Download presentation
Presentation is loading. Please wait.

1
Lower Gastrointestinal Bleeding
Kirk Bernadino, M.D. St. Mary’s / Duluth Clinic Section of Gastroenterology

2
Upper vs. Lower GI Hemorrhage

3
Upper vs. Lower GI Hemorrhage “What Comes Up Might Go Down”
“Hematemesis doesn’t lie”

4
Causes of Lower GI Bleeding
Upper GI Source – 10% Small Bowel Source – 5% Colonic Source – 85%

5
Depth and Bouquet Hematochezia Melena

6
Clots Depth and Bouquet Maroon Bright Red Black STINKY! Hematochezia
Melena Black STINKY!

7
Etiologies of Lower GI Bleeding
Diverticular hemorrhage Cancer / Polyps Angiodysplasia Colitis Anorectal Meckel’s Diverticulum Misc.

8
Etiologies of Lower GI Bleeding
Cancer / Polyps Colon / Rectal Carcinoid Appendiceal Small bowel Metastatic

9
Etiologies of Lower GI Bleeding
Colitis Infectious Ischemic Inflammatory Radiation Diversion

10
Etiologies of Lower GI Bleeding
Anorectal Hemorrhoids Anal Fissure Solitary Rectal Ulcer Dieulafoy’s

11
Etiologies of Lower GI Bleeding
Misc. Postpolypectomy NSAID ulcers Anastomotic

12
Etiologies of Lower GI Bleeding
Diverticular hemorrhage Cancer / Polyps Angiodysplasia Infectious Ischemic Inflammatory Hemorrhoids Anal Fissure Solitary Rectal Ulcer Meckel’s Diverticulum Dieulafoy’s

13
Etiologies of Lower GI Bleeding
Acute Chronic Diverticular hemorrhage Cancer / Polyps Angiodysplasia Infectious Ischemic Inflammatory Hemorrhoids Anal Fissure Solitary Rectal Ulcer Meckel’s Diverticulum Dieulafoy’s

14
Etiologies of Lower GI Bleeding
Acute Chronic Diverticular hemorrhage Cancer / Polyps Angiodysplasia Infectious Ischemic Inflammatory Hemorrhoids Anal Fissure Solitary Rectal Ulcer Meckel’s Diverticulum Dieulafoy’s

15
Etiologies of Lower GI Bleeding
Massive Minor Diverticular hemorrhage Cancer / Polyps Angiodysplasia Infectious Ischemic Inflammatory Hemorrhoids Anal Fissure Solitary Rectal Ulcer Meckel’s Diverticulum Dieulafoy’s

16
Etiologies of Lower GI Bleeding
Massive Minor Diverticular hemorrhage Cancer / Polyps Angiodysplasia Infectious Ischemic Inflammatory Hemorrhoids Anal Fissure Solitary Rectal Ulcer Meckel’s Diverticulum Dieulafoy’s

17
Etiologies of Lower GI Bleeding
Old Young Diverticular hemorrhage Cancer / Polyps Angiodysplasia Infectious Ischemic Inflammatory Hemorrhoids Anal Fissure Solitary Rectal Ulcer Meckel’s Diverticulum Dieulafoy’s

18
Etiologies of Lower GI Bleeding
Old Young Diverticular hemorrhage Cancer / Polyps Angiodysplasia Infectious Ischemic Inflammatory Hemorrhoids Anal Fissure Solitary Rectal Ulcer Meckel’s Diverticulum Dieulafoy’s

