Download presentation
Presentation is loading. Please wait.

1
INGUINAL CANAL Dr.LUBNA NAZLI ASST. PROF. ANATOMY RAK MHSU
Dt. 12/11/2007 Mon 8.30 a.m-9.30 am

2
Objectives Definition Inlet & its relations Outlet & its relations
Boundaries Contents Defensive mechanism Applied anatomy (hernias)
")
3
Before we start, lets look at :
Ant abdominal wall: It has 8 layers Skin Superficial fascia Ext oblique muscle Int oblique muscle Transversus abdominis Fascia transversalis Extra peritoneal tissue Parietal peritoneum

4
The normal structure of the abdominal wall

5
Ext oblique ORIGIN lower eight ribs
INSERTION Outer anterior half of iliac crest, inguinal lig, public tubercle and crest, and aponeurosis of anterior rectus sheath ACTION Supports abdominal wall, assists forced expiration, aids raising intraabdominal pressure and, with muscles of opposite side, abducts and rotates trunk NERVE Anterior primary rami (T7-12)
")
6
Int oblique ORIGIN Lumbar fascia, anterior two thirds of iliac crest and lateral two thirds of inguinal ligament INSERTION Costal margin, aponeurosis of rectus sheath (anterior and posterior ), conjoint tendon to pubic crest and pectineal line ACTION Supports abdominal wall, Conjoint tendon supports posterior wall of inguinal canal NERVE Anterior primary rami (T7-12) (conjoint tendon ilioinguinal nerve (L1))
, conjoint tendon to pubic crest and pectineal line. ACTION Supports abdominal wall, Conjoint tendon supports posterior wall of inguinal canal. NERVE Anterior primary rami (T7-12) (conjoint tendon ilioinguinal nerve (L1))")
7
Transversus abdominus
ORIGIN Costal margin, lumbar fascia, anterior two thirds of iliac crest and lateral half of inguinal ligament INSERTION Aponeurosis of posterior and anterior rectus sheath and conjoint tendon to pubic crest and pectineal line ACTION Supports abdominal wall, aids forced expiration and raising intra-abdominal pressure. Conjoint tendon supports posterior wall of inguinal canal NERVE Anterior primary rami (T7-12). Conjoint tendon ilioinguinal nerve (L1)
. Conjoint tendon ilioinguinal nerve (L1)")
8
Inguinal canal Definition :
It is a musculoaponeurotic tunnel extending from superficial inguinal ring to the deep inguinal ring. The inguinal canal is about 4 cm long and is directed obliquely and inferomedially through the inferior part of the anterolateral abdominal wall. The canal lies parallel to the medial half of the inguinal ligament.

10
Inguinal ligament: This ligament extends from the anterior superior iliac spine to the pubic tubercle. It is the lower free edge of the external oblique aponeurosis.

11
Inlet of inguinal canal
The inguinal canal has openings the deep and superficial inguinal rings. The deep inguinal ring is the entrance to the inguinal canal. It is an oval gap in the transversalis fascia. It is about 1.25 cm superior to the middle of the inguinal ligament. From the deep inguinal ring the vas deferens (or round ligament of the uterus in the female), and gonadal vessels pass to enter the inguinal canal. The transversalis fascia continues into the canal, forming the innermost covering (internal fascia) of the structures traversing the inguinal canal.
, and gonadal vessels pass to enter the inguinal canal. The transversalis fascia continues into the canal, forming the innermost covering (internal fascia) of the structures traversing the inguinal canal.")
13
Outlet The superficial, or external inguinal ring is the exit from the inguinal canal. It is a slitlike opening in the aponeurosis of the external oblique muscle, superolateral to the pubic tubercle. The medial and lateral margins of the superficial ring formed by the split in the aponeurosis are caller crura. The lateral crus is attached to the pubic tubercle and the medial crus is attached to the pubic crest.

15
The anterior wall of the canal is formed mainly by the aponeurosis of the external oblique with the lateral part of the wall being reinforced by fibres of the internal oblique. The posterior wall is formed by transversalis fascia with the medial part of the wall being reinforced by the conjoint tendon ( the merging of the internal oblique and transversus abdominal aponeurosis into a common tendon).
.")
16
The roof of the inguinal canal is formed by the arching fibres of the internal oblique and transverse abdominal muscles. The floor is formed by the superior surface of the inguinal ligament. It is reinforced in the medial part by the lacunar ligament (a reflected part or extension from the deep aspect of the inguinal ligament to the pectineal line of the superior pubic ramus).
.")
17
Contents The main content of the inguinal canal is the spermatic cord in males and the round ligament of the uterus in females. The canal also transmits the blood and lymphatic vessels and the ilioinguinal nerve L1.

