Download presentation
Presentation is loading. Please wait.

1
Essentials MA MURPHY FRCSI
Back to Department of Surgery Trinity College Dublin Abdominal Wall Hernia Essentials MA MURPHY FRCSI

2
Objectives Understand the term hernia Basic anatomical knowledge
Clinical features of common hernia Complications of hernias Examination of a hernia Differential diagnoses of a lump in the groin Management of hernia

3
Hernia A protrusion of an organ or tissue outside its’ normal compartment

4
Common External Hernias
ABDOMINAL WALL & GROIN Midline Umbilical Para- umbilical Epigastric Inguinal Direct/ Indirect/ Combined Femoral Incisional

6
Common Presentations A lump Comes and goes
Appears on straining /coughing A pain Dragging pain/ Pain on exertion Incidental finding on examination/ imaging Presenting as a complication Incarceration/ Intestinal obstruction

7
Inguinal Hernia Commonest external hernia Male preponderance
Infant / adult Direct / indirect / combined Weakness / increased pressure Cause pain / discomfort Carry risk of complications Treated surgically

8
Inguinal Hernia - History
OBJECTIVES Establish differential diagnoses Identify risk factors and significant co-morbid pathologies (e.g. increased intra-abdominal pressure due to ascites or chronic airways disease)
")
9
Inguinal Hernia - History
Onset Duration Symptoms Other hernia(e) Irreducibility Gastrointestinal system Respiratory system Surgery / anaesthesia
 Irreducibility. Gastrointestinal system. Respiratory system. Surgery / anaesthesia.")
10
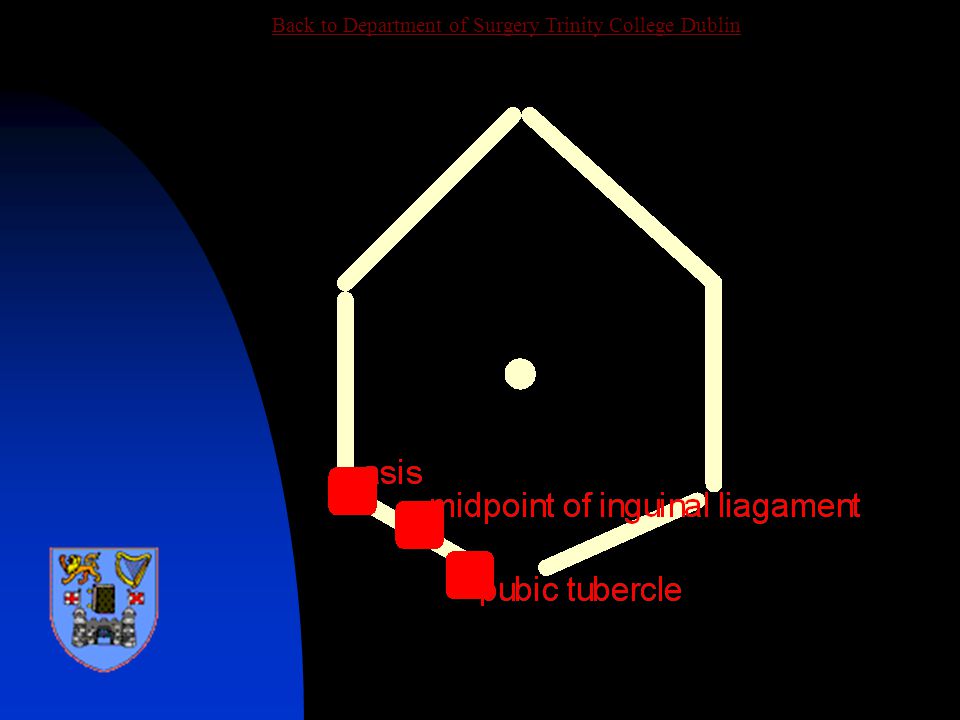
Inguinal Hernia - Examination
Surface markings Anterior superior iliac spine Pubic tubercle Midpoint of inguinal ligament

12
Inguinal Hernia - Examination
OBJECTIVES Confirm diagnoses Out rule differentials Establish type Determine contents Reducibility Identify co-morbid pathologies

13
Direct V’s Indirect Direct Post wall Less common Older Smaller
Hesselbachs Medial Lower risk Indirect Deep ring 70% Congenital Scrotal Lateral Strangulate

