Download presentation
Presentation is loading. Please wait.

1
Holes in the lung Dr. Ahmed Refaey, FRCR

2
References Cystic & cavitary lung diseases. Mayo clinic proceeding 2003;744752 HRCT , W.Richard webb, UCSF interactive radiology series Radiology review manual. Wolfgang Dahnert Diagnostic imaging , Chest , Gurney et al James reed in chest imaging Diffuse lung diseases. Prof. Mamdouh Mahfouz

4
Holes in the lung Cyst - thin walled ( 1-3 mm) - alone or in groups
Cavity - represents areas of tissue necrosis & clearing within areas of parenchymal opacification. - thick walled ( > 3 mm ) - suggests a more aggressive pathology than a cyst.
 - suggests a more aggressive pathology. than a cyst.")
5
Holes in the lung Focal * cyst * cavity Diffuse
Lymphangioleiomyomatosis Tuberous sclerosis L.C.Histeocytosis Honeycombing disease Emphysema

6
Focal holes in the lung Cyst Cavity * Congenital --- - Br. Cyst - CCAM
* Bleb * Bulla * Pneumatocele * Infection---hydatid -coccidioidomycosis -PCP Cavity * neoplastic –Br. Ca - metastasis - lymphoma * infection bacteria - fungal - parasites * immunologic - wegener’s gr. - Rh. nodules * septic emboli * bronchiectasis

7
In cystic lesions, benign nature is often be assumed, while cavitary lesions usually suggest more aggressive pathology.

8
Woodring et al studied the diagnostic implications of cavitary wall thickness
1 mm all benign < 4mm % benign 5-15 mm equally divided > 15 mm % malignant

9
Focal cystic lung disease
Congenital * bronchogenic cyst * CCAM ( cystic adenomatoid malformation ) Bulla Bleb Pneumatocele Infection * coccidioidomycosis * PCP * hydatid disease
 Bulla. Bleb. Pneumatocele. Infection. * coccidioidomycosis. * PCP. * hydatid disease.")
10
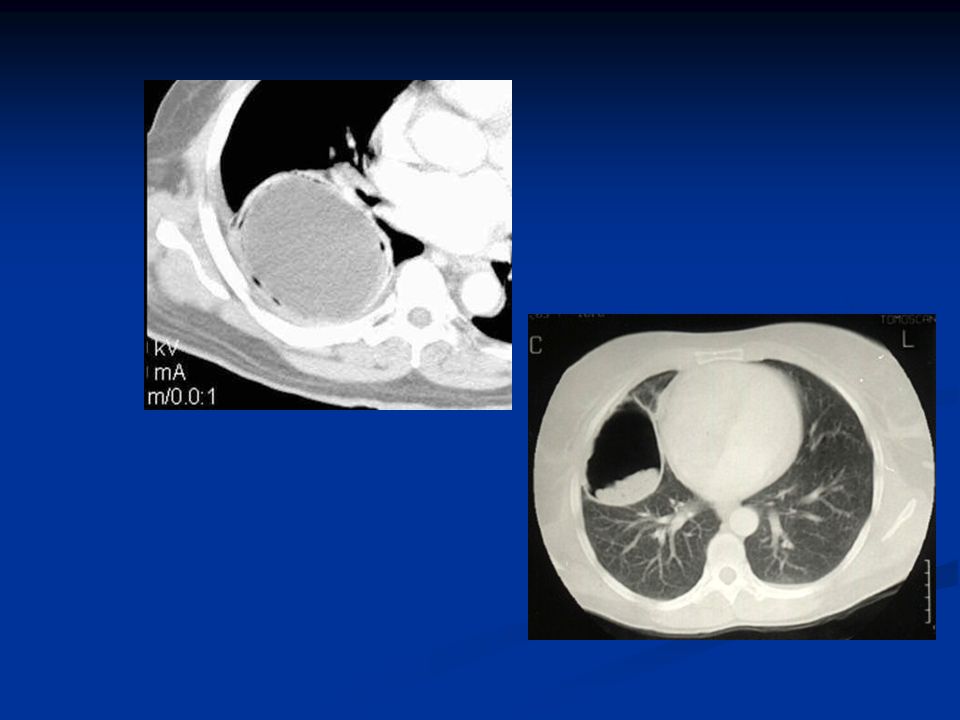
Bronchogenic cyst * 2/3 in mediastinum
* 1/3 in lung parenchyma, usually near hilum * may contain air, fluid or both

12
Congenital cystic adenomatoid malformation ( CCAM )
* air , fluid , or air-fluid containing cysts of varying sizes * 3 types are recognized based on cyst size & number - type or more large cysts(2-10cm) - type 2---neumerous small cysts - type 3 – solid with microcysts
 - type 2---neumerous small cysts. - type 3 – solid with microcysts.")
14
Bulla * intraparenchymal, more than 1 cm.
* result from coalescence of emphsematous spaces or from a Ball-valve type of air-way obstruction.

