Download presentation
Presentation is loading. Please wait.

1
Medical management of ulcerative colitis
Y.Bafandeh;MD. Professor of Gastroenterology and Hepatology Residents-1391/10/16

2
What is IBD? Chronic Inflammation of the bowel Idiopathic
Relapsing course

3
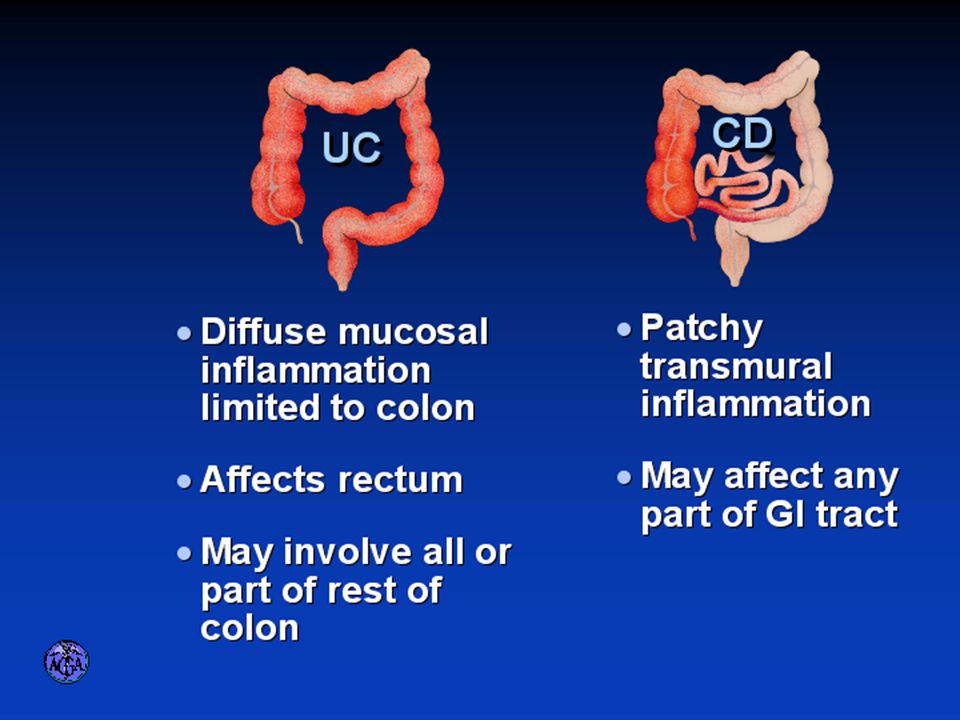
IBD Spectrum Ulcerative colitis Crohn’s Disease Indeterminant colitis

5
Epidemiology

6
Incidence of ulcerative colitis Representation of the relatively constant reported rates of ulcerative colitis

7
The incidence of Crohn's disease rose progressively in various parts of the world from 1955 to 1985.

8
IBD Facts Approx 1,000,000 Americans have IBD
men and women affected equally first peak occurs between the ages of a later peak occurs in the 7th decade

9
Histology

10
Normal Intestine Vs. IBD
Environmental triggers (infection, bacterial products) Failure to down- regulate Chronic uncontrolled inflammation = IBD Moderately inflamed Down-regulate Normal gut controlled inflammation Normal gut controlled inflammation
 Failure to down- regulate. Chronic uncontrolled. inflammation = IBD. Moderately. inflamed. Down-regulate. Normal gut. controlled inflammation. Normal gut. controlled inflammation.")
12
Diet The data suggest that a "Western" style diet (processed, fried and sugary foods) is associated with an increased risk of developing CD, and maybe UC. Food antigens are thought to be a factor in the pathogenesis of IBD. This is the rationale by which patients are given nothing by mouth as a component of their treatment for a flare of IBD. It remains to be seen if dietary factors are a cause of an immunologic response resulting in the development of IBD. However, a number of studies have implicated cow's milk, refined sugar, decreased vegetable intake, and high fat intake as dietary risk factors for the development IBD.
 is associated with an increased risk of developing CD, and maybe UC. Food antigens are thought to be a factor in the pathogenesis of IBD. This is the rationale by which patients are given nothing by mouth as a component of their treatment for a flare of IBD. It remains to be seen if dietary factors are a cause of an immunologic response resulting in the development of IBD. However, a number of studies have implicated cow s milk, refined sugar, decreased vegetable intake, and high fat intake as dietary risk factors for the development IBD.")
13
Oral contraceptives Some case-control studies have not found an association between the use of oral contraceptives and the development of either ulcerative colitis or Crohn's disease .Furthermore, oral contraceptives do not appear to influence the course of patients with established Crohn's disease . If oral contraception predisposes to the development of IBD, it may be doing so through thrombotic effects on the microvasculature. Given the uncertainty, it is reasonable to continue oral contraception in patients with IBD who are doing well. However, in those who remain symptomatic despite conventional drug therapy, cessation of oral contraception should be considered.

14
NSAIDs A number of reports suggest that NSAIDs increase the risk for the development of IBD and may exacerbate underlying IBD ,although some patients with IBD appear to be able to tolerate them, particularly when given in low doses . Experience with the COX-2 selective inhibitors in patients with IBD is limited. In theory, because COX-2 activity promotes epithelial proliferation and wound healing, COX-2 inhibition may have a deleterious effect in patients with IBD .However, the available data suggest that most patients can tolerate at least short-term treatment without exacerbation of disease.

15
Psychosocial factors Analyses conclude that there is no consistent type of psychopathology among patients with either Crohn's disease or ulcerative colitis . Stress does not appear to be related to the onset of IBD, but even if not causally related, it may have a role in the exacerbation of symptoms ,possibly via activation of the enteric nervous system and the elaboration of proinflammatory cytokines.