18
Defensive mechanism(shutter mechanism)
The canal passes obliquely through the three anterior abdominal muscles so the two rings are at different positions. When intra abdominal pressure is increased the canal closes like a flap valve. The canal is protected by two of the anterior abdominal muscles. The superficial ring is protected posteriorly by the conjoint tendon. The deep ring is posterior to the muscular fibres of internal oblique.

19
Arched fibres of internal oblique and transversus act like demisphincters and obliterate the canal by bringing the roof in contact with the floor. Cremasteric plug: The cremaster muscle contracts and pulls the testis towards the superficial ring closing the outlet like a ball valve.

20
Applied anatomy A hernia is a protrusion of tissue (usually parietal peritoneum and viscera such as fat,gut or omentum) through or alongside an opening in the abdomen that is designed to allow a normal structure to enter or exit. Example: the deep inguinal ring may allow a hernia to appear alongside the spermatic cord, or in the femoral canal a hernia alongside the lymphatics.
 through or alongside an opening in the abdomen that is designed to allow a normal structure to enter or exit. Example: the deep inguinal ring may allow a hernia to appear alongside the spermatic cord, or in the femoral canal a hernia alongside the lymphatics.")
21
TYPES OF HERNIAS Indirect hernias arise lateral to the inferior epigastric vessels. Direct hernias arise medial to the inferior epigastric vessels

22
Other types of hernias ??

23
Causes ?

24
Indirect or oblique hernias
This is the most common of all abdominal hernias. It leaves the abdominal cavity lateral to the inferior epigastric vessels and enters the deep inguinal ring. The hernial sac is formed by a persistent processus vaginalis and is surrounded by all three fascial coverings of the spermatic cord. The hernia traverses the entire inguinal canal. It exits through the superficial inguinal ring and commonly enters the scrotum.

25
Indirect or oblique hernia entering the scrotum

26
Direct hernias This is also known as acquired inguinal hernia.
It is common in elderly men. The sac leaves the abdominal cavity medial to the inferior epigastric artery. It protrudes through an area of relative weakness in the posterior wall of the inguinal canal. The hernial sac is formed by transversalis fascia. It lies outside the processus vaginalis, which is usually obliterated, parallel to the spermatic cord and outside the inner one or two fascial coverings of the cord.

27
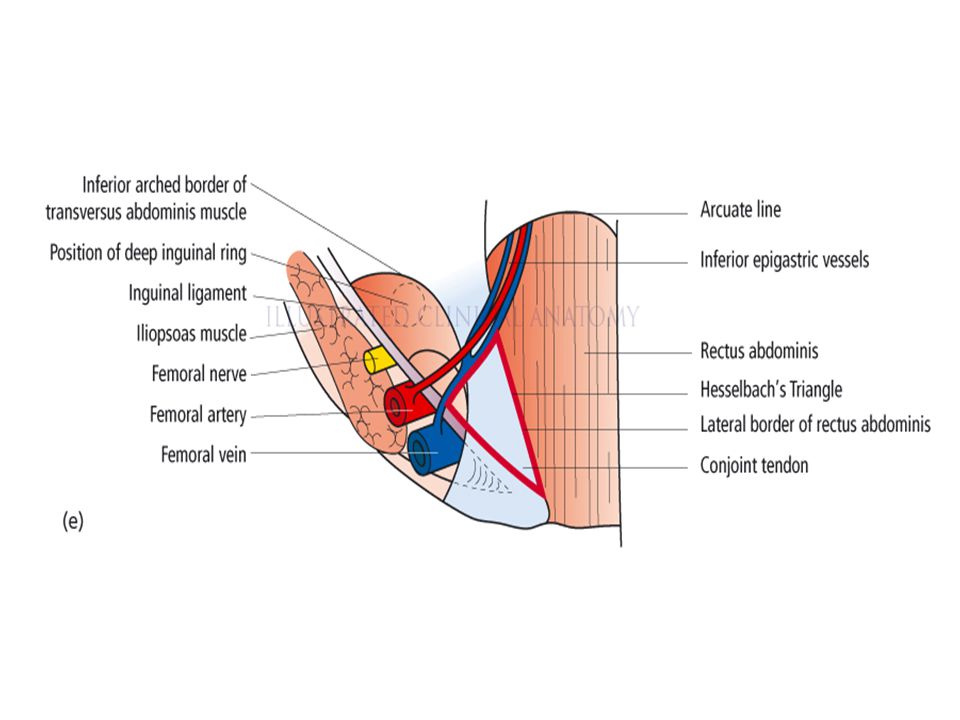
Direct hernias It does not traverse the entire inguinal canal.
The hernia protrudes through the inguinal triangle of Hesselbach that lies between the inferior epigastric artery superolaterally, the rectus abdominis medially and the inguinal ligament inferiorly. It emerges through or around the conjoint tendon to reach the superficial inguinal ring, gaining an outer covering of external spermatic fascia inside or parallel to that on the cord. It almost never enters the scrotum.

Similar presentations