16
Bleb * usually located in the apex of lung within the pleura

17
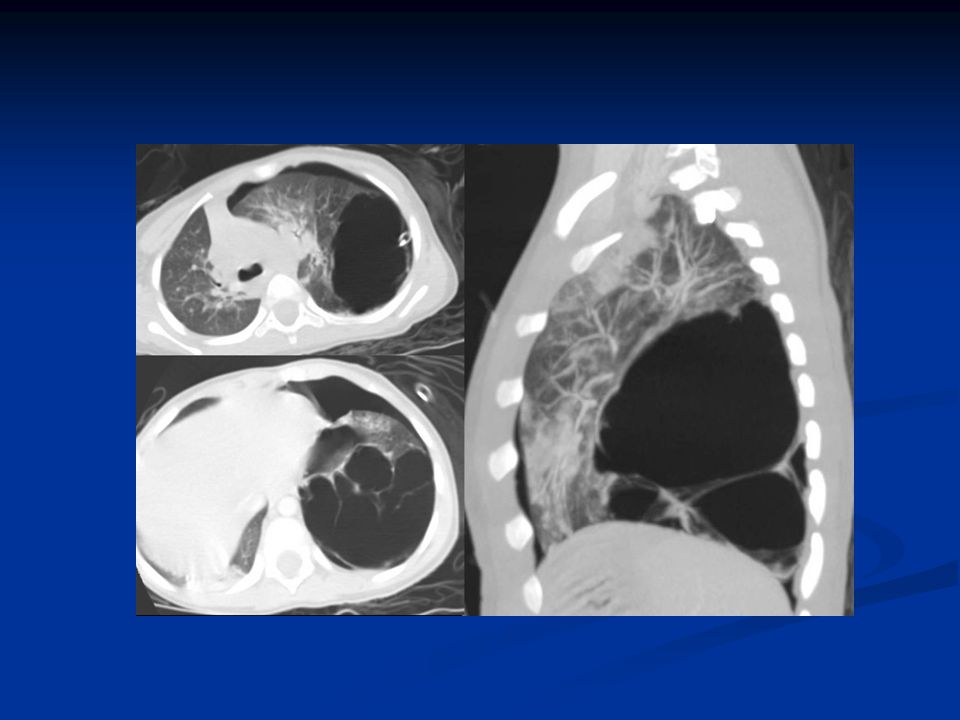
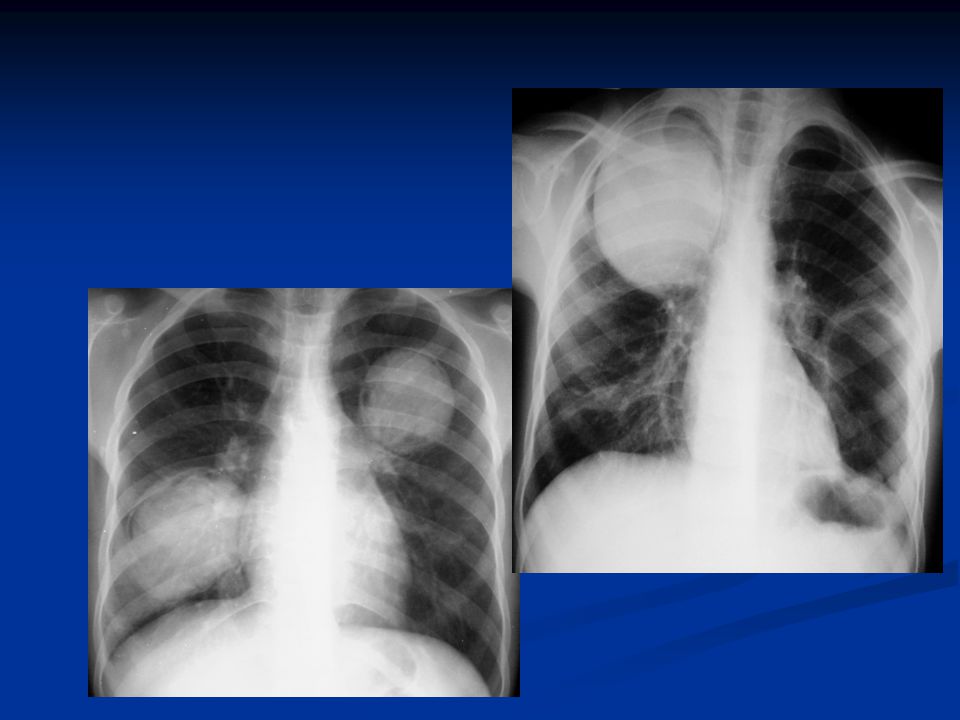
Pneumatocele typically associated with infection, particularly staph. Pneumonia in children characteristically increase in size over time. probably due to Ball-valve air-trapping. resolves eventually. May reach a large size to fill the hemi- thorax

20
Infections * { coccidioidomycosis } * { PCP } * { hydatid disease }
Most of the other infections of the lung tend to cause cavitary lesion.