16
Evidence of Genetic Influence
Prevalence varies among different populations (Both ulcerative colitis and Crohn's disease are more common in Jews than non-Jews ) Risk in increased among first degree relatives (10 to 25 percent of affected patients have a first degree relative with either Crohn's disease or ulcerative colitis .Furthermore, there tends to be a concordance for the same disease category within families, especially with Crohn's disease. Among families with Crohn's disease, there may also be a concordance for disease location and the severity of the clinical course ) Greater concordance among monozygotic than diazygotic twins Observations indicate different genetic susceptibilities for the two disorders. The first confirmed IBD gene (IBD1) confers an increased risk of Crohn's disease. IBD1 encodes a product (NOD2 also referred to as CARD 15).
 Risk in increased among first degree relatives (10 to 25 percent of affected patients have a first degree relative with either Crohn s disease or ulcerative colitis .Furthermore, there tends to be a concordance for the same disease category within families, especially with Crohn s disease. Among families with Crohn s disease, there may also be a concordance for disease location and the severity of the clinical course ) Greater concordance among monozygotic than diazygotic twins. Observations indicate different genetic susceptibilities for the two disorders. The first confirmed IBD gene (IBD1) confers an increased risk of Crohn s disease. IBD1 encodes a product (NOD2 also referred to as CARD 15).")
17
Proportion of Patients with Family History of IBD by Age of Diagnosis
* % Patients with Positive Family History of IBD * *p<0.005 Polito JM et al. Gastro.1996;111:580

18
Diagnosis

19
Diagnosis Clinical history Physical examination Laboratory tests
Endoscopic findings Radiographic findings Histology

20
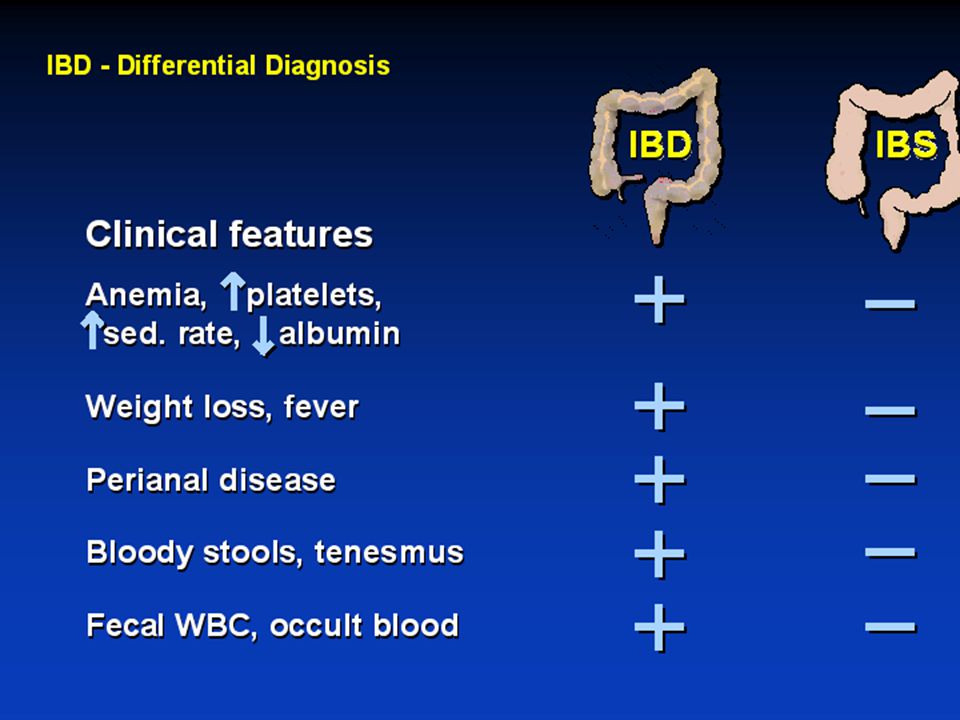
Differential Diagnosis
Lymphoma Infectious etiologies Appendicitis Diverticulitis Carcinoma Celiac Disease Ischemic colitis Irritable Bowel Syndrome

24
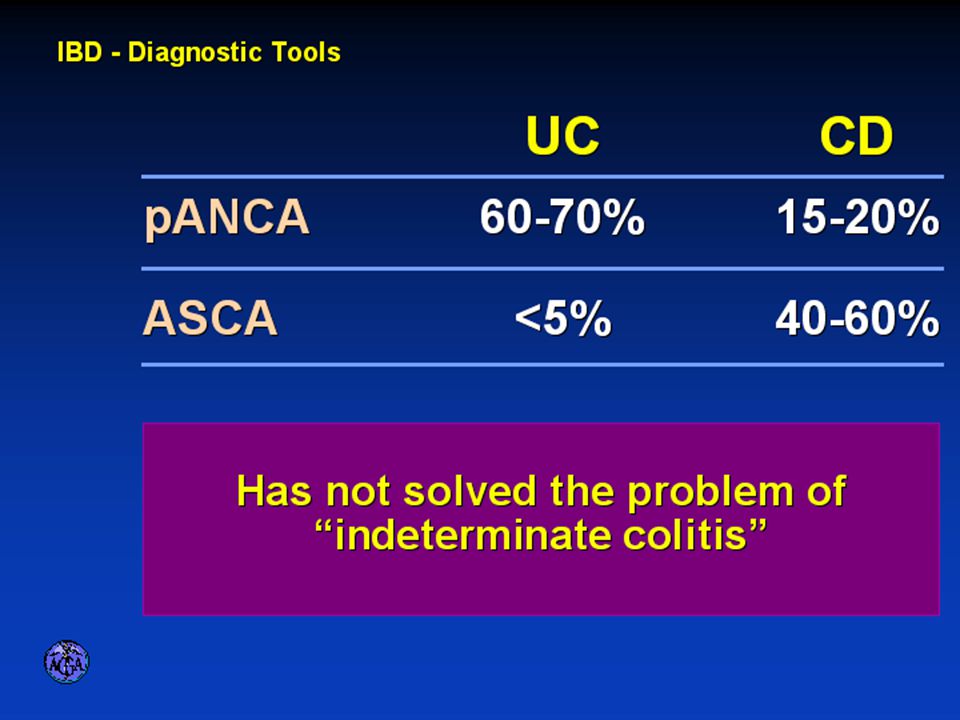
Antibody tests Antineutrophil cytoplasmic antibodies (pANCA) and anti-Saccharomyces cerevisiae antibodies (ASCA) – pANCA and ASCA have been proposed as a means for diagnosing IBD and distinguishing CD from ulcerative colitis. One study included 582 adult patients with established diagnoses (407 with CD, 147 with ulcerative colitis, and 28 with indeterminate colitis) . The sensitivity of the antibody tests alone or in combination was in the range of 40 to 60 percent, and the specificity was greater than 90 percent for distinguishing patients with IBD from controls. Specificity was slightly less for distinguishing ulcerative colitis from CD .
 and anti-Saccharomyces cerevisiae antibodies (ASCA) – pANCA and ASCA have been proposed as a means for diagnosing IBD and distinguishing CD from ulcerative colitis. One study included 582 adult patients with established diagnoses (407 with CD, 147 with ulcerative colitis, and 28 with indeterminate colitis) . The sensitivity of the antibody tests alone or in combination was in the range of 40 to 60 percent, and the specificity was greater than 90 percent for distinguishing patients with IBD from controls. Specificity was slightly less for distinguishing ulcerative colitis from CD .")
25
Crohn’s Disease

