Download presentation
Presentation is loading. Please wait.

1
Growth Hormone and puberty

2
Learning Objectives Intra uterine and Post natal Growth
Growth hormone release and its regulation Direct and Indirect actions of Growth hormone Applied aspect Puberty- role of nutrition and hormones Growth periods

3
Intrauterine Growth Genetic factors determine early growth; maternal factors more important later in gestation Important roles for Growth hormone, IGF-II (early in gestation), IGF-I(later in gestation) and insulin Poor maternal nutrition and smoking - lowers birth weight. Infants of diabetic mothers have increased insulin levels and are large. Smoking decreases vascularity of the placenta and decreases birth weight.
, IGF-I(later in gestation) and insulin. Poor maternal nutrition and smoking - lowers birth weight. Infants of diabetic mothers have increased insulin levels and are large. Smoking decreases vascularity of the placenta and decreases birth weight.")
4
Postnatal Growth Growth hormone, insulin, and thyroid hormone play major roles. Replacement of hormone deficiencies creates a period of catch-up growth, but it is soon replaced with a normal growth rate. There is no major role for gonadal sex steroids or for glucocorticoids on prepubertal growth but glucocorticoid excess will slow growth. Although fetal hypothyroidism does not decrease birth weight, hypothyroidism following delivery causes irreversible abnormalities in nervous system maturation, which in turn lead to mental retardation (cretinism). Acquired hypothyroidism later in childhood will slow growth and reduce bone advancement more than growth hormone deficiency, but will not cause mental retardation
. Acquired hypothyroidism later in childhood will slow growth and reduce bone advancement more than growth hormone deficiency, but will not cause mental retardation.")
5
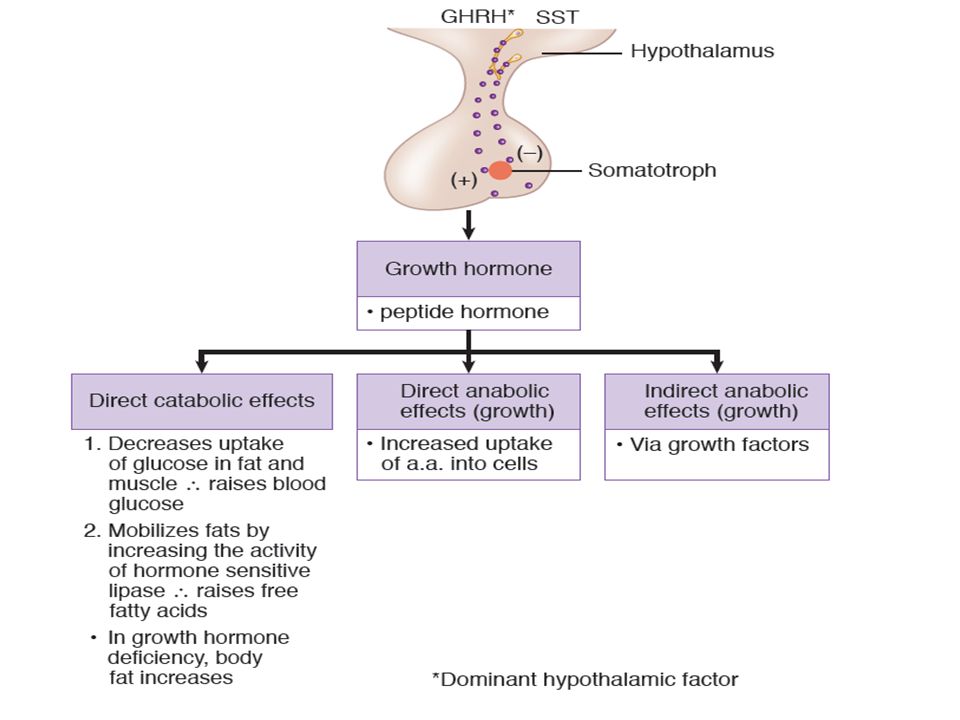
Growth hormone/ Somatotrophin
The somatotrope produces growth hormone (GH, also called somatotropin) and is part of the hypothalamus-pituitary-liver axis .). GH is a protein that is similar to prolactin (PRL) and human placental lactogen (HPL). It is the single most important hormone for growth to adult stature. Large diurnal variation. The largest burst occurs with peak secretion occurring in the early morning just before awakening. A major target of GH is the liver, where it stimulates the production of insulin-like growth factor type I (IGF-I GH secretion, like that of ACTH, shows prominent diurnal rhythms, with peak secretion occurring in the early morning just before awakening. Its secretion is stimulated during deep, slow-wave sleep (stages III and IV). GH secretion is lowest during the day. This rhythm is entrained to sleep-wake patterns rather than light-dark patterns, so a phase shift occurs in people who work night shifts. As is typical of anterior pituitary hormones, GH secretion is pulsatile
 and is part of the hypothalamus-pituitary-liver axis .). GH is a protein that is similar to prolactin (PRL) and human placental lactogen (HPL). It is the single most important hormone for growth to adult stature. Large diurnal variation. The largest burst occurs with peak secretion occurring in the early morning just before awakening. A major target of GH is the liver, where it stimulates the production of insulin-like growth factor type I (IGF-I. GH secretion, like that of ACTH, shows prominent diurnal rhythms, with peak secretion occurring in the early morning just before awakening. Its secretion is stimulated during deep, slow-wave sleep (stages III and IV). GH secretion is lowest during the day. This rhythm is entrained to sleep-wake patterns rather than light-dark patterns, so a phase shift occurs in people who work night shifts. As is typical of anterior pituitary hormones, GH secretion is pulsatile.")
7
CONTROL OF GH SECRETION
Primarily by hypophysiotrophic hormones of hypothalamus- Growth hormone releasing hormone [GHRH] Growth hormone release inhibiting hormone [GHRIH]