21
Coccidioidomycosis * endemic in southwestern United States and Mexico.

22
Pneumocytis carnii pneumonia PCP
* in immunocompromised patients * upper lobar predilection * pneumothorax 35%

24
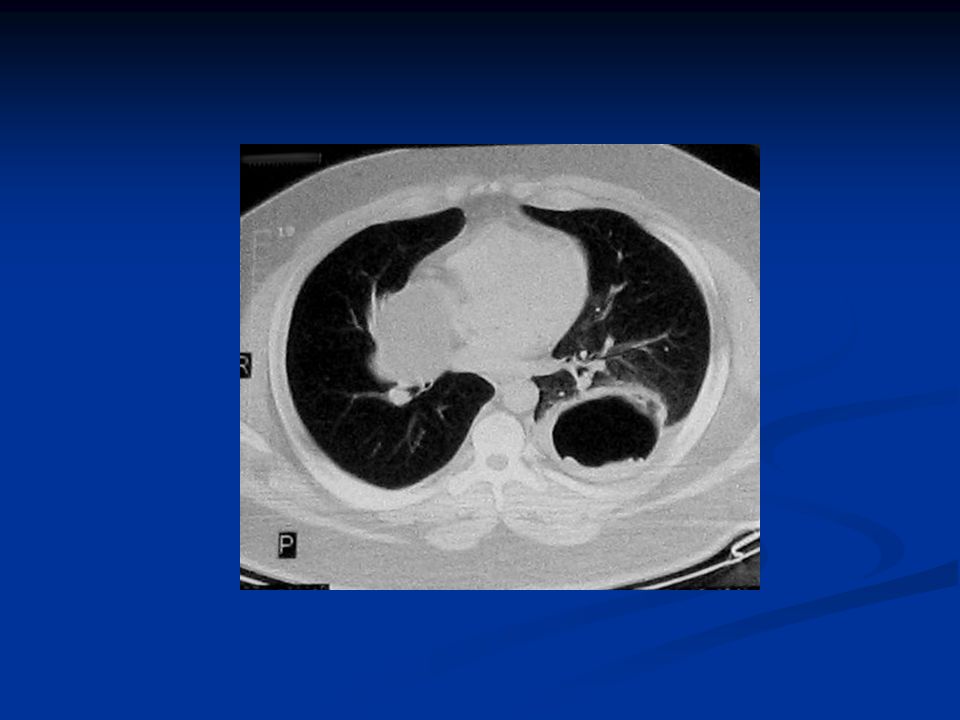
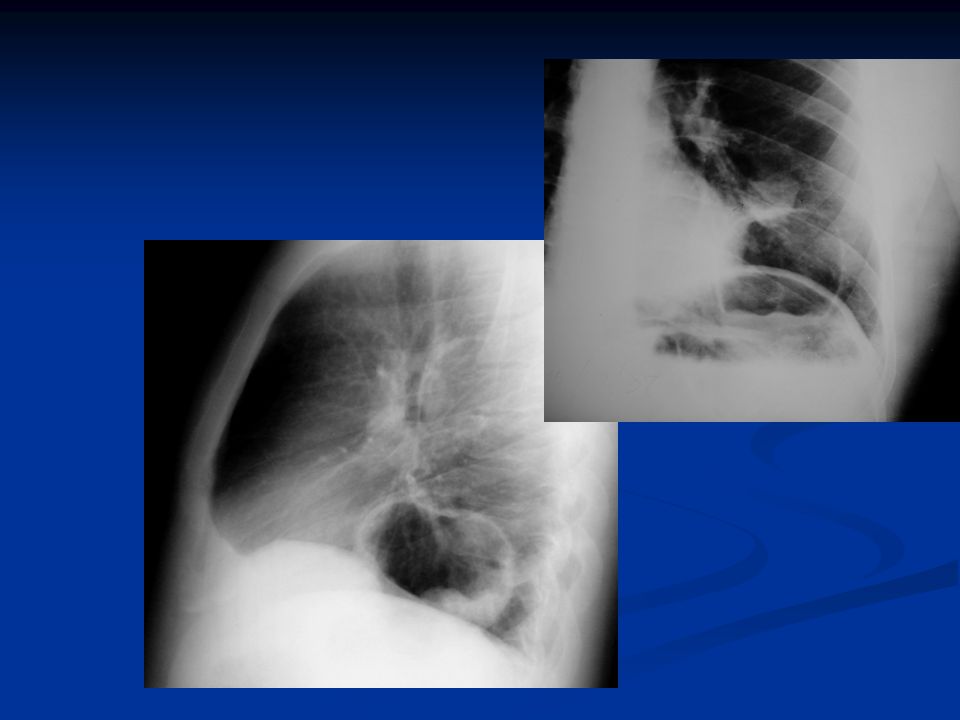
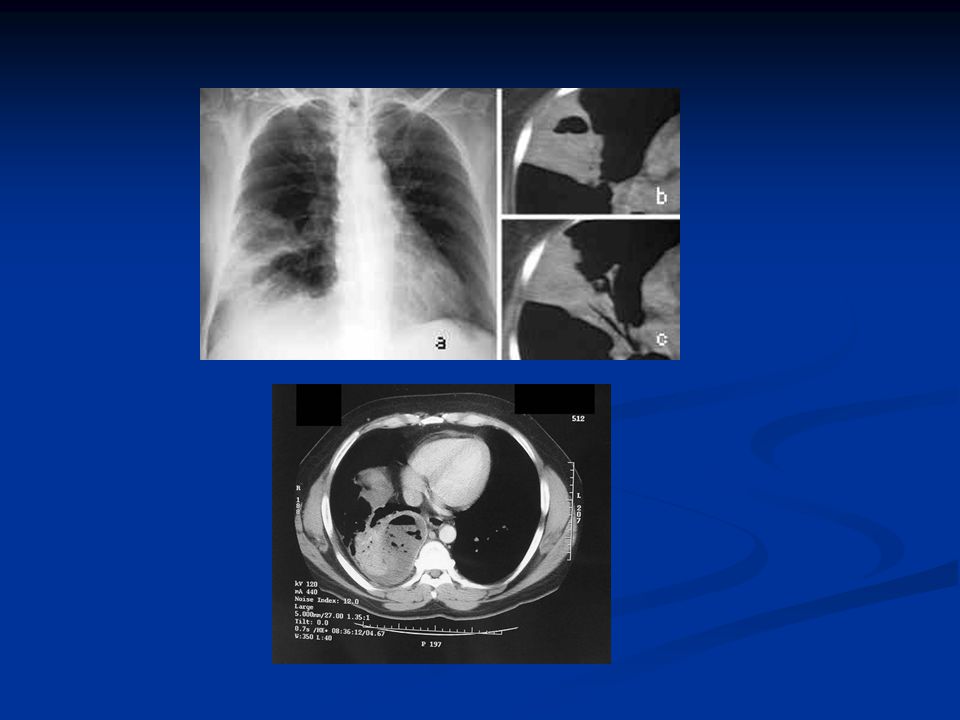