26
History In 1932, Drs. Crohn, Oppenheimer and Ginzburg at Mount Sinai Medical Center described a subacute inflammatory process affecting the distal ileum “terminal ileitis” “granulomatous ileitis” In 1952, Dr. Wells reported colonic involvement

27
What is Crohn’s Disease?
Crohn’s disease (CD) is an inflammatory bowel disorder that may affect any part of the gastro-intestinal (GI) tract The inflammation penetrates the lining of the GI tract and often causes ulcers Esophagus Small Intestine Stomach Large Intestine (Colon) Rectum Appendix
 is an inflammatory bowel disorder that may affect any part of the gastro-intestinal (GI) tract. The inflammation penetrates the lining of the GI tract and often causes ulcers. Esophagus. Small. Intestine. Stomach. Large. Intestine. (Colon) Rectum. Appendix.")
28
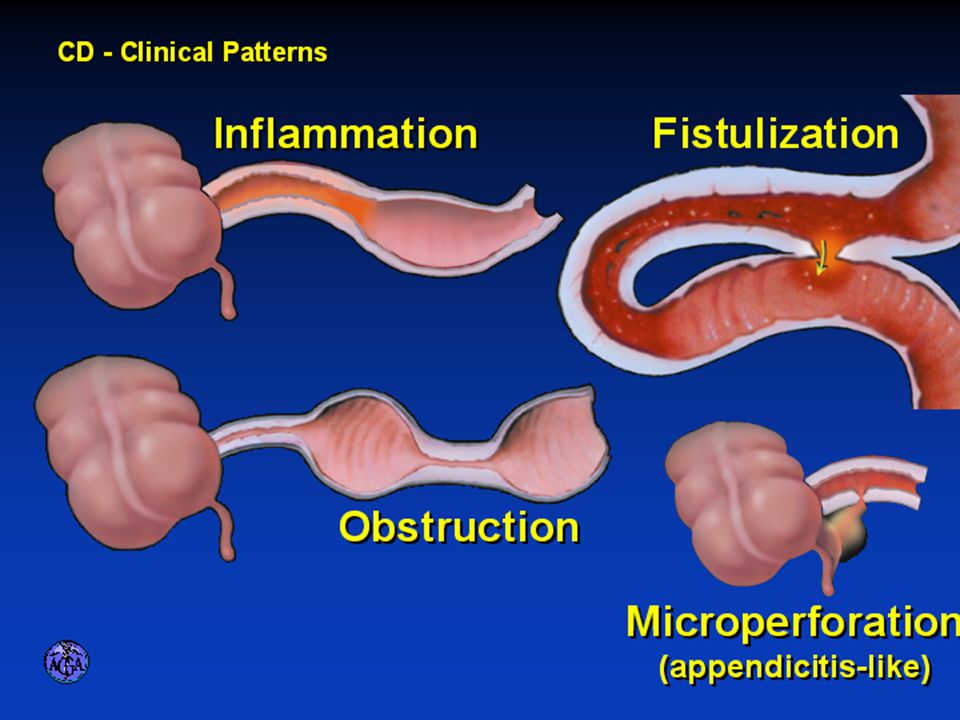
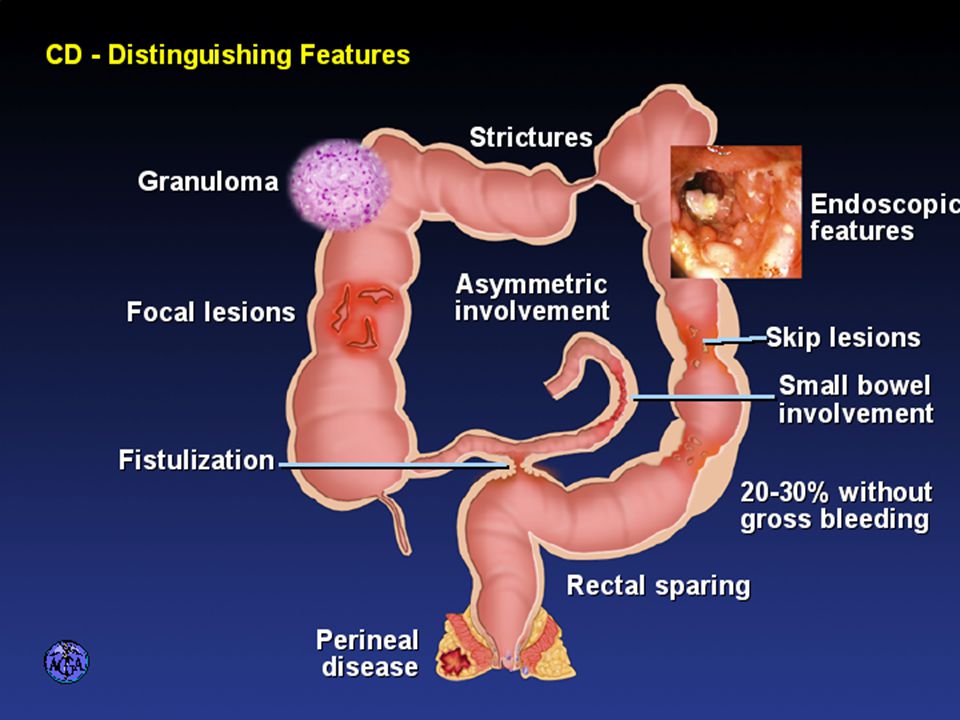
Crohn’s Disease Crohn's disease may involve the entire gastrointestinal tract from mouth to perianal area: Approximately 80 percent of patients have small bowel involvement, usually in the distal ileum, with one-third of patients having exclusively ileitis. Approximately 50 percent of patients have ileocolitis, which refers to involvement of both the ileum and colon. Approximately 20 percent have disease limited to the colon. Although this pattern is similar to that in ulcerative colitis, roughly one-half of such patients have sparing of the rectum, which is rare in ulcerative colitis. A small percentage of patients have predominant involvement of the mouth or gastroduodenal area, while fewer patients have involvement of the esophagus and proximal small bowel. Approximately one-third of patients have perianal disease.