8
Notice that most of the factors that regulate GH secretion are identical to those that regulate glucagon (except for those boxed). These factors are consistent with their shared role as stress hormones.

9
Stimulate Growth hormone secretion Inhibit Growth hormone secretion
Decrease blood glucose Decrease blood FFA Starvation/Fasting Increase in circulating levels of amino acids Trauma, Stress ,excitement Exercise Deep Sleep (Stage III and IV) Growth hormone releasing Hormone Increase blood glucose Increase blood FFA Obesity Cortisol GHIH and IGF-I Growth hormone
 Growth hormone releasing Hormone. Increase blood glucose. Increase blood FFA. Obesity. Cortisol. GHIH and IGF-I. Growth hormone.")
10
Which of the following inhibits the secretion of growth hormone by the anterior pituitary?
(A) Sleep (B) Stress (C) Puberty (D) Somatomedins (E) Starvation (F) Hypoglycemia D
 Sleep. (B) Stress. (C) Puberty. (D) Somatomedins. (E) Starvation. (F) Hypoglycemia. D.")
11
The secretion of growth hormone is increased by a. Hyperglycemia
b. Exercise c. Somatostatin d. Hypothermia e. Free fatty acid B

12
Secretion of GH requires the presence of normal plasma levels of thyroid hormones. GH secretion is markedly reduced in hypothyroid individuals. is believed that these periodic bursts of GH secretionare caused by an increase in the rate of GHRH secretionand a fall in the rate of somatostatin secretion

13
Pulsatile GH secretion in an adolescent boy
and in an adult. In the adult, GH levels are reduced as a result of smaller pulse width and amplitude rather than a decrease in the number of pulses. GH secretion is pulsatile. The secretory pulses are much more likely to occur during the night in stages III and IV (non-REM) of sleep than during the day.
 of sleep than during the day.")
14
GH secretion The sectretory rates increases steadily from birth to early childhood, then remains stable during childhood, peaks at puberty (both in magnitude and frequency), declines after puberty to a stable level, and decreases in old age
, declines after puberty to a stable level, and decreases in old age.")
15
About 50% of GH in serum is bound to GH-binding protein (GHBP).
GHBP reduces renal clearance and thus increases the biological half-life of GH, which is about 20 minutes. The liver and kidney are major sites of GH degradation. Laron dwarfs, who lack normal GH receptors but have normal GH secretion, do not have detectable GHBP in their serum

16
Hypothalamus-pituitary-liver axis
Hypothalamus-pituitary-liver axis. ALS, acid labile subunit; GHBP, growth hormone-binding protein; GHRH, growth hormone-releasing hormone; IGFBP, insulin-like growth factor-binding protein; IGF-I, insulin-like growth factor I; SS, somatostatin

17
ANTERIOR PITUITARY negative feed back effect GH DIRECT ANTI INSULIN ACTION INDIRECT GROWTH PROMOTING ACTION + CORTISOL LIVER &OTHER ORGANS FAT CHO LIPOLYSIS SOMATOMEDIN BLOOD SUGAR & OTHER ANTI INSULIN EFFECT CHONDRO GENESIS SKELETAL GROWTH PROTEIN SYNTHESIS & CELL PROLIFERATION EXTRA SKELETAL GROWTH