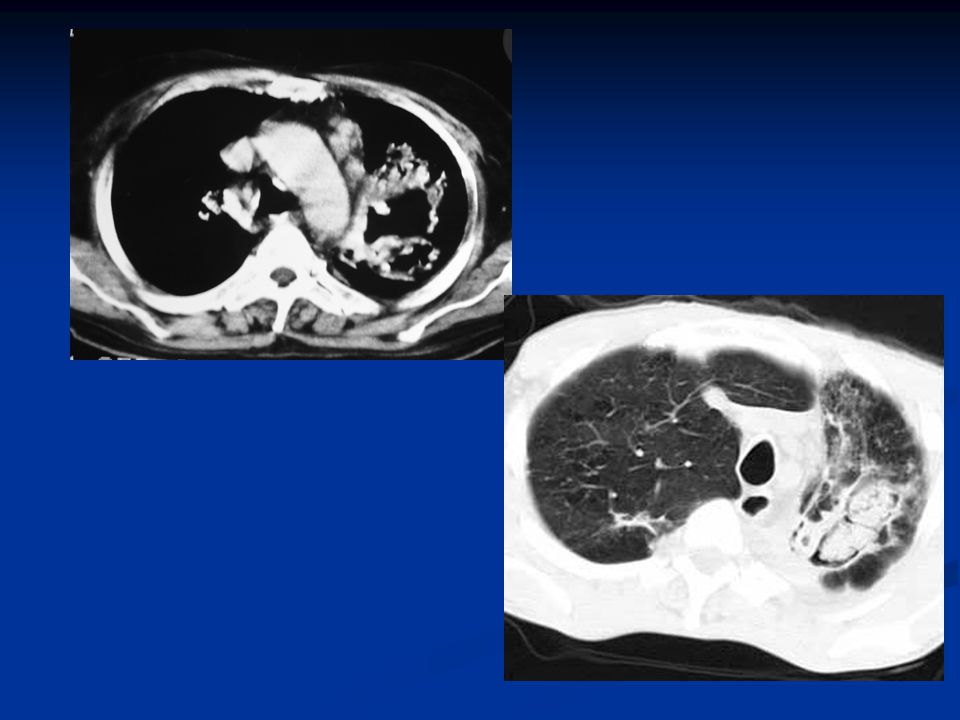
Hydatid disease * endemic in sheep-raising areas of Mediterranean basin * solitary in 75%, multiple in 25% * water density * rare calcify * complications: rupture between layers of cyst—meniscus or halo sign ruptue into bronchus—water lilly sign rupture into pleura---hydropneumothorax