29
CLINICAL MANIFESTATIONS - CD
Patients can have symptoms for many years prior to diagnosis . Fatigue, prolonged diarrhea with abdominal pain, weight loss, and fever, with or without gross bleeding, are the hallmarks of CD .

31
Crohn’s Disease: Fistula

32
Fistulas Fistulas are tracts or communications that connect two epithelial-lined organs. Common sites for fistulas connect the intestine to bladder (enterovesical), to skin (enterocutaneous), to bowel (enteroenteric), and to the vagina (enterovaginal). In a population-based study of patients with CD, the cumulative risk of developing a fistula was 33 and 50 percent after 10 and 20 years, respectively . Up to 45 percent of patients develop a fistula before diagnosis of CD. Enterocutaneous fistulas can cause bowel contents to drain to the surface of the skin
, to skin (enterocutaneous), to bowel (enteroenteric), and to the vagina (enterovaginal). In a population-based study of patients with CD, the cumulative risk of developing a fistula was 33 and 50 percent after 10 and 20 years, respectively . Up to 45 percent of patients develop a fistula before diagnosis of CD. Enterocutaneous fistulas can cause bowel contents to drain to the surface of the skin.")
33
Phlegmon/abscess All sinus tracts do not lead to fistulas. Sinus tracts may present as a phlegmon, a walled off inflammatory mass without bacterial infection that may be palpable on physical examination. Ileal involvement is suggested by a mass in the right lower quadrant. Some sinus tracts lead to abscess formation and an acute presentation of localized peritonitis with fever, abdominal pain and tenderness. Diffuse peritonitis due to abscess perforation is a rare but recognized complication of CD.

34
Malabsorption Steatorrhea (disease or resection of more than 100 cm of the terminal ileum, leading to depletion of the bile salt pool and fat malabsorption )can lead to severe malnutrition, clotting abnormalities, osteomalacia, and hypocalcemia, which may cause tetany.
can lead to severe malnutrition, clotting abnormalities, osteomalacia, and hypocalcemia, which may cause tetany.")
35
Extraintestinal manifestations
CD and ulcerative colitis share a number of extraintestinal manifestations generally related to inflammatory disease activity and includes: Musculoskeletal , Skin and mouth , Hepatobiliary , Ocular , Metabolic and Less common as Blood and vascular , Renal and genitourinary tract , Neurological , Airway and parenchymal lung disease , Cardiac , Pancreas , Autoimmune .

36
Erythema Nodosum

37
Pyoderma Gangrenosum

38
DIAGNOSIS - CD The diagnosis of CD is usually established with endoscopic findings or imaging studies in a patient with a compatible clinical history. Physical examination may be normal or show nonspecific signs (pallor, weight loss) suggestive of CD. More specific findings include perianal skin tags, sinus tracts, and abdominal tenderness. Presenting symptoms frequently determine the order of subsequent testing. Colonoscopy is the most appropriate initial test for patients presenting with predominant diarrhea, while imaging studies may be more appropriate for those presenting with abdominal pain.
 suggestive of CD. More specific findings include perianal skin tags, sinus tracts, and abdominal tenderness. Presenting symptoms frequently determine the order of subsequent testing. Colonoscopy is the most appropriate initial test for patients presenting with predominant diarrhea, while imaging studies may be more appropriate for those presenting with abdominal pain.")
39
Laboratory studies - CD
Routine laboratory tests may be normal or they may reveal anemia, iron deficiency, elevated white blood cell count, B12 deficiency, and/or elevated erythrocyte sedimentation rate or CRP. If diarrhea is present, a stool specimen should be sent for culture and examination for ova and parasites.