19
Direct versus Indirect Actions of Growth Hormone
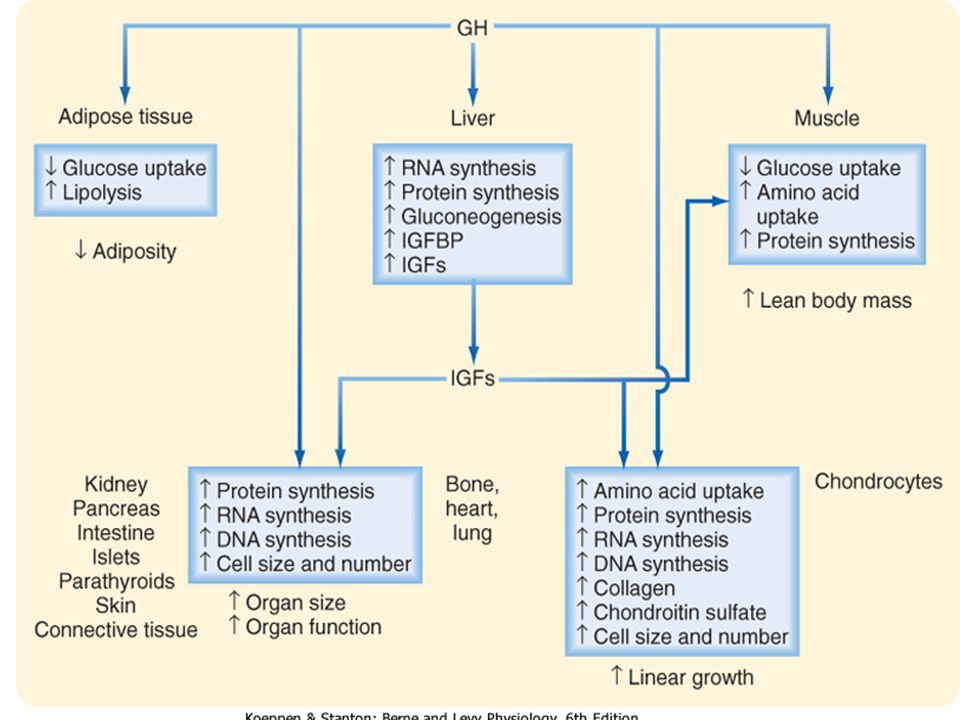
GH acts directly on the liver, muscle, and adipose tissue to regulate energy metabolism GH is a protein anabolic hormone GH is a lipolytic hormone GH alters carbohydrate metabolism. Many of its actions may be secondary to increased fat mobilization and oxidation GH antagonizes the action of insulin at the postreceptor level in skeletal muscle and adipose tissue (but not the liver) GH acts directly on the liver, muscle, and adipose tissue to regulate energy metabolism It shifts metabolism to lipid use for energy, thereby conserving carbohydrates and proteins. GH is a protein anabolic hormone that increases cellular amino acid uptake and incorporation into protein, and it represses proteolysis. Consequently, it produces nitrogen retention (positive nitrogen balance) and decreases urea production. The muscle wasting that occurs concomitant with aging has been proposed to be caused, at least in part, by the decrease in GH secretion that occurs with aging GH is a lipolytic hormone. It activates hormone-sensitive lipase and therefore mobilizes neutral fats from adipose tissue. As a result, serum fatty acid levels rise after GH administration, more fats are used for energy production, and fatty acid uptake and oxidation increase in skeletal muscle and liver. GH can be ketogenic as a result of the increase in fatty acid oxidation (the ketogenic effect of GH is not seen when insulin levels are normal). If insulin is given along with GH, the lipolytic effects of GH are abolished. GH alters carbohydrate metabolism. Many of its actions may be secondary to increased fat mobilization and oxidation. (Remember, an increase in serum free fatty acids inhibits uptake of glucose in skeletal muscle and adipose tissue.) After administration of GH, blood glucose rises. The hyperglycemic effects of GH are mild and slower than those of glucagon and epinephrine. The increase in blood glucose results in part from decreased glucose uptake and use in skeletal muscle and adipose tissue. Liver glucose output increases, and this is probably not a result of glycogenolysis. In fact, glycogen levels can rise after administration of GH. However, the increase in fatty acid oxidation and hence the rise in liver acetyl coenzyme A (acetyl CoA) stimulate gluconeogenesis, followed by increased glucose production from substrates such as lactate and glycerol.
 GH acts directly on the liver, muscle, and adipose tissue to regulate energy metabolism It shifts metabolism to lipid use for energy, thereby conserving carbohydrates and proteins. GH is a protein anabolic hormone that increases cellular amino acid uptake and incorporation into protein, and it represses proteolysis. Consequently, it produces nitrogen retention (positive nitrogen balance) and decreases urea production. The muscle wasting that occurs concomitant with aging has been proposed to be caused, at least in part, by the decrease in GH secretion that occurs with aging. GH is a lipolytic hormone. It activates hormone-sensitive lipase and therefore mobilizes neutral fats from adipose tissue. As a result, serum fatty acid levels rise after GH administration, more fats are used for energy production, and fatty acid uptake and oxidation increase in skeletal muscle and liver. GH can be ketogenic as a result of the increase in fatty acid oxidation (the ketogenic effect of GH is not seen when insulin levels are normal). If insulin is given along with GH, the lipolytic effects of GH are abolished. GH alters carbohydrate metabolism. Many of its actions may be secondary to increased fat mobilization and oxidation. (Remember, an increase in serum free fatty acids inhibits uptake of glucose in skeletal muscle and adipose tissue.) After administration of GH, blood glucose rises. The hyperglycemic effects of GH are mild and slower than those of glucagon and epinephrine. The increase in blood glucose results in part from decreased glucose uptake and use in skeletal muscle and adipose tissue. Liver glucose output increases, and this is probably not a result of glycogenolysis. In fact, glycogen levels can rise after administration of GH. However, the increase in fatty acid oxidation and hence the rise in liver acetyl coenzyme A (acetyl CoA) stimulate gluconeogenesis, followed by increased glucose production from substrates such as lactate and glycerol.")
20
Indirect Effects of Growth Hormone on Growth
Most of the anabolic actions of growth hormone are an indirect result of increased production of growth factors, which are called somatomedins, or insulin-like growth factors (IGFs). A major growth factor is somatomedin C, also called IGF-I GH increases skeletal and visceral growth; children without GH show growth stunting or dwarfism. GH also promotes cartilage growth, long-bone length, and periosteal growth. Most of these effects are mediated by a group of hormones called insulin-like growth factors.
. A major growth factor is somatomedin C, also called IGF-I. GH increases skeletal and visceral growth; children without GH show growth stunting or dwarfism. GH also promotes cartilage growth, long-bone length, and periosteal growth. Most of these effects are mediated by a group of hormones called insulin-like growth factors.")
21
Specific Properties of the IGFs
IGF-I is a major anabolic growth factor-- increases the synthesis of cartilage (chondrogenesis) in the epiphyseal plates of long bones, thereby increasing bone length. Similar in structure to proinsulin and has some insulin-like activity Because it has a long half-life, plasma IGF-I serves as a reflection of 24-hour growth hormone secretion. Growth hormone secretion is difficult to measure directly because it is secreted in pulses and mainly at night. It is also hypothesized that circulating IGFs increase lean body mass. IGF-II is another somatomedin, the importance of which is not well understood but may have a role in fetal development. Circulates in the blood tightly bound to a large protein, whose production is also dependent on growth hormone. Being bound to a protein, the plasma half-life is very long (20 hours). The decreased lean body mass of aging may, in part, be due to the concomitant decrease in IGFs. IGFs also decrease in catabolic states, especially protein calorie malnutrition.
 in the epiphyseal plates of long bones, thereby increasing bone length. Similar in structure to proinsulin and has some insulin-like activity. Because it has a long half-life, plasma IGF-I serves as a reflection of 24-hour growth hormone secretion. Growth hormone secretion is difficult to measure directly because it is secreted in pulses and mainly at night. It is also hypothesized that circulating IGFs increase lean body mass. IGF-II is another somatomedin, the importance of which is not well understood but may have a role in fetal development. Circulates in the blood tightly bound to a large protein, whose production is also dependent on growth hormone. Being bound to a protein, the plasma half-life is very long (20 hours). The decreased lean body mass of aging may, in part, be due to the concomitant decrease in IGFs. IGFs also decrease in catabolic states, especially protein calorie malnutrition.")
22
Complementary regulation of GH and insulin secretion coordinates availability of nutrients with anabolism and either caloric storage or mobilization

