalyzes the conversion of fibrinogen to fibrin. A clot is eventually formed at the site of vascular injury.")
26
fibrinolysis plasma substrate plasminogen is activated This substrate is converted to the active enzyme plasmin, which lyses fibrin clots and destroys fibrinogen and Factors XII and VII.

27
Etiology of PPH

28
Etiology of PPH tone, tissue, trauma, thrombin
The causes of postpartum hemorrhage can be thought of as the four Ts: tone, tissue, trauma, thrombin

29
Etiology of PPH Uterine atony Multiple gestation, high parity,
prolonged labor chorioamnionitis, augmented labor, tocolytic agents

30
Retained uterine contents
Etiology of PPH Retained uterine contents Products of conception, blood clots

31
Etiology of PPH Placental abnormalities Accreta Congenital
Bicornuate uterus Location Placenta previa Attachment Acquired structural Leiomyoma, previous surgery Peripartum Uterine inversion, uterine rupture, placental abruption Accreta

32
Lacerations and trauma
Etiology of PPH Lacerations and trauma Unplanned Vaginal/cervical tear, surgical trauma Planned Cesarean section, episiotomy

33
Acquired Etiology of PPH Congenital Coagulation disorders DIC,
dilutional coagulopathy, heparin Congenital Von Willebrand's disease

34
prevention

35
Women in whom these factors have been identified should be advised to deliver in a specialist obstetric unit odds ratio for PPH Risk Factor 13 12 5 4 Proven abruptio placentae Known placenta praevia Multiple pregnancy Pre-eclampsia/gestational hypertension

36
The following factors, becoming apparent during labour and delivery are associated with an increased risk of PPH. odds ratio for PPH Risk factor 9 4 5 2 Delivery by emergency Caesarean section Delivery by elective Caesarean section Retained placenta Mediolateral episiotomy Operative vaginal delivery Prolonged labour (>12 hours) Big baby (>4 kg)
 Big baby (>4 kg)")
37
In the event of a woman coming to delivery while receiving therapeutic heparin,
the infusion should be stopped. Heparin activity will fall to safe levels within an hour. Protamine sulphate will reverse activity more rapidly, if required.

38
Antenatal assessment anemia
Detection of anemia more than physiologic anemia of pregnancy is important, because anemia at delivery increases the likelihood of a woman requiring blood transfusion.

39
management

40
Guideline by the RCOG COMMUNICATE. RESUSCITATE. MONITOR / INVESTIGATE.
STOP THE BLEEDING.

41
COMMUNICATE call 6 Call experienced midwife
Call obstetric registrar & alert consultant Call anaesthetic registrar , alert consultant Alert haematologist Alert Blood Transfusion Service Call porters for delivery of specimens / blood

42
RESUSCITATE IV access with 14 G cannula X 2 Head down tilt
Oxygen by mask, 8 litres / min Transfuse Crystalloid Colloid once 3.5 litres infused, GIVE ‘O NEG’ If no cross-matched blood available OR give uncross-matched own-group blood, as available Give up to 1 liter Fresh Frozen Plasma and 10 units cryoprecipitate if clinically indicated

43
MONITOR / INVESTIGATE Cross-match 6 units Full blood count
Clotting screen Continuous pulse / BP / ECG / Oximeter Foley catheter: urine output CVP monitoring

44
STOP THE BLEEDING Exclude causes of bleeding other than uterine atony
Ensure bladder empty Uterine compression IV syntocinon 10 units IV ergometrine 500 mg Syntocinon infusion (30 units in 500 ml) prostaglandins Surgery earlier rather than late Hysterctomy early rather than late
 prostaglandins. Surgery earlier rather than late. Hysterctomy early rather than late.")
45
If conservative measures fail to control haemorrhage, initiate surgical haemostasis SOONER RATHER THAN LATER laparotomy Bilateral ligation of uterine arteries Bilateral ligation of internal iliac (hypogastric arteries) Hysterectomy
 Hysterectomy.")
46
Resort to hysterectomy SOONER RATHER THAN LATER (especially in cases of placenta accreta or uterine rupture)
")
47
Whole blood frequently is used for rapid correction of volume loss because of its ready availability, but component therapy is ideal. A general practice has been to transfuse 1 unit of fresh-frozen plasma for every 3 to 4 units of red cells given to patients who are bleeding profusely