14
Inguinal Hernia Examination Standing / Lying Supine Cough impulse
Reducibility Contents Bowel sounds Scrotal contents

15
Differential Direct /Indirect/Combined Femoral hernia Hydrocele Lipoma
Lymph node Testicular tumour Saphenous varix

16
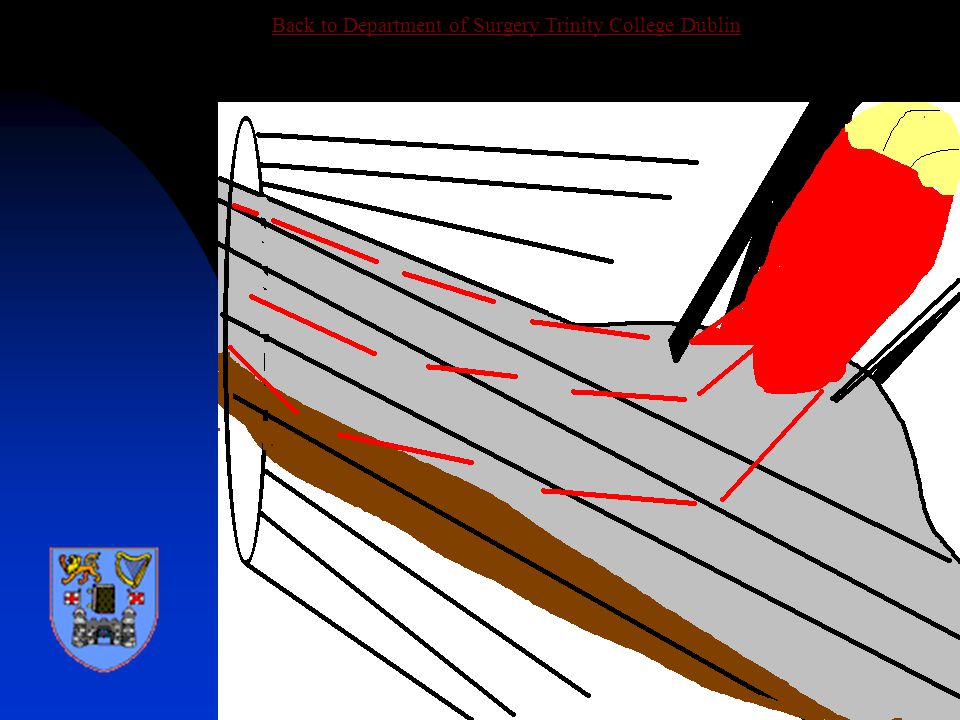
Inguinal Anatomy The inguinal canal represents the oblique passage through the anterior abdominal wall of the vas deferens (round ligament) It is 5cm long and lies directly above the medial half of the inguinal ligament

17
Inguinal Anatomy Floor Transversalis fascia
Medially the conjoint tendon Roof External oblique aponeurosis Laterally the conjoint tendon Skin and superficial fascia Above Conjoint tendon Below The inguinal ligament

18
Inguinal Anatomy Three nerves Ilio-inguinal (on not in)
Sympathetic fibers Genitofemoral Three layers of fascia Internal spermatic (transversalis f.) Cremasteric (conjoint tendon) External spermatic (ext. oblique)
 Cremasteric (conjoint tendon) External spermatic (ext. oblique)")
19
Inguinal Anatomy Three arteries Testicular (from the aorta)
Artery of the vas (external iliac) Cremasteric (inferior epigastric) Three other structures The vas deferens The pampniform plexus of veins Lymphatics (to aortic nodes)
 Cremasteric (inferior epigastric) Three other structures. The vas deferens. The pampniform plexus of veins. Lymphatics (to aortic nodes)")
20
TESTIS CORD STRUCTURES

21
Inguinal Anatomy

22
Hernia Anatomy

23
Indirect Hernia

24
Direct Inguinal Hernia

25
Hernia Complications Incarceration Strangulation
Intestinal obstruction

26
Varieties of Hernias Maydls W loop of intestine Richters
Partial inclusion of intestinal wall Sliding hernia Bladder Sigmoid colon/ appendix

27
Richters’ Hernia

28
Maydls’ Hernia

29
Hernia Management Investigations
None required for routine uncomplicated case Plain X-ray for suspected bowel obstruction Ultrasound in case of diagnostic uncertainty Herniogram rarely used Routine pre-op investigations

30
Hernia Treatment Surgery To relieve symptoms To prevent complications
Operations Open hernia repair Laparoscopic hernia repair Pre-peritoneal Intra- abdominal

31
Open Hernia Repair Day-case surgery Anaesthesia General Local
Operations Tension free Mesh repair (Lichtenstien) Darn repairs (Shouldice, Bassini)
 Darn repairs (Shouldice, Bassini)")
32
Open Hernia Repair Incision above medial half of inguinal ligament
External oblique opened from external ring to expose the cord and overlying ilioinguinal nerve Internal (deep) ring exposed Hernial sac identified and reduced Prolene mesh inserted to reinforce posterior wall and deep ring
 ring exposed. Hernial sac identified and reduced. Prolene mesh inserted to reinforce posterior wall and deep ring.")
33
Open Hernia Repair

34
Open Hernia Repair

35
Open Hernia Repair

36
Open Hernia Repair

42
Open Hernia Repair

43
Laparoscopic Repair

44
Laparoscopic Repair

45
Laparoscopic Repair

46
Surgery Complications
Trauma Nerve Artery (testicular atrophy) Intestine Haemorrhage Haematoma (infection) Infection Wound infection Chest Infection
 Intestine. Haemorrhage. Haematoma (infection) Infection. Wound infection. Chest Infection.")
47
Femoral Hernia Herniation through femoral canal
Appears below and lateral to pubic tubercle Relatively uncommon Commoner in females Contains omentum or small intestine High risk of strangulation Repaired surgically

48
Femoral Hernia

49
Femoral Hernia Repair

50
Summary Inguinal hernia is the commonest external hernia
Indirect hernias have a higher risk of strangulation Hernias are treated by surgery, to relieve symptoms and prevent complications Femoral hernias have a high risk of strangulation

51
Recommended Reading Ellis H. Clinical Anatomy

Similar presentations












>")