40
Imaging studies - CD Imaging studies are most useful to evaluate the upper gastrointestinal tract and allow documentation of the length and location of strictures in areas not accessible by colonoscopy. Imaging has traditionally involved barium studies, such as barium enema or upper gastrointestinal series with small bowel follow through (SBFT), though the use of computed tomography (CT) and magnetic resonance imaging (MRI) is becoming more common.
, though the use of computed tomography (CT) and magnetic resonance imaging (MRI) is becoming more common.")
41
Aphthoid ulcers in Crohn's disease Colonic disease

42
T2-weighted axial magnetic resonance imaging (MRI) study showing perianal fistulas (arrows) in a patient with Crohn's disease.
 study showing perianal fistulas (arrows) in a patient with Crohn s disease.")
43
Small bowel disease Radiologic imaging is generally needed to evaluate patients with probable small bowel disease. Several imaging modalities are available, including conventional upper gastrointestinal series with SBFT, CT and CT enterography, enteroclysis, and MRI and MR enterography. While CT enterography and MR enterography are being done more frequently, in general, the initial study remains the conventional upper gastrointestinal series with SBFT.

44
Small bowel disease Upper gastrointestinal series with SBFT involves ingestion of a barium solution with subsequent radiologic imaging of the small intestine. Typical features of small bowel CD include narrowing of the lumen with nodularity and ulceration, a "string" sign when luminal narrowing becomes more advanced or with severe spasm, a cobblestone appearance, fistulas and abscess formation, and separation of bowel loops, a manifestation of transmural inflammation with bowel wall thickening.

45
Crohn's disease of the upper gastrointestinal tract

46
Fibrostenotic Crohn’s Disease

47
Single axial CT scan of the lower abdomen demonstrates an abscess (arrowheads) extending from the markedly thickened and inflamed terminal ileum (arrow). The presence of contrast material within the abscess confirms a communication with the adjacent ileum.

48
Endoscopic findings in Crohn's disease: Endoscopic findings in Crohn's disease include: aphthous ulcers, which are the earliest lesions seen in Crohn's disease (panel A); large ulcers interspersed with normal mucosa, which are typical for the segmental distribution of Crohn's disease (panel B); a cobblestone appearance that is characterized by nodular thickening, with linear or serpiginous ulcers (panel C); and strictures due to fibrosis (panel D).
; large ulcers interspersed with normal mucosa, which are typical for the segmental distribution of Crohn s disease (panel B); a cobblestone appearance that is characterized by nodular thickening, with linear or serpiginous ulcers (panel C); and strictures due to fibrosis (panel D).")
50
Crohn’s Disease Histology
The major findings on intestinal biopsy are focal ulcerations, and acute and chronic inflammation. These findings are usually confirmatory rather than diagnostic. The focality of the inflammation differs from the diffuse pattern seen typically in ulcerative colitis. Granulomas may be noted in up to 30 percent of patients with CD and are diagnostic of the disorder if appropriate infections are excluded .Thus, demonstration of a granuloma is not required for establishing the diagnosis, nor does its presence confirm the diagnosis, since granulomas may be seen with other disorders including Yersinia spp., Behçet's disease, tuberculosis, and lymphoma.

51
Crohn’s Disease Histology

53
Crohn’s Disease Histology

55
CANCER RISK The AGA concluded that the risk of colorectal cancer associated with ulcerative colitis and Crohn's colitis is similar for comparable extent, duration, and age of onset of inflammatory disease. As a result, the surveillance strategy discussed for UC also applies for Crohn's colitis.

56
Ulcerative Colitis

57
History 1859, Samuel Wilks described “simple idiopathic colitis” 1909
Hawkins described the natural history of UC Hurst describe the sigmoidoscopic appearance

58
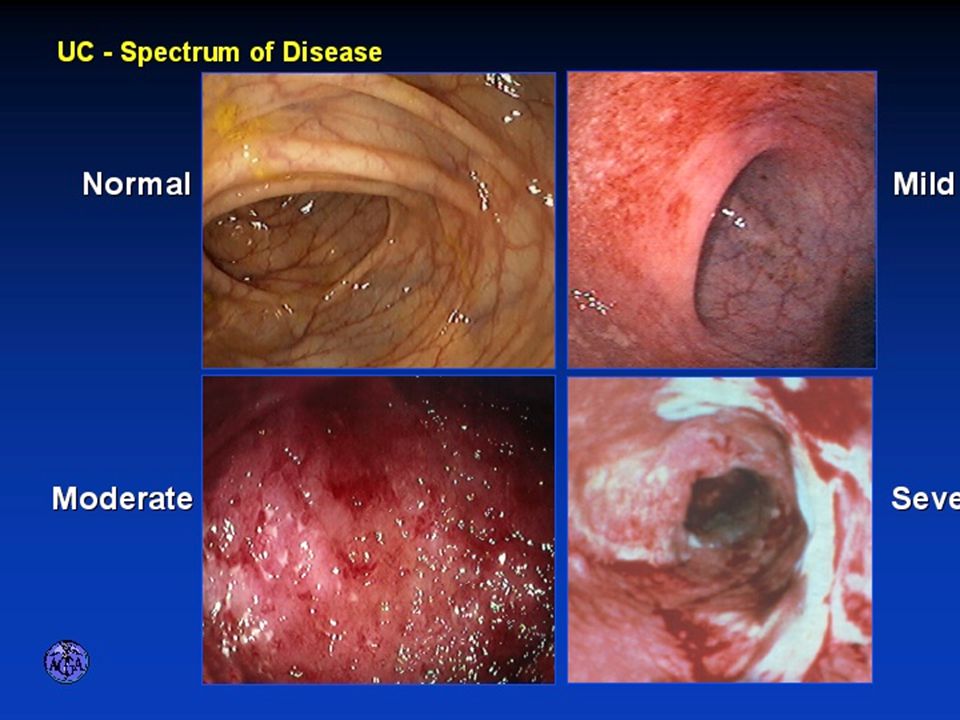
SIGNS AND SYMPTOMS -UC Patients with ulcerative colitis can have a variable presentation. For therapeutic and prognostic purposes, it has been useful to classify these presentations as mild, moderate, or severe. The severity of the symptomatology often correlates with the anatomic extent of disease, another parameter that will guide therapy.