48
Genital tract lacerations
Genital trauma always must be eliminated first if the uterus is firm.

49
Management of uterine atony
Explore the uterine cavity. Inspect vagina and cervix for lacerations. If the cavity is empty, Massage and give methylergonovine 0.2 mg, the dose can be repeated every 2 to 4 hours. Rectal 800mcg. Misoprostol is beneficial.

50
Uterine Atony: Prostaglandins
myometrial intracellular free Ca++, enhance action of other oxytocics Side effects: fever, nausea/vomiting, diarrhea 15-methyl PG F2 (Carboprost, Hemabate) may cause bronchospasm, altered VQ, shunt, hypoxemia, HTN 250 g IM or intramyometrially q min, up to max 2 mg. contraindications: asthma, hypoxemia
 may cause bronchospasm, altered VQ, shunt, hypoxemia, HTN. 250 g IM or intramyometrially q min, up to max 2 mg. contraindications: asthma, hypoxemia.")
51
Management of uterine atony
During the administration of uterotonic agents, bimanual compression may control hemorrhage. The physician places his or her fist in the vagina and presses on the anterior surface of the uterus while an abdominal hand placed above the fundus presses on the posterior wall. This while the Blood for transfusion made available.

52
Retained placenta Retained placental fragments are a leading cause of early and delayed postpartum hemorrhage. Treatment is manual removal, General anesthesia with any volatile agent (1.5–2 minimum alveolar concentration (MAC)) may be necessary for uterine relaxation On rare occasions, a retained placenta is an undiagnosed placenta accreta, and massive bleeding may occur during attempted manual removal.
) may be necessary for uterine relaxation. On rare occasions, a retained placenta is an undiagnosed placenta accreta, and massive bleeding may occur during attempted manual removal.")
53
Placenta accreta Placenta accreta is defined as an abnormal implantation of the placenta in the uterine wall, of which there are three types: (1) accreta vera, in which the placenta adheres to the myometrium without invasion into the muscle. (2) increta, in which it invades into the myometrium. (3) percreta, in which it invades the full thickness of the uterine wall and possibly other pelvic structures, most frequently the bladder.
 accreta vera, in which the placenta adheres to the myometrium without invasion into the muscle. (2) increta, in which it invades into the myometrium. (3) percreta, in which it invades the full thickness of the uterine wall and possibly other pelvic structures, most frequently the bladder.")
54
Placenta accreta In a patient with a previous cesarean section and a placenta previa: Previous one has 14% risk of placenta accreta. Previous two has 24% risk of placenta accreta. Previous three has 44% risk of placenta accreta.

55
UTERINE RUPTURE Rupture of the uterus is described as complete or incomplete and should be differentiated from dehiscence of a cesarean section scar.

56
UTERINE RUPTURE The reported incidence for all pregnancies is 0.05%,
After one previous lower segment cesarean section 0.8% After two previous lower segment cesarean section is 5% all pregnancies following myomectomy may be complicated by uterine rupture.

57
UTERINE RUPTURE Complete rupture describes a full-thickness defect of the uterine wall and serosa resulting in direct communication between the uterine cavity and the peritoneal cavity.

58
UTERINE RUPTURE Incomplete rupture describes a defect of the uterine wall that is contained by the visceral peritoneum or broad ligament. In patients with prior cesarean section,

59
UTERINE RUPTURE dehiscence describes partial separation of the scar with minimal bleeding, with the peritoneum and fetal membranes remaining intact.

60
Management of Rupture Uterus
The identification or suspicion of uterine rupture must be followed by an immediate and simultaneous response from the obstetric team. Surgery should not be delayed owing to hypovolemic shock because it may not be easily reversible until the hemorrhage is controlled.