31
Focal holes in the lung Cyst Cavity * Congenital --- - Br. Cyst - CCAM
* Bleb * Bulla * Pneumatocele * Infection---hydatid -coccidioidomycosis -PCP Cavity * neoplastic –Br. Ca - metastasis - lymphoma * infection bacteria - fungal - parasites * immunologic - wegener’s gr. - Rh. nodules * septic emboli * bronchiectasis

32
Focal cavitary lung lesions
* neoplastic – - Br. Ca - metastasis - lymphoma * infection bacteria - fungal - parasites * immunologic wegener’s gr. - Rh. nodules * septic emboli * bronchiectasis

33
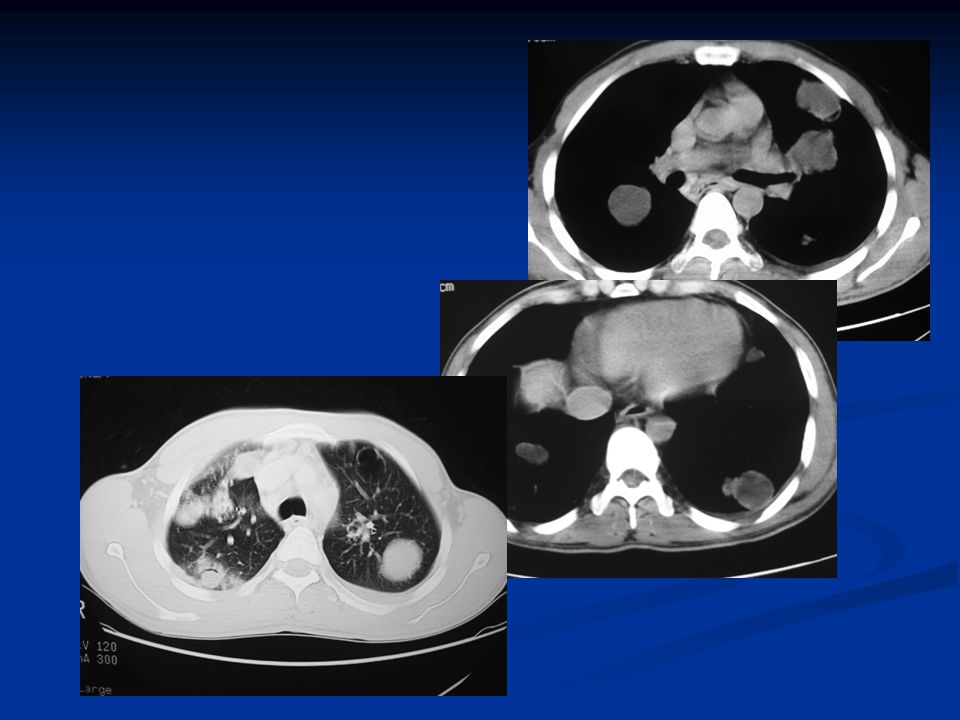
Neoplastic lesions Bronchogenic carcinoma Lymphoma Metastasis

34
Bronchogenic carcinoma (squamous cell type)
")
35
Squamous cell carcinoma

37
Infection * bacterial * fungal * parasites

40
Immunologic * Wegener’s granuloma * Rheumatoid nodules

41
Septic emboli Significant febrile illness
Multifocal, peripheral location Increase incidence of cavitation

42
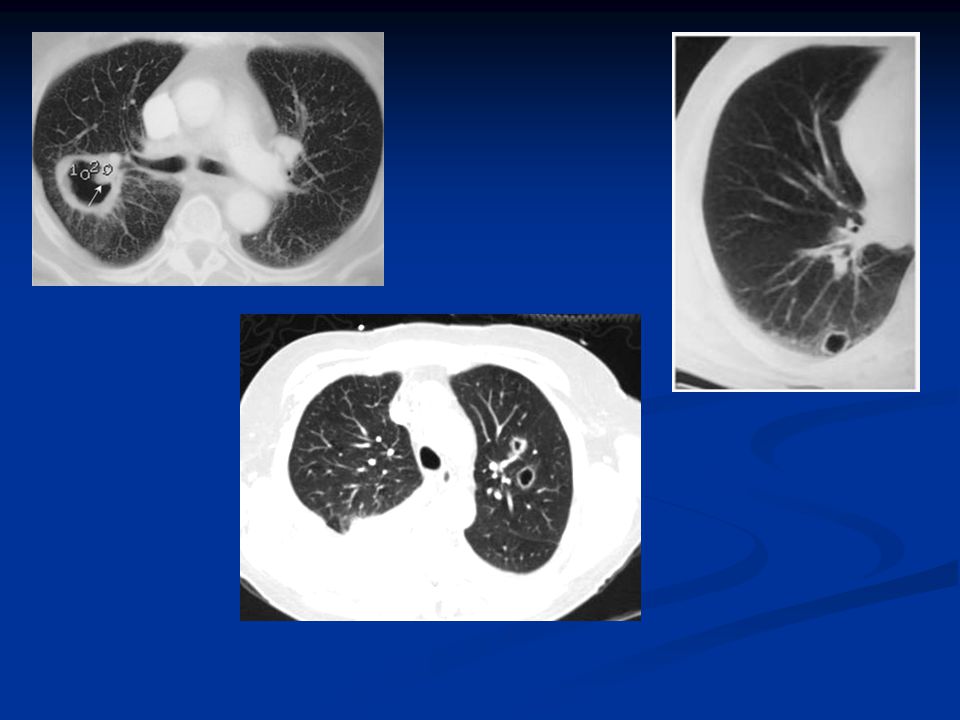
Bronchiectasis Cystic structures continuous with broncheal tree.
Signet ring sign

43
Cavity We have to look at: * wall thickness * contents ------- air
air-fluid level air with soft tissue mass. * relation to broncheal tree

44
Wall thickness : more than 4 mm
Contents * only air : regularity of the inner margin - if regular……chronic lung abscess - if irregular ….cavitating tumor * air-fluid level: - if fluid level is straight…acute lung abscess - if fluid level is wavy ….ruptured hydatid cyst * contents of the cavity -if inner wall is smooth with soft tissue inside….mycetoma -if inner wall is irregular with soft tissue mass..necrotic tumor

