Download presentation
Presentation is loading. Please wait.

1
Child with gastrointestinal dysfunctions
Emad Al Khatib, RN,MSN,CNS

2
Appendicitis The appendix is a small finger-shaped tube that branches off the first part of the large intestine. The appendix can become inflamed or infected causing pain in the lower right part of the abdomen.

3
Appendicitis is when the appendix becomes blocked and inflamed
Appendicitis is when the appendix becomes blocked and inflamed. The appendix is a small pouch attached to the large intestine, whose function is not well known.

5
Causes, incidence, and risk factors
Appendicitis is one of the most common causes of emergency abdominal surgery in the United States. Appendicitis usually occurs when the appendix becomes blocked by feces, a foreign object, or rarely, a tumor .

7
Symptom of Appendicitis
Appendicitis is the most common surgical emergency seen in hospitals. Six of every hundred persons will get it at some point in their life.

8
It's use is unknown but sometimes it gets blocked by stool passing by
It's use is unknown but sometimes it gets blocked by stool passing by. Once this happens bacteria in the stool start to multiply and cause an infection of the appendix. It's like having a river of stool passing by. If it stops it gets stagnant just like a real pool of water allowing bacteria to grow - which is why stagnant water starts to smell bad.

9
The symptoms of Appendicitis
Abdominal pain:-Pain may begin in the upper-middle abdomen (epigastric), then develop to sharp localized pain Pain may shift from the epigastric area to become most intense in the lower right side of the abdomen ("typical" case), tenderness of this area is common Pain initially may be vague, but becomes increasingly more severe
, then develop to sharp localized pain. Pain may shift from the epigastric area to become most intense in the lower right side of the abdomen ( typical case), tenderness of this area is common. Pain initially may be vague, but becomes increasingly more severe.")
10
Point tenderness, especially over the right lower quadrant of the abdomen
Nausea and vomiting Fever usually occurs within several hours Abdominal pain may be worse when walking or coughing. The patient may prefer to lie still; sudden jarring motions or bumping can cause pain.

11
Later symptoms: Fever Loss of appetite Nausea Vomiting Constipation Rectal tenderness Chills and shaking

12
Additional symptoms that may be associated with this disease include bloody urine (microscopic hematuria).
.")
13
Signs and tests With appendicitis, pain increases when the abdomen is gently pressed and then the pressure is suddenly released. Touching the abdomen may cause a spasm of the abdominal muscles if peritonitis is present. Rectal examination may also cause pain, localized on the right side.

14
The health care provider may perform other tests, including having the patient lie on his or her back with the following: The right leg is extended straight up. The knee and hip are flexed, and then the leg is rotated inward and outward. The lower left portion of the abdomen is palpated.

15
Each of these actions will cause pain in the lower right quadrant of the abdomen of a person with appendicitis. Appendicitis may be strongly suspected based on the following tests: CBC, often shows an increased white blood cell count Abdominal sonography Abdominal CT scan

17
Appendicitis is diagnosed from a history of the above symptoms and by pressing with his/her hand on the tummy. If there is pain over the right lower abdomen, especially if worse on jerking the area, appendicitis is strongly suspected - except in females where ovaries and other structures can also lead to pain in this area.

18
The surgeon may confirm the diagnosis during an exploratory laparotomy
The surgeon may confirm the diagnosis during an exploratory laparotomy. The operation may be done as an open procedure or through a laparoscopic approach that uses a small camera and requires a smaller incision. It is important to realize that not all surgical explorations for appendicitis reveal an abnormal appendix.

19
Approximately 10-15% of operations for suspected appendicitis reveal either no obvious abnormality, or a disease process other than appendicitis. This relatively high rate of "negative appendectomies" is tolerated because the consequences of not diagnosing appendicitis in patients with abdominal pain can be severe and sometimes life-threatening.

20
If an operation for suspected appendicitis reveals a normal appendix, the surgeon will probably remove the appendix anyway, and then explore the rest of the abdomen for other possible causes of pain. In some cases, this may require extension of the surgical incision.