23
When ample supplies of nutrients are available, high serum amino acid levels stimulate GH and insulin secretion, and high serum glucose levels stimulate insulin secretion. The high serum GH, insulin, and nutrient supply stimulate IGF production, and these conditions are appropriate for growth. However, if the diet is high in calories but low in amino acids, the hormonal response is different. Whereas high carbohydrate availability results in high insulin availability, low serum amino acid levels inhibit GH and IGF production. These conditions allow dietary carbohydrates and fats to be stored, but conditions are unfavorable for tissue growth. On the other hand, during fasting, when the availability of nutrients decreases, serum GH levels rise and serum insulin levels fall (because of hypoglycemia). IGF production is low, and the conditions are not favorable for growth. In these circumstances, the rise in GH secretion is beneficial because it promotes fat mobilization while minimizing tissue protein loss. In the absence of insulin, peripheral tissue glucose use decreases, thereby conserving glucose for essential tissues such as the brain Complementary regulation of GH and insulin secretion coordinates availability of nutrients with anabolism and either caloric storage or mobilization. Note that both hormones are increased by protein and that both stimulate protein synthesis
. IGF production is low, and the conditions are not favorable for growth. In these circumstances, the rise in GH secretion is beneficial because it promotes fat mobilization while minimizing tissue protein loss. In the absence of insulin, peripheral tissue glucose use decreases, thereby conserving glucose for essential tissues such as the brain. Complementary regulation of GH and insulin secretion coordinates availability of nutrients with anabolism and either caloric storage or mobilization. Note that both hormones are increased by protein and that both stimulate protein synthesis.")
24
Correct statements about human growth hormone include which of the following?
a. It is synthesized in the hypothalamus b. It stimulates production of somatomedins by the liver c. Its release is stimulated by somatostatin d. It causes a decrease in lipolysis e. It is deficient in acromegaly

25
The basic effects of growth hormone on body metabolism include
a. Decreasing the rate of protein synthesis b. Increasing the rate of use of carbohydrate c. Decreasing the mobilization of fats d. Increasing the use of fats for energy e. Inhibition of insulin-like growth factor 1