45
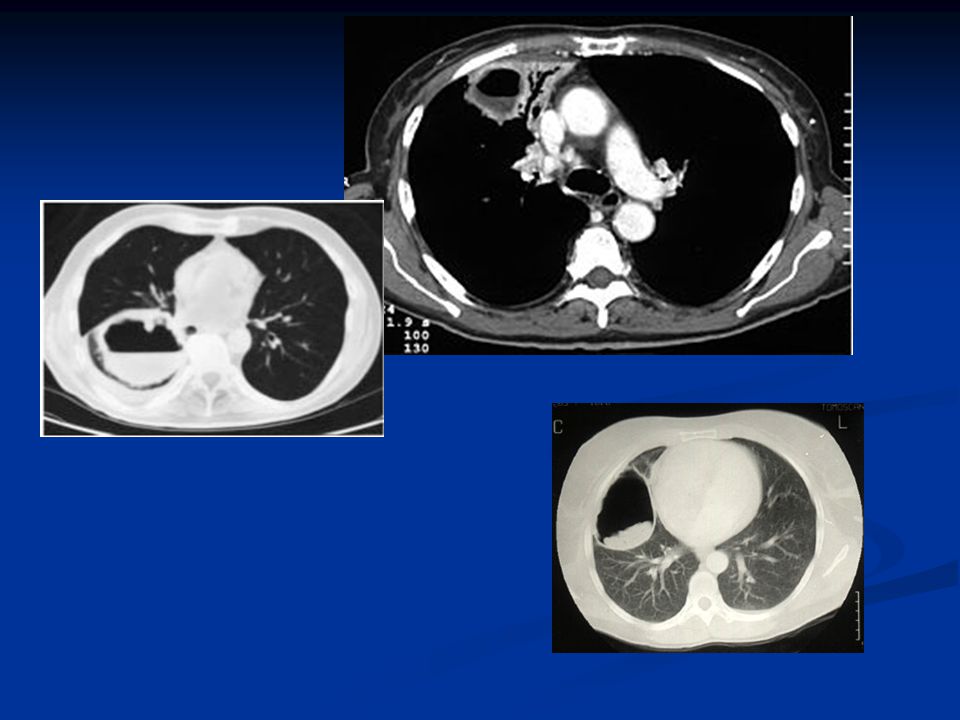
Cavity containing only air
* regularity of inner margin - if regular ---ch. Lung abscess - if irregular---cavitating tumor

46
Cavity with air-fluid level
- if fluid level is straight--- ----- acute lung abscess - if fluid level is wavy ----- -----ruptured hydatid cyst

47
Cavity with mass inside
- if inner wall is smooth--- mycetoma - if inner wall is nodular – necrotic tumor

49
Abscess vs hydatid

50
Hydatid vs abscess vs necrotic tumor

53
Focal holes in the lung Cyst Cavity * Congenital --- - Br. Cyst - CCAM
* Bleb * Bulla * Pneumatocele * Infection---hydatid -coccidioidomycosis -PCP Cavity * neoplastic –Br. Ca - metastasis - lymphoma * infection bacteria - fungal - parasites * immunologic - wegener’s gr. - Rh. nodules * septic emboli * bronchiectasis

54
Diffuse holes in the lung
Lymphangioleiomyomatosis Tuberous sclerosis L.C.Histiocytosis Honeycombing disease Emphysema

55
Lymphangioleiomyomatosis (LAM )
Proliferation of smooth muscles in lung interstitium Hyperinflated lung Widespread thin wall cysts No nodules Diffuse lung involvement Complicated by pneumothorax (40%) & chylothothorax (60%) Only in females All patients die within 10 years.
 & chylothothorax (60%) Only in females. All patients die within 10 years.")
59
Tuberous sclerosis * autosomal dominant
* pulmonary changes seen almost exclusively only in females in 3rd-4th decades * changes similar to LAM except chylous effusion