19
What is the differential? What is the most likely diagnosis?
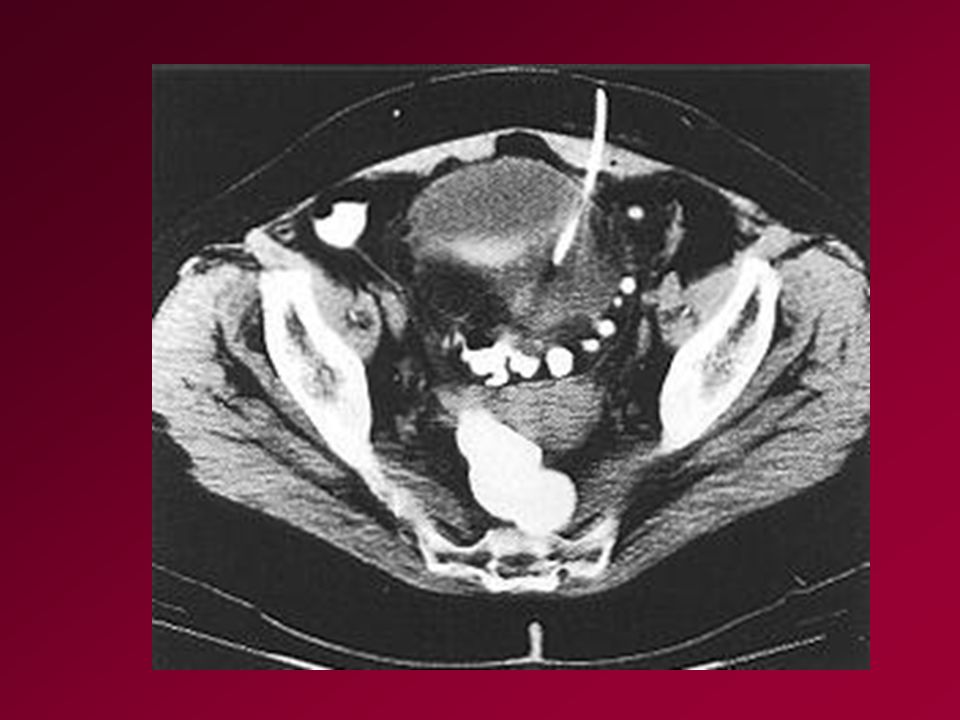
Case 1 A 64 year old man presents with intense LLQ pain and fever. Symptoms have worsened over the last 3 days. A CT of the abdomen and pelvis reveal intense pelvic inflammation with a round structure containing fluid density and air. What is the differential? What is the most likely diagnosis?

21
Diverticulitis & Diverticular hemorrhage

27
Diverticular Disease of the Colon
In the West, affects 5-10% > age 40 and 80% > age 85. Symptoms of diverticulitis occur in about 20% Symptoms: Pain, diarrhea, fever & abdominal tenderness Diverticulitis may rupture or may fistulize to adjacent organs Diverticulitis does not increase risk of hemorrhage Diagnosis is made by CT, not endoscopy or barium enema

29
Treatment of Diverticulitis
Mild without peritoneal signs, tolerating po: oral hydration, liquid diet, oral antibiotics Severe peritonitis, cannot tolerate PO: hospitalize, IV antibiotics, NPO, CT scan Emergent Peritonitis; sepsis; perforation surgical intervention

30
Case 2 A 76 year old man presents to the emergency room having become dizzy after passing a large painless bloody stool. In the ER he again passes a voluminous bright red stool with clots and again feels dizzy. Aside from a BP of 90/56 and a pulse of 110 his physical exam is remarkable only for blood in the rectum. Hgb = 11.2g What is the differential? What is most likely?

32
Think! Small Bowel

38
Diverticular Hemorrhage
50% of acute lower GI bleeding Massive bleeding occurs in 5% of patients with diverticulosis 75% stop spontaneously Bleeding recurs in 30% Risk of rebleeding after a 2nd bleed is > 50%

39
Case 3 An 84 year old woman with renal failure presents to the ER with a 2 day history of copious rectal bleeding confirmed by physical exam. Hgb = 7.4 and she is transfused 2 units packed red cells after complaining of shortness of breath. What would you like to know? What is the differential?