26
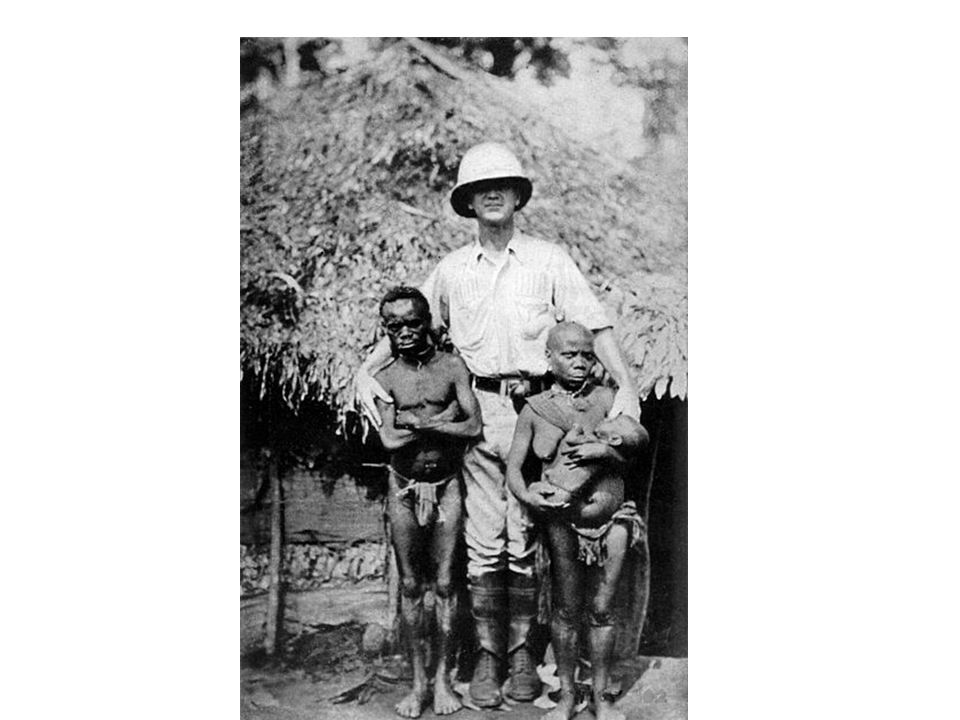
APPLIED PHYSIOLOGY GH SECRETION-DWARFISM Stunted growth
Delayed skeletal growth Normal intelligence. Well proportioned Congenital deficiency is associated with decreased birth length. Growth hormone deficiency leads to dwarfism. Growth hormone deficiency following puberty is not a major problem. Classic congenital deficiency creates short stature, delayed skeletal maturation, proneness to episodes of hypoglycemia, and a chubby, immature facial appearance. Acquired deficiency may be due to a hypothalamic–pituitary tumor.

27
Hypothyroid dwarfs (cretins) retain their infantile proportions, whereas dwarfs of the constitutional type and, to a lesser extent, of the hypopituitary type have proportions characteristic of their chronologic age Thyroid hormones have widespread effects on the ossification of cartilage, the growth of teeth, the contours of the face, and the proportions of the body. Hypothyroid dwarfs (also known as cretins) therefore have infantile features. Patients who are dwarfed because of panhypopituitarism have features consistent with their chronologic age until puberty, but since they do not mature sexually, they have juvenile features in adulthood
 therefore have infantile features. Patients who are dwarfed because of panhypopituitarism have features consistent with their chronologic age until puberty, but since they do not mature sexually, they have juvenile features in adulthood.")
28
Normal growth requires not only normal levels of GH but also normal levels of thyroid hormones, insulin, and sex steroids