59
Mild disease Patients whose disease is confined to the rectum (proctitis) or rectosigmoid (proctosigmoiditis or distal colitis), often present insidiously with intermittent rectal bleeding associated with the passage of mucus, and the development of mild diarrhea with fewer than four small loose stools per day. Mild crampy pain, tenesmus, and periods of constipation are also common, but severe abdominal pain, profuse bleeding, fever, and weight loss are not part of the spectrum of mild disease.
 or rectosigmoid (proctosigmoiditis or distal colitis), often present insidiously with intermittent rectal bleeding associated with the passage of mucus, and the development of mild diarrhea with fewer than four small loose stools per day. Mild crampy pain, tenesmus, and periods of constipation are also common, but severe abdominal pain, profuse bleeding, fever, and weight loss are not part of the spectrum of mild disease.")
60
Moderate disease Moderate disease is usually characterized anatomically by involvement of more than the distal colon, with the inflammatory process extending to at least the splenic flexure (left-sided colitis). The clinical picture is characterized by frequent loose, bloody stools (up to 10 per day), mild anemia not requiring blood transfusions, abdominal pain that is not severe, and low grade fever. Adequate nutrition is usually maintained.
. The clinical picture is characterized by frequent loose, bloody stools (up to 10 per day), mild anemia not requiring blood transfusions, abdominal pain that is not severe, and low grade fever. Adequate nutrition is usually maintained.")
61
Severe disease Patients with a severe or fulminant presentation usually have extensive colonic involvement, often but not always extending to the cecum (pancolitis). These patients typically have frequent loose stools (greater than 10 per day) with severe cramps, fever up to 39.5ºC, and bleeding often necessitating blood transfusion. They may suffer rapid weight loss, leading to a poor nutritional state. In severely ill patients, the inflammatory process may extend beyond the mucosa to involve the muscle layers of the colon. In this setting, colonic motility is impaired, the colon dilates, bowel movements may become less frequent, and a pattern termed toxic megacolon ensues. Extension of the disease process to the serosa may lead to colonic perforation.
. These patients typically have frequent loose stools (greater than 10 per day) with severe cramps, fever up to 39.5ºC, and bleeding often necessitating blood transfusion. They may suffer rapid weight loss, leading to a poor nutritional state. In severely ill patients, the inflammatory process may extend beyond the mucosa to involve the muscle layers of the colon. In this setting, colonic motility is impaired, the colon dilates, bowel movements may become less frequent, and a pattern termed toxic megacolon ensues. Extension of the disease process to the serosa may lead to colonic perforation.")
62
Disease Distribution at Presentation
37% 17% 46% Farmer RG. Dig Dis Sci;38:

63
DIAGNOSIS - UC The diagnosis of ulcerative colitis can usually be established by the characteristic history coupled with a typical endoscopic appearance of the mucosa and confirmatory histology seen on colonic biopsy. CT may also show marked thickening of the bowel wall, but this finding is nonspecific .

64
Flexible sigmoidoscopy -UC
Since treatment is based in part on the extent of disease, it is useful at the initial presentation to document the extent of inflammation by flexible sigmoidoscopy Total colonoscopy is usually not necessary at this time unless there is confusion about the underlying diagnosis. Furthermore, it may induce megacolon or perforation in the severely ill patient with extensive disease.

65
Flexible sigmoidoscopy -UC
The normal colonic mucosa has well demarcated vessels and a shiny pale appearance. The vascular markings are lost due to engorgement of the mucosa, giving it an erythematous appearance. In addition, petechiae, exudates, touch friability, and frank hemorrhage may be present. More severe cases may be associated with macroulcerations, profuse bleeding, and copious exudates . Colonic involvement is continuous in ulcerative colitis, in contrast to the patchy nature of Crohn's disease . Pseudopolyps, as a reaction to prior inflammation and signifying some degree of chronicity, may be present in areas of disease involvement.

67
Ulcerative Colitis Complications
Massive Bleeding Perforation Acute Dilation Pseudopolyps Colonic Cancer Extraintestinal manifestations

68
Local complications Massive hemorrhage occurs in up to 3 percent of patients with ulcerative colitis and may necessitate urgent colectomy . Fulminant colitis is seen in up to 15 percent of patients, up to 20 percent of whom progress to toxic megacolon which carries with it the risk of perforation and death . Perforation with peritonitis has been associated with a 50 percent mortality in ulcerative colitis.

69
Local complications Benign stricture can occur due to repeated episodes of inflammation and, in some cases, to muscle hypertrophy. Stricture is most common in the rectosigmoid area, occurs in about 10 percent of cases with ulcerative colitis, and may cause symptoms of obstruction. Strictures in ulcerative colitis should be considered malignant until proven otherwise by endoscopic evaluation with biopsy. Surgery is indicated for strictures that cause continued symptoms of obstruction or that cannot be fully evaluated to exclude malignancy.

70
Local complications A major concern in the evolution of ulcerative colitis is the potential for the development of colon cancer . The risk of acquiring colon cancer is related to both the duration and extent of the disease. The incidence of colon cancer begins to increase relative to the general population seven to eight years after the onset of disease in those patients with disease beyond the splenic flexure. It is generally agreed that, for the patient at increased risk, the risk goes up about 0.5 percent per year after this time. There also appears to be an increased risk of colon cancer in patients with ulcerative colitis if they also have a family history of colon cancer .

71
Local complications There is emerging evidence that patients with left-sided colitis up to the splenic flexure have almost the same risk of colon cancer as those with disease beyond that point . In contrast, patients with proctitis and distal colitis appear to be at low risk regardless of the duration of disease.