22
inflammatory bowel diseases
These diseases each exhibit very different symptoms that make them appear to be completely unrelated. However, they all have one commonality. They are all autoimmune disorders in which the body's immune system has been accidentally triggered to attack a specific protein tissue of your own body.

23
The original cause is most likely Leaky Gut Syndrome
The original cause is most likely Leaky Gut Syndrome. Therefore, autoimmune diseases such as arthritis, multiple sclerosis and lupus have a very close connection with inflammatory bowel diseases. Many people exhibit several of these diseases for this reason.

25
Doctors will typically prescribe drugs to treat the multitude of possible symptoms which leads people to think the diet should be different for each. Doctors also prescribe drugs to suppress the immune system in an attempt to stop the attack. Most of these drugs have very harmful side effects.

26
This diet program addresses the root cause by eliminating those foods that trigger the immune system to attack the body. Eating one bite of a "Forbidden Food" as listed below can trigger an autoimmune flare that will last for weeks. Therefore, strictly compliance with this diet program is required.

27
Most people suffering from chronic intestinal problems have been found to be addicted to the very foods that made them sick and continue to prevent their recovery. These people typically refuse to change their nutritional philosophy.

28
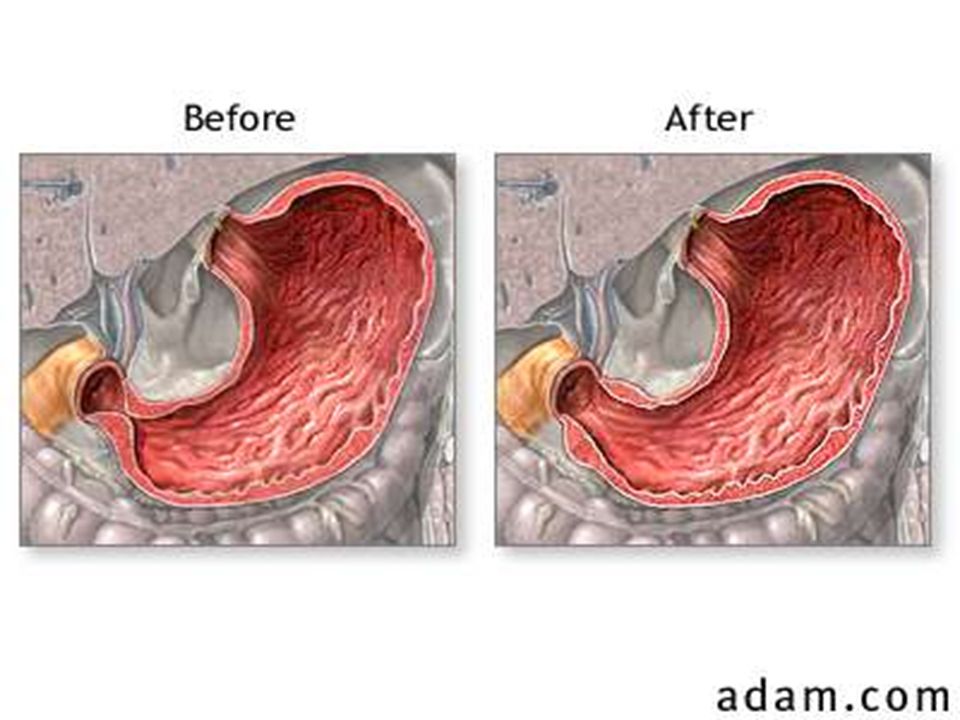
Pyloric stenosis The stomach connects the esophagus to the small intestines The pylorus of the stomach is a small, narrow muscular sphincter through which food passes into the duodenum after it has been partially digested in the stomach.

30
Pyloric stenosis is a congenital defect in which the opening of the pylorus is too narrow. Food is thus unable to pass into the duodenum. Children with pyloric stenosis usually manifest forceful, "projectile" vomiting within the first 1-2 weeks of life.

32
After general anesthesia is administered and the patient is in deep sleep and pain free, the abdomen is cleaned and draped. A small incision is made in the abdomen.

34
The surgeon makes a cut into the pyloric muscle (stomach outlet) down to the mucosa, the inner layer of the stomach, thus releasing the restriction. No tissue is removed and the stomach lining is not opened. The pyloric muscle returns to normal size with time.