61
Management of Rupture Uterus
Upon entering the abdomen, aortic compression can be applied to decrease bleeding. Oxytocin should be administered to effect uterine contraction to assist in vessel constriction and to decrease bleeding. Hemostasis can then be achieved by ligation of the hypogastric artery, uterine artery, or ovarian arteries.

62
Management of Rupture Uterus
At this point, a decision must be made to perform hysterectomy or to repair the rupture site. In most cases, hysterectomy should be performed. In selected cases, repair of the rupture can be attempted. When rupture occurs in the body of the uterus, bladder rupture must be ruled out by clearly mobilizing and inspecting the bladder to ensure that it is intact. This avoids injury on repair of the defect as well.

63
Management of Rupture Uterus
A lower segment lateral rupture can cause transection of the uterine vessels. The vessels can retract toward the pelvic side wall, and the site of bleeding must be isolated before placing clamps to avoid injury to the ureter and iliac vessels. Typically, longitudinal tears, especially those in a lateral position, should be treated by hysterectomy, whereas low transverse tears may be repaired.

64
Uterine Artery Ligation
Uterine artery ligation involves taking large purchases through the uterine wall to ligate the artery at the cervical isthmus above the bladder flap .

65
Hypogastric Artery Ligation
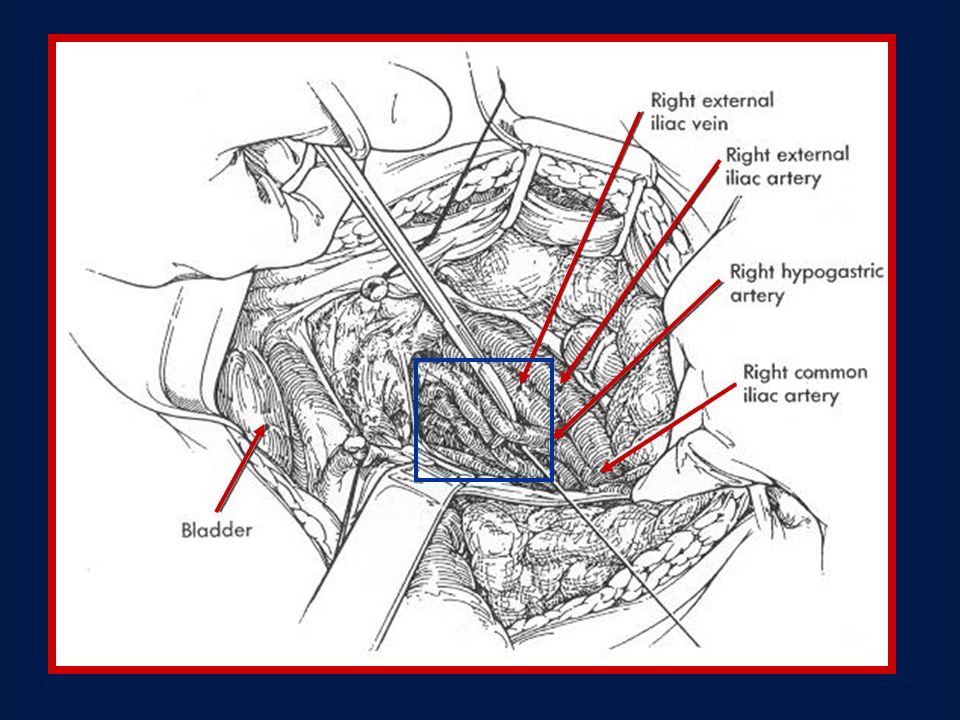
The hypogastric artery is exposed by ligating and cutting the round ligament and incising the pelvic sidewall peritoneum cephalad, parallel to the infundibulopelvic ligament The ureter should be visualized and left attached to the medial peritoneal reflection to prevent compromising its blood supply.

66
Hypogastric Artery Ligation
. The common, internal, and external iliac arteries must be identified clearly. The hypogastric vein, which lies deep and lateral to the artery, may be injured as instruments are passed beneath the artery, resulting in massive, potentially fatal bleeding.