42
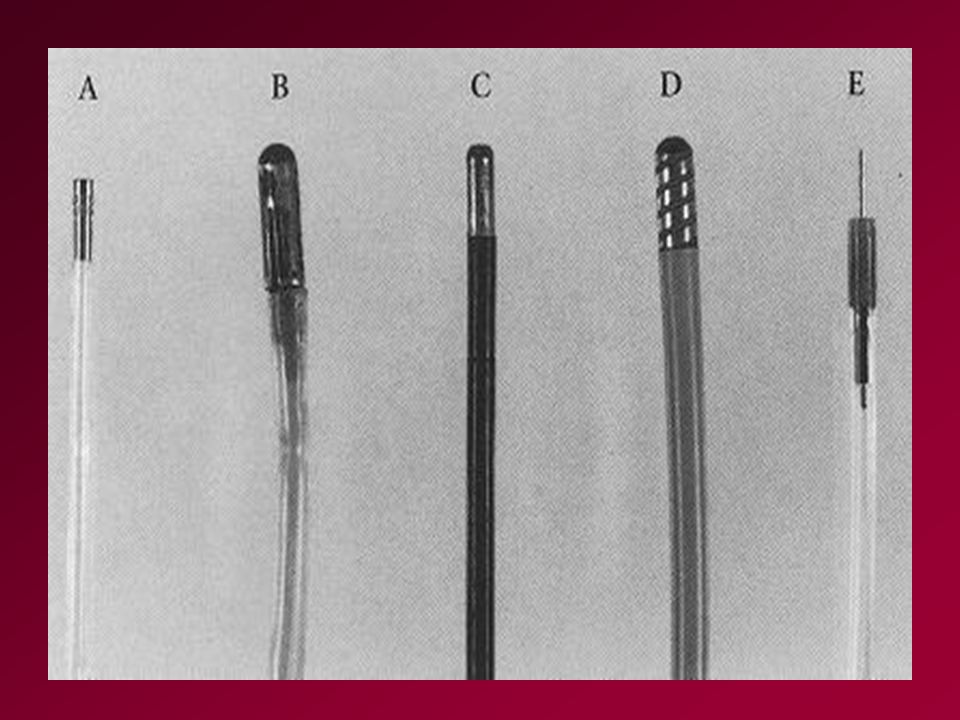
Capsule Endoscopy

45
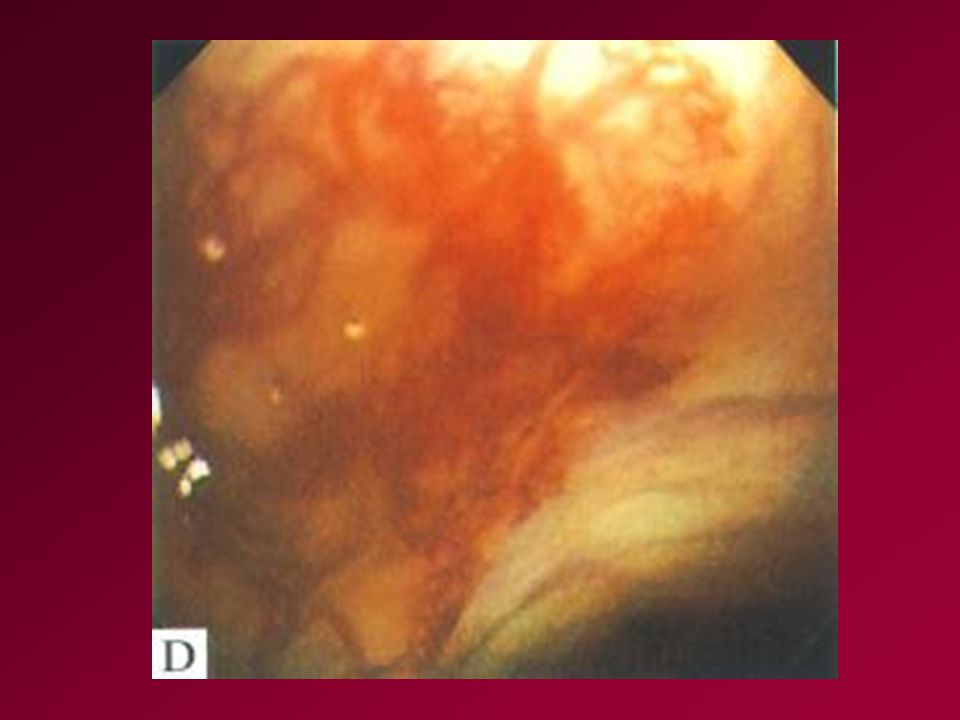
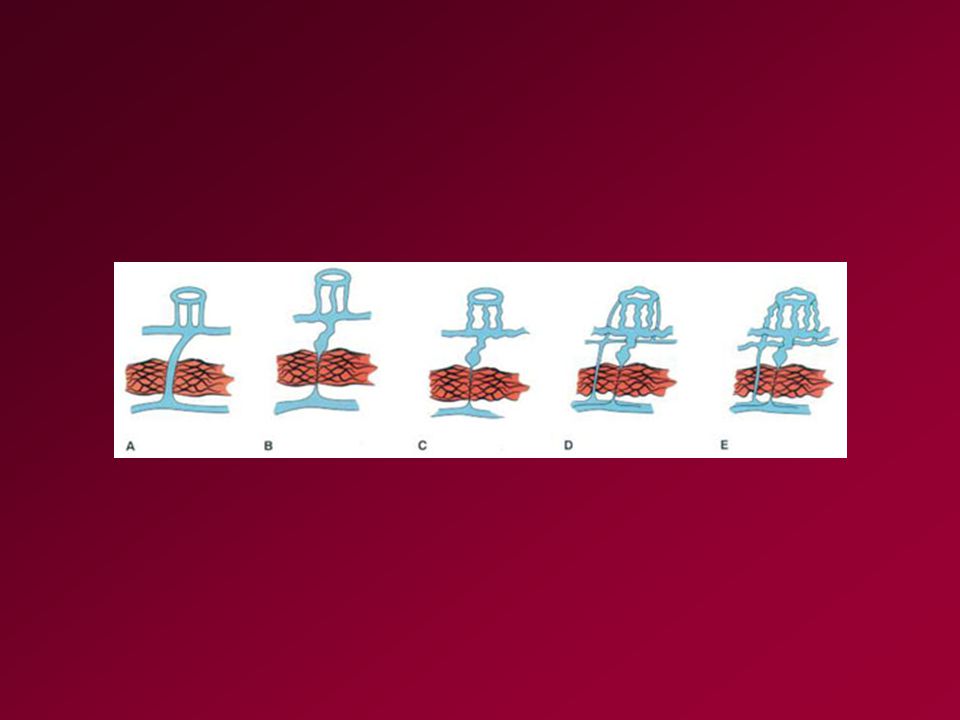
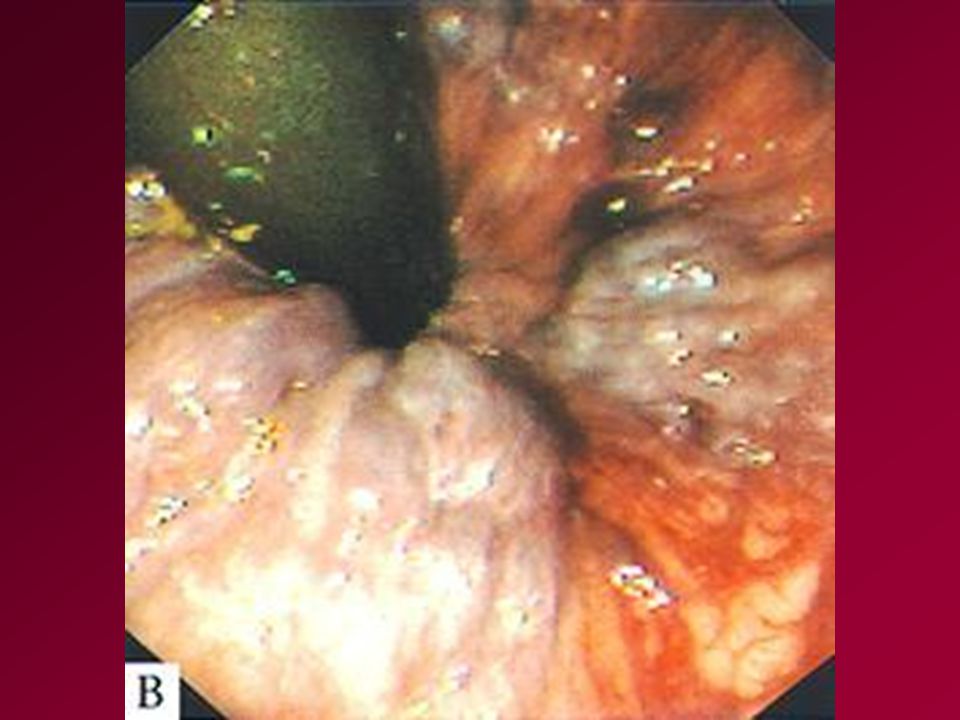
Arteriovenous Malformations
Vascular ectasias not associated with multisystem disorders Usually < 5mm in diameter Most commonly found in the right colon; can occur anywhere in the colon and in the stomach and small intestine < 10% with AVM’s will have bleeding Can present as hemorrhage or anemia without overt bleeding

47
Distribution of Angiodysplasia

48
Bleeding Can Occur from Polyps

49
Bleeding from Tumors

50
Case 4 A 68 year old man with severe coronary artery disease, claudication and a 6 month history of intermittent abdominal pain presents to the ER with a history of severe lower abdominal pain followed an hour later by passage of bright red blood per rectum. What are the key elements of this story?

51
Ischemic Colitis

53
Hemorrhoids

55
Radiation Proctitis

56
Infectious Colitis

57
Solitary Rectal Ulcer

58
Case 5 A 15 year old boy presents to the ER with a first ever episode of severe rectal bleeding. He is dizzy and his Hgb = 10.3g. He has no pain but has cramps just before a BM. The diagnosis is made on a bleeding scan.

59
Meckel’s Diverticulum

Similar presentations




























>")
 The McGraw-Hill Companies, Inc. Permission required for reproduction or display. 23-1 Chapter 23 Abdominal and Gastrointestinal Disorders.>")