36
Children usually recover quickly
Children usually recover quickly. There are no long-term disadvantages to surgery. One to two days of hospitalization may be all that is required. Feedings by mouth are usually delayed for 12 hours after the operation. The stomach requires this short time to regain its ability to contract and to empty.

37
Most infants can advance from clear liquids to normal amounts of formula or breast feedings within 36 hours after the operation. Vomiting of one or two feedings in the first 24 to 48 hours after the operation is not uncommon.

38
Paper tapes will cover a small incision located on the child’s right upper abdomen. A firm ridge may appear at the incision site, which is no cause for concern. Avoid bathing for at least 5 days after the operation. Sponge bathing is permitted the day of discharge. Carefully pat dry the incision tapes after the sponge bath.

40
Celiac disease is a life-long autoimmune disorder of the intestinal tract, which may have its onset in childhood or adulthood. (Celiac disease occurs with greater incidence in persons with other autoimmune disorders.) The disorder is characterized by sensitivity to the predominant wheat protein, gluten (or more specifically, the gliadin portion of the molecule).
 The disorder is characterized by sensitivity to the predominant wheat protein, gluten (or more specifically, the gliadin portion of the molecule).")
41
The disease varies in severity with classic symptoms of malabsorption noted in some persons while others remain completely asymptomatic.

42
The disease has also been known as celiac sprue, nontropical sprue and gluten sensitive enteropathy. It is a genetic condition in which the immune system damages the small intestine when gluten enters the digestive system.

43
The body produces immune cells, which damage the villi
The body produces immune cells, which damage the villi. The villi in a healthy intestine have the appearance of a deep pile carpet. All these villi give the small intestine enormous absorptive surface.

44
Gluten Gliadin, a protein portion of gluten, is the specific offender. Gluten is found in wheat, oats, rye. A gluten-free diet is not simply avoidance of bread and pasta. Starch, flour or additives from the toxic grains are added to many prepared foods and some medications.

45
Corn and rice and their byproducts contain no toxic gluten and are considered safe.

46
Celiac disease Celiac disease is an absorption problem found in the small intestinal tract. Celiac is caused by an excessive amount of mucous secreted by the cellular walls of the tract. This mucous is produced in abundance to protect the already deformed and damaged cellular surface due to bacterial attacks and or parasite attacks

48
This typically occurs in the lower portion of the small intestinal tract because this area is the farthest away from the hydrochloric acid of the stomach. The organism either travel from the large colon into the small intestinal tract which is only achievable if the large intestinal tract is extremely dirty and constipated,

49
or through ingesting food that contained the germ
or through ingesting food that contained the germ. Low levels of stomach acid may allow these microbes to survived the secretion of hydrochloric acid. An absorption problem develops when the mucous of the tract becomes too deep to allow nutrients to be absorbed.

50
This causes malnutrition in the body and weakens the immune system leaving the individual susceptible to many viruses. The whole body becomes weakened as essential vitamins and mineral are not being absorbed.

51
Nutrients: The best nutrient for protecting the lower intestines is vitamin B12 in the methylcobalmin form. This type of B12 does not require any breakdown by the liver and is ready for absorption into the blood system via the mouth, stomach and duodenum. From here the B12 will make its way to the tissues that require the vitamin and the individual get healing from the inside out.

52
Suggestion: Diet free of sugar, starches, milk and gluten products such as wheat and rye.
Exclude refined products e.g. sugars, flour, table salt as it contains up to 70% sugar! Sea salt from a health food store is a better choice as it contains many minerals.

54
Complications of CD The disease usually is worse in the first portions of the small intestines. When only the top of the small intestine is smooth (flattened villi), gastrointestinal symptoms may not be present. There may or may not be discomfort, bloating or gas, possibly no diarrhea and/or constipation.
, gastrointestinal symptoms may not be present. There may or may not be discomfort, bloating or gas, possibly no diarrhea and/or constipation.")
55
The presentation of CD is very serious (in spite of no intestinal symptoms) because many nutrients are absorbed in this area of the digestive system.
 because many nutrients are absorbed in this area of the digestive system.")
56
Vitamin B1 and B12 (numbness in extremities), Iron (anemia), Folic Acid (birth defects), Calcium and Vitamin D (bones and muscles), Vitamin E (nerves), Vitamin A (eyes) and Vitamin K (blood clotting) may be malabsorbed. That is, the nutrients from food and supplements are not absorbed properly.