67
Hypogastric Artery Ligation
The hypogastric artery should be completely visualized. A blunt-tipped, right-angle clamp is gently placed around the hypogastric artery, 2.5 to 3.0 cm distal to the bifurcation of the common iliac artery. Passing the tips of the clamp from lateral to medial under the artery is crucial in preventing injuries to the underlying hypogastric vein .

69
Hypogastric Artery Ligation
the artery is double-ligated with a nonabsorbable suture, with 1-0 silk, but not divided .The ligation is then performed on the contralateral side in the same manner.

70
Thank you ?

71
The Use of Blood and Blood Components
Various blood components and how they function The indications and contraindications for use

72
Red Blood Cells - RBC Description:
Whole blood is collected into an anticoagulant then centrifuged to separate the red cells from the plasma. The plasma is then expressed from the whole blood bag and the remaining red blood cells (RBC) are filtered. The filtering process removes all but 5 x 106 white blood cells (WBCs). 85% of the original RBC volume will remain after filtration. A typical unit has a volume of mL and a hematocrit of 80%.
 are filtered. The filtering process removes all but 5 x 106 white blood cells (WBCs). 85% of the original RBC volume will remain after filtration. A typical unit has a volume of mL and a hematocrit of 80%.")
73
Red Blood Cells - RBC Function:
Increase the oxygen carrying capacity of the blood by increasing the circulating red blood cell mass. Carry oxygen and nourishment to the tissues and take away carbon dioxide.

74
Red Blood Cells - RBC Indications:
Component of choice for virtually all patients with a deficit of oxygen carrying capacity, e.g., blood loss or anemia. The majority of the WBC are removed thereby decreasing the risk of cytomegalovirus (CMV) infection in immunocompromised patients. This is because the CMV virus is carried in the WBC. Use of RBC reduces the risk of the patient forming antibodies against WBC (HLA) antigens. This is especially important for potential organ or bone marrow transplant candidates.
 infection in immunocompromised patients. This is because the CMV virus is carried in the WBC. Use of RBC reduces the risk of the patient forming antibodies against WBC (HLA) antigens. This is especially important for potential organ or bone marrow transplant candidates.")
75
Red Blood Cells – RBC Contraindications:
RBC should not be used: when anemia can be corrected with specific medications, e.g., iron, B12, folic acid, erythropoietin, etc for volume replacement

76
Platelets – PC Descriptions:
Platelets are prepared from a random unit of whole blood collected in CP2D anticoagulant solution and filtered to remove leukocytes. PC contain less than 8.3 x 106 leukocytes. Platelets are suspended in a small amount of the original plasma. A unit contains at least 55 x 109 platelets suspended in mL of plasma. Trace amounts of red blood cells can be present in some units. These will appear pink to salmon colored. Platelets may also be obtained by apheresis

77
Platelets - PC Function:
The primary role of platelets is to prevent bleeding of injured blood vessel walls by forming an aggregate at the site of injury. Platelets also participate in blood coagulation, inflammation and wound healing. The transfusion of platelets to a patient with thrombocytopenia or bleeding should produce a rise in the platelet count and control bleeding.

78
Platelets - PC Indications:
For treatment of patients with bleeding due to severely decreased production or abnormal function of platelets. Treatment of bleeding patients with platelet consumption or dilutional thrombocytopenia (in most instances of dilutional thrombocytopenia, bleeding stops without transfusion). Useful if given prophylacticaly to patients with rapidly falling or low platelet counts, less than 10 x 109/L (10,000/uL), secondary to cancer or chemotherapy. Useful in selected cases of postoperative bleeding with platelet count less than 50 x 109/L (50,000/uL).
. Useful if given prophylacticaly to patients with rapidly falling or low platelet counts, less than 10 x 109/L (10,000/uL), secondary to cancer or chemotherapy. Useful in selected cases of postoperative bleeding with platelet count less than 50 x 109/L (50,000/uL).")
79
Platelets – PC Contraindications:
Platelets should not be used if bleeding is unrelated to decreased numbers or abnormal platelet function. Should not be used in patients with consumption of endogenous and exogenous platelets, such as in Thrombotic Thrombocytopenia Purpura (TTP) or Idiopathic Thrombocytopenia Purpura (ITP), unless the patient has a life threatening hemorrhage.
 or Idiopathic Thrombocytopenia Purpura (ITP), unless the patient has a life threatening hemorrhage.")
80
Platelet Incubator Stored with constant agitation