29
Relative importance of hormones in human growth at various ages.
The growth spurt that occurs at the time of puberty is due in part to the protein anabolic effect of androgens, and the secretion of adrenal androgens increases at this time in both sexes; however, it is also due to an interaction among sex steroids, growth hormone, and IGF-I. Treatment with estrogens and androgens increases the secretion of growth hormone in response to various stimuli and increases plasma IGF-I secondary to this increase in circulating growth hormone. This, in turn, causes growth. Although androgens and estrogens initially stimulate growth, estrogens ultimately terminate growth by causing the epiphyses to fuse to the long bones (epiphysial closure). Once the epiphyses have closed, linear growth ceases This is why patients with sexual precocity are apt to be dwarfed. On the other hand, men who were castrated before puberty tend to be tall because their estrogen production is decreased and their epiphyses remain open, allowing some growth to continue past the normal age of puberty. When growth hormone is administered to hypophysectomized animals, the animals do not grow as rapidly as they do when treated with growth hormone plus thyroid hormones. Thyroid hormones alone have no effect on growth in this situation. Their action is therefore permissive to that of growth hormone, possibly via potentiation of the actions of somatomedins. Thyroid hormones also appear to be necessary for a completely normal rate of growth hormone secretion; basal growth hormone levels are normal in hypothyroidism, but the response to hypoglycemia is frequently blunted. Thyroid hormones have widespread effects on the ossification of cartilage, the growth of teeth, the contours of the face, and the proportions of the body. Hypothyroid dwarfs (also known as cretins) therefore have infantile features .Patients who are dwarfed because of panhypopituitarism have features consistent with their chronologic age until puberty, but since they do not mature sexually, they have juvenile features in adulthood
. Once the epiphyses have closed, linear growth ceases This is why patients with sexual precocity are apt to be dwarfed. On the other hand, men who were castrated before puberty tend to be tall because their estrogen production is decreased and their epiphyses remain open, allowing some growth to continue past the normal age of puberty. When growth hormone is administered to hypophysectomized animals, the animals do not grow as rapidly as they do when treated with growth hormone plus thyroid hormones. Thyroid hormones alone have no effect on growth in this situation. Their action is therefore permissive to that of growth hormone, possibly via potentiation of the actions of somatomedins. Thyroid hormones also appear to be necessary for a completely normal rate of growth hormone secretion; basal growth hormone levels are normal in hypothyroidism, but the response to hypoglycemia is frequently blunted. Thyroid hormones have widespread effects on the ossification of cartilage, the growth of teeth, the contours of the face, and the proportions of the body. Hypothyroid dwarfs (also known as cretins) therefore have infantile features .Patients who are dwarfed because of panhypopituitarism have features consistent with their chronologic age until puberty, but since they do not mature sexually, they have juvenile features in adulthood.")
30
OTHER CAUSES OF DWARFISM
It can be due to GHRH deficiency, growth hormone deficiency, or deficient secretion of IGF-I. African pygmies—normal serum GH levels, but they do not exhibit the normal rise in IGF that occurs at puberty. They also may have a partial defect in GH receptors .Normal GH & somatomedin IGF-1 Laron dwarf—genetic defect in expression of the GH receptor such that the response to GH is impaired. Thus, although serum GH levels are normal to high, Laron dwarfs do not produce IGFs in response to GH. Treating patients afflicted by Laron dwarfism with GH will not correct the growth deficiency Kwashiorkor-- GH, but retarted growth following protein deficiency- somatomedin Juvenile diabetes Cretinism

32
It is also part of the syndrome of gonadal dysgenesis seen in patients who have an XO chromosomal pattern Chronic abuse and neglect can also cause dwarfism in children, independent of malnutrition. This condition is known as psychosocial dwarfism or the Kaspar Hauser syndrome, named for the patient with the first reported case Achondroplasia, the most common form of dwarfism in humans, is characterized by short limbs with a normal trunk. It is an autosomal dominant condition caused by a mutation in the gene that codes for fibroblast growth factor receptor 3 (FGFR3). This member of the fibroblast growth receptor family is normally expressed in cartilage and the brain
. This member of the fibroblast growth receptor family is normally expressed in cartilage and the brain.")
33
Growth hormone excess Before puberty: causes gigantism (excess linear growth) because of excessive stimulation of epiphyseal plates. After puberty causes: increases organ size, increased hand and foot size, enlarged tongue, facial coarseness, insulin resistance Treatment is with somatostatin analogues (octreotide)
")
34
INCREASED GH SECRETION
GIANTISM OR GIGANTISM Secretion of GH before epiphysial closure Tall stature > 8 feet Large hands & feet Bilateral gynaecomastia, loss of libido, impotence, amenorrhea & infertility Excessive growth of internal organs Hyperglycemia