72
Ulcerative Colitis Histology
Colonic biopsy can be used to confirm the diagnosis. It may be particularly helpful if the visual findings are equivocal, since it can detect abnormalities with significant inflammation in such settings. The biopsy characteristically reveals crypt abscesses and chronic changes including branching of crypts, atrophy of glands, and loss of mucin in goblet cells. These findings distinguish ulcerative colitis from other disorders, such as an acute self-limited infectious process.

73
Ulcerative Colitis Histology

74
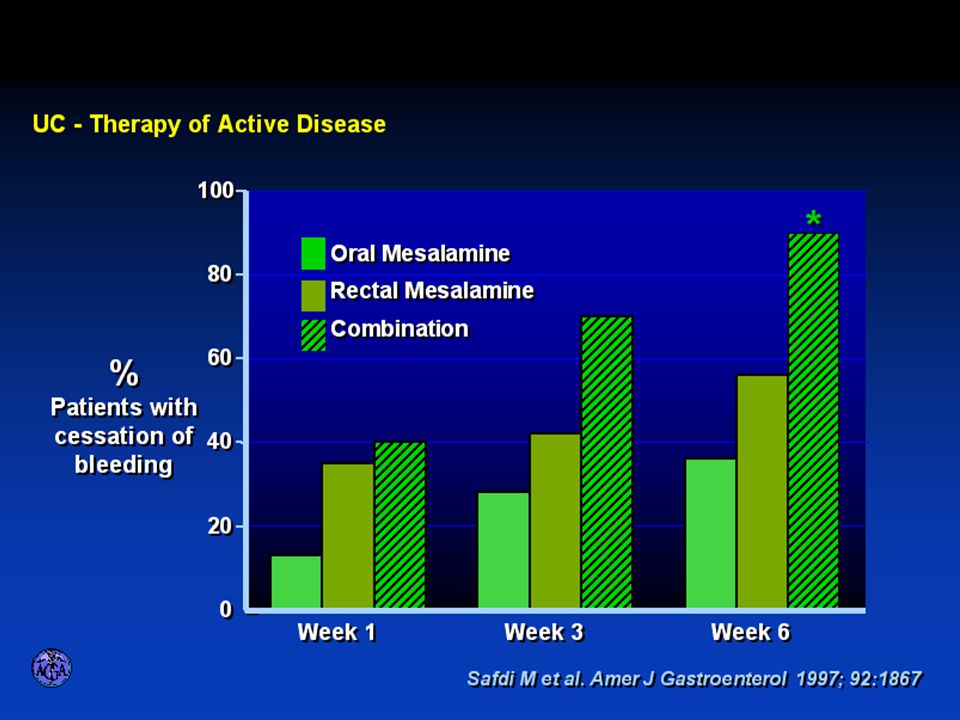
Medical Treatment

75
Goals of Therapy Relieve symptoms Prevent recurrence of symptoms
Prevent or cure complications Control inflammation of the GI tract Improve quality of life Steroid sparing Reduce the need for surgery