60
L.C.Histeocytosis Histeocytes proliferation Widespread cyts & nodules
Cysts are irregular in shapes (bizzare, bilobed, leaf like ), more numerous in apices, sparing costo-pherenic angles Lung volume is preserved >90% Smokers, middle age , men Spontaneous pneumothorax in 15%
, more numerous in apices, sparing costo-pherenic angles. Lung volume is preserved. >90% Smokers, middle age , men. Spontaneous pneumothorax in 15%")
62
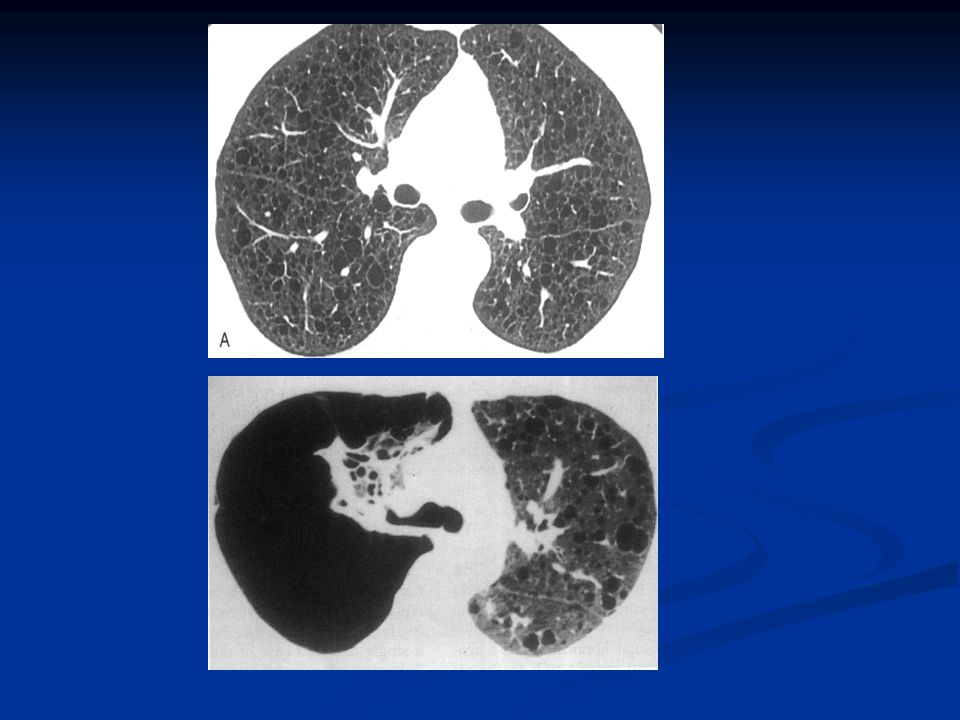
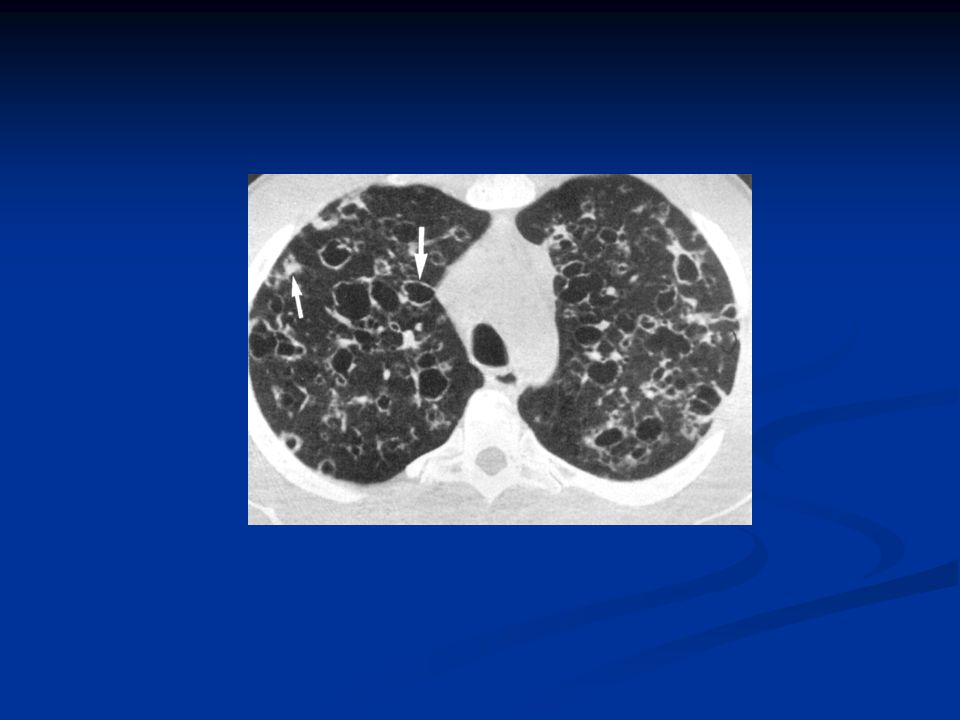
Honeycombing disease Indicates “end stage “ lung and can be seen in any process leading to severe pulmonary fibrosis Adjacent small cysts , 1-3 mm, typically share walls Predominate in lower lobes, peripheral & subpleural lung regions Typically occur in several contiguous layers

63
60% due IPF Other causes: - autoimmune disease like scleroderma & RA - hypersensitivity pneumonitis - drug reactions - asbestosis

65
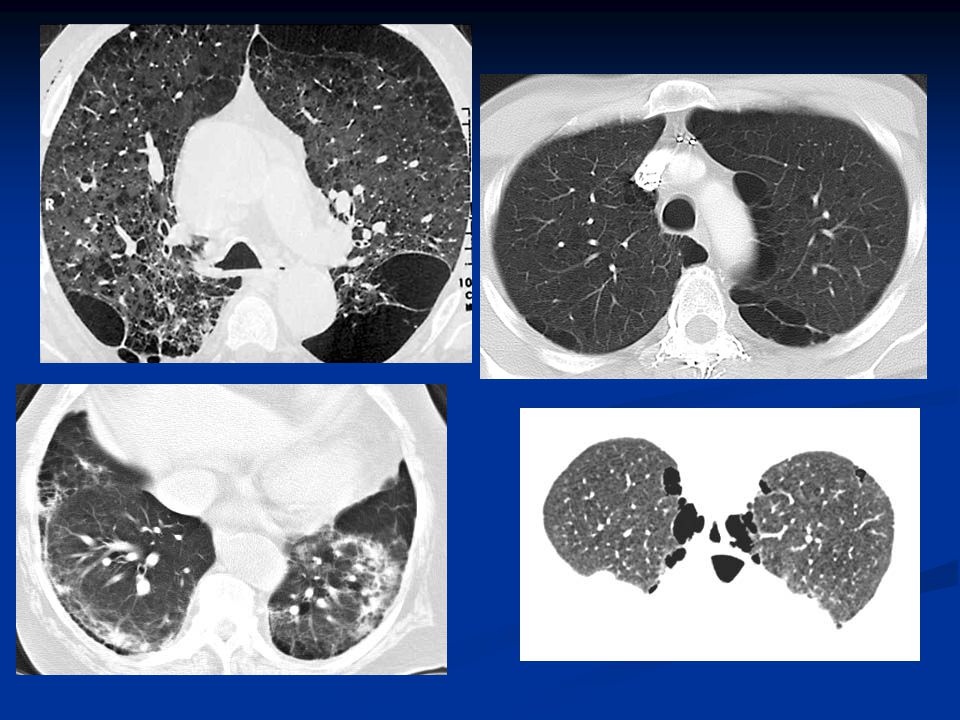
Emphysema Perminant, abnormal,enlargement of airspaces distal to the terminal bronchioles, accompanied by destruction of walls of the involved airspaces 3 types: - centrilobular emphysema - panlobular emphysema - paraseptal emphysema