57
When a larger portion of the small intestine is damaged, gas, bloating and discomfort can be present in addition to the malabsorption of nutrients. Until recently diagnosis was made when much of the intestine had been damaged, diarrhea and wasting appear in addition to malabsorption of nutrients.

58
Additional explanation of the complications of malabsorption include (besides weight loss, vitamin and mineral deficiencies) coagulopathy, osteopenia, bone fractures, lymphocytic gastritis and lymphocytic colitis/intestinal strictures and ulcerations may occur. Other complications include refractory and collagenous sprue as well as malignancy.

59
There is a three to four-fold increased incidence of all malignancies among undiagnosed celiac, half of which occur in the intestinal tract. Of those, there is a particularly high incidence of enterocyte associated T cell lymphoma of the small intestine (EATL).
.")
60
This is very difficult to diagnose and warning symptoms may include unexplained or worsening diarrhea, weight loss and abdominal pain. There is also a much greater incidence of adenocarcinoma of the small intestine. The risk of malignancy returns to that of the general population after five years of maintaining a gluten-free lifestyle.

61
Untreated celiac disease will also negatively affect pregnancy outcome with relative incidences of spontaneous abortion and low birth weight being nearly nine and six times higher respectively. These improve markedly in treated celiac patients with unexplained neurological dysfunction.

62
Side Effects Bone disease Short stature in children
Joint and bone aches Muscle weakness and cramps Anemia Lactose intolerance Chronic fatigue Edema (swelling)
")
63
Hyperactivity Personality change Attention deficit Neurological disorders Ataxia (stumbling gait) Spinal cord lesions Eye problems Dental defects
 Spinal cord lesions. Eye problems Dental defects.")
64
Diagnosis Diagnosis of celiac disease should be considered when symptoms or laboratory findings indicate celiac disease could be an explanation of the person's health condition. A reliable assessment of gluten sensitivity is a celiac disease evaluation panel (of blood tests) which includes: IgG and IgA Gliadin Antibodies (AGA)
 which includes: IgG and IgA Gliadin Antibodies (AGA)")
65
IgA Endomysial Antibodies (EmA)
IgA Reticulin Antibodies (ARA) These studies, whether positive or negative, are only suggestions and reasonably predictive of the possibility of celiac disease. Confirmation or exclusion of the disease requires a biopsy of the small intestine.
 These studies, whether positive or negative, are only suggestions and reasonably predictive of the possibility of celiac disease. Confirmation or exclusion of the disease requires a biopsy of the small intestine.")
66
The biopsy is usually performed through an endoscope - commonly done under sedation - in which a flexible tube is passes through the mouth into the small intestine where several biopsies are obtained.

67
It is still advisable to obtain annual CBC, biochemical panel, iron levels, B12, folic acid and vitamin D-250H. A one-year post-treatment biopsy is important in establishing a new baseline, as all patients do not heal completely in spite of strict adherence to the diet. Bone densitometry at the time of diagnosis and periodically thereafter is important - particularly in female patients.

68
Celiac antibodies may be helpful in monitoring some patients, particularly those in whom noncompliance is suspected. It should be stated also that first-degree relatives of celiac should also be screened since celiac disease is a genetic disease.

69
Treatment A life-long adherence to a gluten-free diet.
This is a very under diagnosed disease because the symptoms are so varied. Until recently, only persons were diagnosed with celiac disease who presented with the most severe gastrointestinal symptoms such as diarrhea and weight loss. Currently, celiac disease experts advise that all the listed SIDE EFFECTS, ASSOCIATED AUTOIMMUNE DISORDERS and the FAMILY HISTORY should be considered diagnosis.

Similar presentations












 the immune system reacts abnormally.>")














 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")