76
Disease Activity Number of bowel movements a day
presence of blood in stool abdominal exam (tenderness) Weight loss Extraintestinal manifestation Overall well-being Vitals: fever, tachycardia Labs: anemia,
 Weight loss. Extraintestinal manifestation. Overall well-being. Vitals: fever, tachycardia. Labs: anemia,")
78
Medications for Mild-Moderate Disease
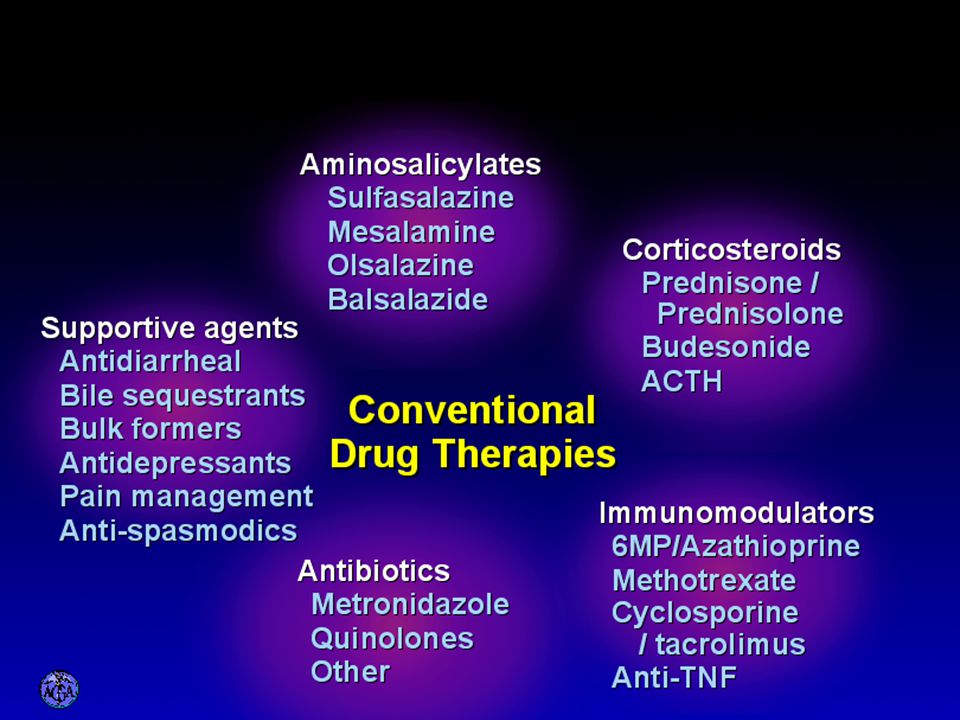
Aminosalicylates Sulfasalazine Mesalamine (Pentasa, Asacol, Colazal, Rowasa enema and Canasa Suppositories) Antibiotics Metronidazole (Flagyl) Quinolones (Cipro)
 Antibiotics. Metronidazole (Flagyl) Quinolones (Cipro)")
79
Medications for Moderate-Severe Disease
Steroids Prednisone Solumedrol Budesonide (Entocort) Immunosuppressives Azathioprine (Imuran) 6-mercaptopurine (Purinethol) Methotrexate Cyclosporin
 Immunosuppressives. Azathioprine (Imuran) 6-mercaptopurine (Purinethol) Methotrexate. Cyclosporin.")
80
Medications for Moderate-Severe Disease
Biologics Infliximab (Remicade)
")
82
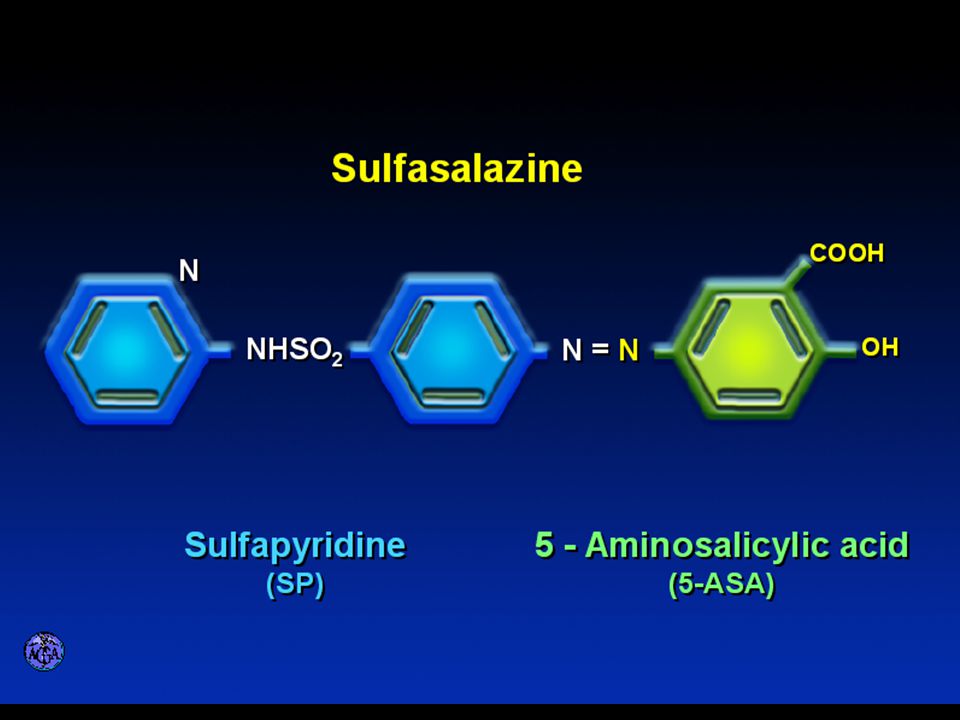
Side Effects of Sulfasalazine
Fever Headache Rash Nausea/vomiting Diarrhea Loss of appetite

83
Mesalamine in microgranules
Oral 5-ASA Release Sites Olsalazine Sulfasalazine Mesalamine in microgranules Pentasa® Mesalamine w/ eudragit-S Asacol® Azo bond COLAZAL™ Stomach Small Intestine Large Intestine

84
Mesalamine Side Effects
Nausea/vomiting Heartburn Diarrhea Headache Allergic Reaction

86
Antibiotic Side Effects
Flagyl metallic taste headache nausea/vomiting dizziness diarrhea peripheral neuropathy Cipro headache rash nausea/vomiting dizziness Achilles tendon rupture

87
Steroid Side Effects GI upset Acne Moon face Fluid Retention Diabetes
HTN Striae Weight gain Cataracts Glaucoma Depression Osteoporosis Infection Growth retardation

88
Outcome of Steroid Therapy for Patients with CD
1-Month Outcomes (n=109) No response 20% Remission 48% Improved 32% 12-Month Outcomes (n=87) Remission 54% Relapse 46% Improved 57% Relapse 43% Summary Outcomes (n=109) Steroid Dependent 36% (n=39) Prolonged Response 44% (n=48) Steroid Resistant 20% (n=22) Munkholm P et al. Gut 1994;35:360
 No response 20% Remission. 48% Improved. 32% 12-Month. Outcomes. (n=87) Remission 54% Relapse 46% Improved 57% Relapse 43% Summary. Outcomes. (n=109) Steroid Dependent. 36% (n=39) Prolonged Response. 44% (n=48) Steroid Resistant. 20% (n=22) Munkholm P et al. Gut 1994;35:360.")
90
Purine Metabolism 6Methyl Mercaptopurine TPMT AZA 6MP 6TGN
HPRT AZA 6MP 6TGN Xanthine oxidase 6Thiouric Acid

91
Immunosuppressant Side Effects
AZA/6MP Bone marrow suppression pancreatitis hepatitis allergic reaction lymphoma infections MTX hepatotoxicity pneumonitis teratogenic alopecia allergic reaction

92
Infliximab

93
Infliximab Side Effects
Reactivation of TB Headache Nausea Upper respiratory tract infection Other serious infections Fatigue Fever

95
Referral to Surgeon Symptoms not relieved by medications
Serious complications abscesses fistula intestinal blockage uncontrolled bleeding

96
Conclusion Crohn’s Disease and Ulcerative Colitis are the two major types of IBD The inflammatory bowel diseases are chronic diseases the are caused by genetic, environmental factors and immunologic abnormalities Medical treatment options should be tailored based of disease type, distribution and pattern

97
Conclusion Medical treatment will usually relieve symptoms but relapse is common and therefore treatment is lifelong

Similar presentations










>")


 Kristina Blaslov Mentor: A. Žmegač Horvat.>")