66
Centrilobular emphysema
The more commoner Usually results from cigarette smoking Mainly involves upper lobes Multiple, small, lucencies, lack visible walls centrilobular distributd (grouped near the center of 2ry pulmonary lobules), surrounding the centrilobular artery
, surrounding the centrilobular artery.")
69
Panlolobular ( panacinar) emphysema
Uniform destruction of pulmonary lobule diffuse or more severe in lower lung Pulmonary vessels in affected lung appear smaller and fewer than normal No focal lucincies can be seen

70
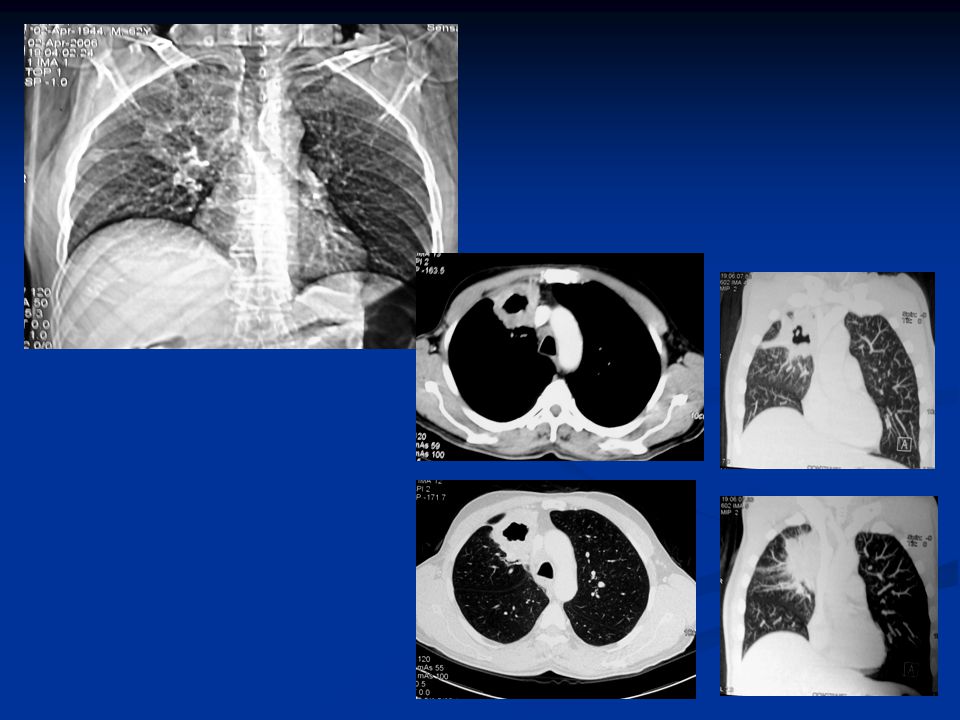
Paraseptal emphysema More stricking in subpleural location, arranged in single layer Often have visible very thin walls Can be an isolated phenomenon Can be associated with centrilobular emphysema When larger than 1cm , are termed as bulla

71
Paraseptal emphysema, Centrilobular emphysema and bulla can coexist together while panlobular emphysema is usually not associated with paraseptal emphysema or bulla .

73
Paraseptal emphysema vs honeycombing

74
Conclusion

75
Holes in the lung Focal * cyst * cavity Diffuse
Lymphangioleiomyomatosis Tuberous sclerosis L.C.Histeocytosis Honeycombing disease Emphysema

76
Focal holes in the lung Cyst Cavity * Congenital --- - Br. Cyst - CCAM
* Bleb * Bulla * Pneumatocele * Infection---hydatid -coccidioidomycosis -PCP Cavity * neoplastic –Br. Ca - metastasis - lymphoma * infection bacteria - fungal - parasites * immunologic - wegener’s gr. - Rh. nodules * septic emboli * bronchiectasis

77
In cystic lesions, benign nature is often be assumed, while cavitary lesions usually suggest more aggressive pathology. Other forms of focal pulmonary cysts may be seen in adults outside these clinical sittings, and are of obscure origin but are thaught to be related to smoking.

78
Thank you

Similar presentations













 Infections (pneumonia, airways disease)>")







>")
disease TB Histoplasmosis Chicken box Sarcoidosis LCH Pneumoconiosis Alveolar microlithiasis Metastasis.>")