81
Fresh Frozen Plasma - FFP Description:
Fresh frozen plasma is separated from whole blood and frozen within 8 hours of collection. It can be obtained from a whole blood donation (approx. 250 mL) or by apheresis (approx. 500 mL). Fresh frozen plasma contains a normal concentration of fibrinogen and the labile coagulation factors VIII and V.
 or by apheresis (approx. 500 mL). Fresh frozen plasma contains a normal concentration of fibrinogen and the labile coagulation factors VIII and V.")
82
Fresh Frozen Plasma – FFP Function:
Fresh frozen plasma contains the clotting factors that are necessary for hemostasis. Plasma also has volume expansion and oncotic properties.

83
Fresh Frozen Plasma – FFP Indications:
The majority of clinical situations for which FFP is currently used do not require FFP. FFP is indicated for massive transfusion (replacement of the patient’s blood volume in < 24 hours) with a demonstrated deficiency of Factor VIII and V, otherwise frozen plasma is adequate. Fresh frozen plasma is also indicated in exchange transfusion in neonates.
 with a demonstrated deficiency of Factor VIII and V, otherwise frozen plasma is adequate. Fresh frozen plasma is also indicated in exchange transfusion in neonates.")
84
Fresh Frozen Plasma – FFP Contraindications:
Fresh frozen plasma should not be used when a coagulopathy can be corrected more effectively with specific therapy, such as vitamin K, cryoprecipitate, or Factor VIII concentrates. Fresh frozen plasma has the same infectious disease risk as whole blood. Fresh frozen plasma should not be used when the blood volume can be replaced with other volume expanders such as 0.9% sodium chloride, lactated ringer’s, albumin or pentaspan.

85
Frozen Plasma – FP Frozen plasma is prepared from whole blood, collected in CP2D anticoagulation solution. The plasma is separated after cold centrifugation and processed to the frozen state within 24 hours of collection.

86
Frozen Plasma – FP Frozen plasma contains stable coagulation factors such as Factor IX and fibrinogen in concentrations similar to FFP, but reduced amounts of Factor V and VIII. On average, each unit of frozen plasma contains an average of 250 mL (>100 mL) of anticoagulated plasma. The indications and side effects are the same as for FFP, except that FP should not be used to treat coagulation factor deficiencies of Factor V and Factor VIII.
 of anticoagulated plasma. The indications and side effects are the same as for FFP, except that FP should not be used to treat coagulation factor deficiencies of Factor V and Factor VIII.")
87
Fresh Frozen Plasma (FFP)
Unit of FFP (Approx mL) Apheresis FFP (Approx. 500 mL)
 Apheresis FFP. (Approx. 500 mL)")
88
Cryoprecipitate (Cryo) Description:
Cryoprecipitate is prepared by thawing fresh frozen plasma at a temperature between 1°C and 6°C. After centrifugation, the supernatant plasma is removed and the insoluble cryoprecipitate is refrozen. On average, each unit of cryoprecipitate contains 80 IU or more Factor VIII (FVIII:C) and at least 150 mg of fibrinogen in 5-15 mL of plasma.
 and at least 150 mg of fibrinogen in 5-15 mL of plasma.")
89
Cryoprecipitate (Cryo) Function:
Cryoprecipitate provides a source of coagulation factors. Factor VIII, Factor XIII and von Willebrand Factor. Fibrinogen and fibronectin are present.

90
Cryoprecipitate (Cryo) Indications:
Currently the main indication for this component is as a source of fibrinogen or Factor XIII. It may be used as a source of Factor VIII only when inactivated fractionation products or recombinant Factor VIII are not available.