35
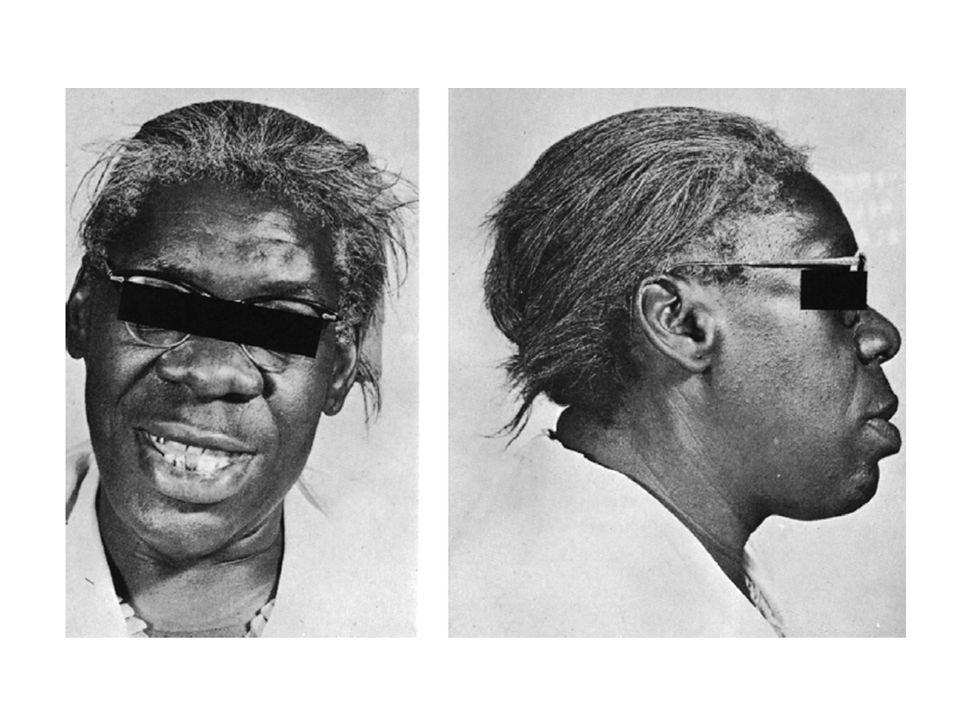
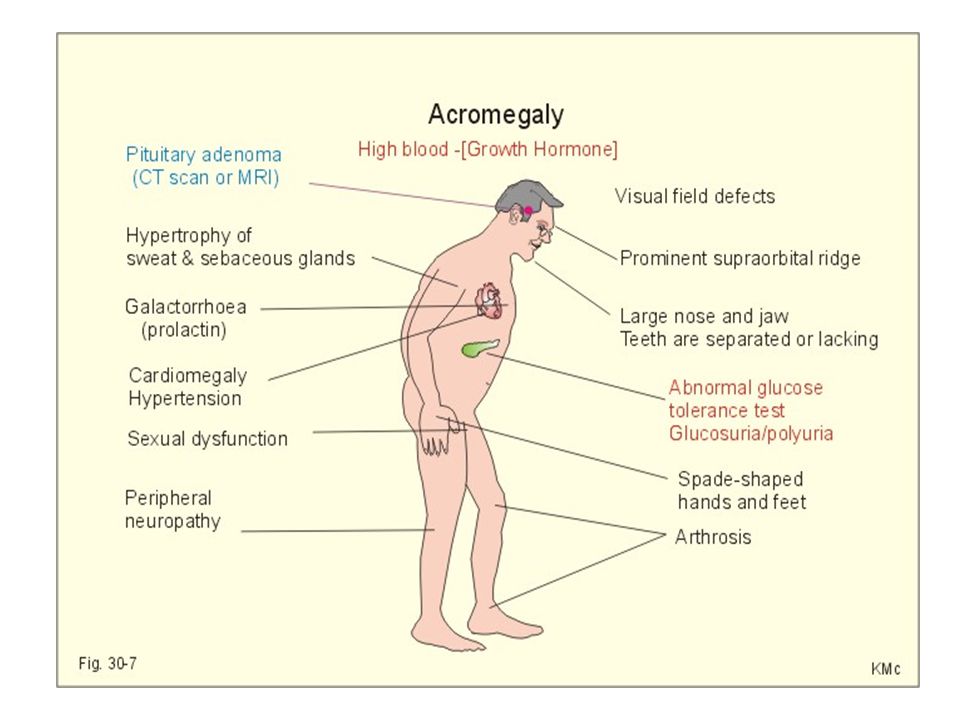
ACROMEGALY - SECRETION -AFTER THE CLOSURE OF EPIPHYSIS
Acral-distal parts, Megaly-enlargement It is almost always due to macroadenoma (> 1 cm dia) of the anterior pituitary and second in frequency to prolactinomas. Ectopic GHRH secretion occurs but is rare Some tumors contain lactotrophs, and elevated prolactin can cause hypogonadism and galactorrhea. Measurement of IGF-I is a useful screening measure and confirms diagnosis with the lack of growth hormone suppression by oral glucose (not somatostatin). Adrenal size due to acth Body hair growth , protein content, fat content Precipitation of osteoarthritis Hyperglycemia Bitemporal hemianopia Gynaecomastia with milk secretion Urinary excretion of creatinine
 of the anterior pituitary and second in frequency to prolactinomas. Ectopic GHRH secretion occurs but is rare. Some tumors contain lactotrophs, and elevated prolactin can cause hypogonadism and galactorrhea. Measurement of IGF-I is a useful screening measure and confirms diagnosis with the lack of growth hormone suppression by oral glucose (not somatostatin). Adrenal size due to acth. Body hair growth , protein content, fat content. Precipitation of osteoarthritis. Hyperglycemia. Bitemporal hemianopia. Gynaecomastia with milk secretion. Urinary excretion of creatinine.")
36
A patient is diagnosed with acromegaly
A patient is diagnosed with acromegaly. Patients with this disease typically have a. Decreased gluconeogenesis b. Hypoglycemia c. Insulin resistance d. Decreased protein synthesis e. Decreased lipolysis

38
Enlargement of flat bones- skull,Hands & feet
There is characteristic proliferation of cartilage, bone and soft tissue, visceral, and cardiomegaly. Enlargement of flat bones- skull,Hands & feet Prognathism, frontal bossing, kyphosis, Thickening of skin- acromegalic facies Hypertrophy of int.Organs—cardiomegaly, hepatomegaly, renomegaly, splenomegaly, enlarged tongue growth hormone excess directly causes the hyperglycemia and insulin resistance. Observable changes include enlargement of the hands and feet (acral parts) and coarsening of the facial features, including downward and forward growth of the mandible. Also, increased hat size.
 and coarsening of the facial features, including downward and forward growth of the mandible. Also, increased hat size.")
41
Which treatment would provide the greatest therapeutic benefit in patients with acromegaly?
(A) Glucocorticoid (B) Somatostatin (C) Growth hormone (D) Insulin (E) GHRH (F) Thyroid hormone
 Glucocorticoid. (B) Somatostatin. (C) Growth hormone. (D) Insulin. (E) GHRH. (F) Thyroid hormone.")
42
Puberty