91
Cryoprecipitate (Cryo) Contraindications:
Cryoprecipitate should not be used unless results of laboratory studies indicate a specific hemostatic defect for which this product is indicated. Specific factor concentrates are preferred, when available, because of their reduced risk of transmissible diseases (because of viral inactivation during manufacturing). Cryoprecipitate can be used to make fibrin glue. Alternatively, virally inactivated commercial products can be purchased for this purpose.
. Cryoprecipitate can be used to make fibrin glue. Alternatively, virally inactivated commercial products can be purchased for this purpose.")
92
Cryoprecipitate (Cryo)
Pooling Cryoprecipitate

93
Blood & its Usage

94
Components Cells Plasma molecules & ions water

95
Function Medium of transport Oxygen Carbon dioxide Other gases Ions
Carbohydrates, proteins, fats Immune response Humoral cellular

96
Cells Erythrocyres White cells Granulocyes neutophiles Eosinophiles
Basophiles Lymphocyes Monocytes Platelets

97
Molecules & ions Ions Molecules Na+, Cl-, K+, HCO2-, etc
Proteins – enzymes, precursors, active agents, immunoglobulins, carriers Proteoglycans Lipoproteins

98
Body Water Intracellular 55% Interstitial Fluid 20% Plasma 7.5%
Connective Tissue 7.5% Bone Water 7.5% Transcellular Fluid 2.5%

99
Blood products Whole blood Blood components Plasma fractions Red cells
Platelets Granulocytes Whole plasma (FFP, reconstituted) Cryoprecipitate Plasma fractions Clotting factor concentrates Immunoglobulin preparations Saline albumin solution Salt-poor albumin
 Cryoprecipitate. Plasma fractions. Clotting factor concentrates. Immunoglobulin preparations. Saline albumin solution. Salt-poor albumin.")
100
Volume replacement Haemorrhage or burns
Replacement with RBC mass at early stage necessary in massive haemorrhage Initiate with rapid transfusion of plasma expanders, electrolyte solutions & get blood type & match in 30 minutes Unmatched Grp O Rh- blood rarely justified

101
Massive Blood Transfusion
pH & K+ increase impair myocardial function Citrate lowers ionised Ca++ Significant hypothermia Platelet & WBC aggregates precipitate ARDS

102
Prevention 1 unit of fresh blood for every 5 – 10 units of stored blood IV 10% calcium gluconate 10 mls with every litre of transfused citrated blood Warming blood Microaggregate blood filters

103
Fresh Blood DIVC Massive haemorrhage Major liver trauma
Bleeding associated with liver disease

104
Clotting factors Clotting disorders Haemophilia Liver disease

105
Complications of Blood Transfusion
Febrile reactions Bacterial contamination Immune reactions Physical complications Circulatory overload Air embolism Pulmonary embolism Thrombophlebitis ARDS

106
Complications of Blood Transfusion
Metabolic complications Hyperkalaemia Citrate toxicity & hypocalcaemia Release of vasoactive peptides Release of plasticizers from PVC-phthalates Haemorrhagic reactions After massive transfusion of stored blood Disseminated intravascular coagulation

107
Complications of Blood Transfusion
Transmission of disease Hepatitis, CMV. EBV AIDS (Factor VIII) Syphilis Brucellosis Toxoplasmosis Malaria Trypanosomiasis Haemosiderosis After repeated transfusion in patients with haematological diseases
 Syphilis. Brucellosis. Toxoplasmosis. Malaria. Trypanosomiasis. Haemosiderosis. After repeated transfusion in patients with haematological diseases.")
108
Autologous transfusion
Uses pt own blood Remove 500 ml & store 2 weeks later, may be transfused in op or 1000 mls taken to increase the stored amount Multiplier effect No danger of transmitted infections

Similar presentations


: leading cause of maternal mortality worldwide Prevalence rate: 6% Africa has highest prevalence.>")

 产后出血 林建华. Major causes of death for pregnancy women ( maternal mortality) Postpartum hemorrhage ( 28%) heart diseases pregnancy-induced.>")

 and abnormalities of the Third Stage Sept 12 – Dr. Z. Malewski.>")