43
Rate of growth in boys and girls from birth to age 20
The first period of accelerated growth is partly a continuation of the fetal growth period. The second growth spurt, at the time of puberty, is due to growth hormone, androgens, and estrogens, and the subsequent cessation of growth is due in large part to closure of the epiphyses in the long bones by estrogens .After this time, further increases in height are not possible. Because girls mature earlier than boys, this growth spurt appears earlier in girls. Of course, in both sexes the rate of growth of individual tissues

44
Growth of different tissues at various ages as a percentage of size at age 20

45
Relative importance of hormones in human growth at various ages.

46
PULSATILE SECRETION OF GNRH, FSH, AND LH
The primary event at puberty is the initiation of pulsatile secretion of GnRH. This new pattern of GnRH secretion drives a parallel pulsatile secretion of FSH and LH Initiation Genetically programmed Neuronal maturation Nutrition and stress Melatonin

47
Reproductive Changes Hypothalamic pulse generator increases activity just before physical changes at puberty. First noted sign in a female is breast development; first by estrogen(promotes duct growth) then progesterone (promotes development of milk-producing alveolar cells). First noted sign in a male is enlargement of the testes. Mainly FSH stimulating seminiferous tubules Pubic hair development in males and females is dependent on androgen
 then progesterone (promotes development of milk-producing alveolar cells). First noted sign in a male is enlargement of the testes. Mainly FSH stimulating seminiferous tubules. Pubic hair development in males and females is dependent on androgen.")
48
CHARACTERISTICS OF PUBERTY
In males: Leydig cell proliferation in the testes, and increased synthesis and secretion of testosterone There is growth of the testes, prostate. There is a pronounced linear growth spurt, and the epiphyses close when adult height is attained. pubic and axillary hair appears, and there is growth of the penis, lowering of the voice, and initiation of spermatogenesis.

49
a burst of testosterone secretion occurs in male fetuses before birth In the neonatal period there is another burst, with unknown function, but thereafter the Leydig cells become quiescent. There follows in all mammals a period in which the gonads of both sexes are quiescent until they are activated by gonadotropins from the pituitary to bring about the final maturation of the reproductive system. This period of final maturation is known as adolescence

50
Changes in plasma hormone concentrations during puberty in boys and girls
Stage 1 of puberty is preadolescence in both sexes. In boys, stage 2 is characterized by beginning enlargement of the testes, stage 3 by penile enlargement, stage 4 by growth of the glans penis, and stage 5 by adult genitalia. In girls, stage 2 is characterized by breast buds, stage 3 by elevation and enlargement of the breasts, stage 4 by projection of the areolas, and stage 5 by adult breasts

51
In females: Synthesis of estradiol by the ovaries. The first event is thelarche, the development of breasts, followed by pubarche, the development of axillary and pubic hair, and then by menarche, the first menstrual period.. The growth spurt and closure of the epiphyses typically begin and end earlier in girls than in boys.

52
Growth Changes During puberty, androgens promote the secretion in the following anabolic sequence: At puberty, if T4 is normal, ↑ androgens drive ↑ growth hormone, which drives ↑ IGF-I. In males, the increased androgen arises from the testes (testosterone); in females, from the adrenals (adrenarche). Near the end of puberty, androgens promote the mineralization (fusion or closure) of the epiphyseal plates of long bones. Estrogen can also cause plate closure, even in men. In females, the growth spurt begins early in puberty and is near completion by menarche. In males, the growth spurt develops near the end of puberty. IGF-I is the major stimulus for cell division of the cartilage-synthesizing cells located in the epiphyseal plates of long bones.
; in females, from the adrenals (adrenarche). Near the end of puberty, androgens promote the mineralization (fusion or closure) of the epiphyseal plates of long bones. Estrogen can also cause plate closure, even in men. In females, the growth spurt begins early in puberty and is near completion by menarche. In males, the growth spurt develops near the end of puberty. IGF-I is the major stimulus for cell division of the cartilage-synthesizing cells located in the epiphyseal plates of long bones.")
Similar presentations









 SST (somatostatin) (-) Anterior Pituitary: Hypothalamus: GHRH (+) GH (somatotropin) Liver: IGF (somatomedins)>")

 1 cm in diameter and 0.5 to 1 gm in weight Lies in sella turcica (bony cavity at the base of brain Connected to hypothalamus.>")



. Is located at the base of the brain in a small.>")


 Growth of an individual or an organ involves: – Increase both in cell number and cell size – Differentiation.>")

