Download presentation
Presentation is loading. Please wait.

1
Chronic obstructive pulmonary diseases (COPD)
By Dr. Abdelaty Shawky Assistant professor of pathology

2
COPD is a group of lung diseases characterized by increased resistance to air flow due to airway obstruction. Includes; 1. Chronic bronchitis. 2. Emphysema.

3
1. Chronic bronchitis

4
* Definition: persistent productive cough for at least 3 consecutive months in at least 2 consecutive years. * Causes: Chronic irritation of the bronchial mucosa by: Cigarette smoking. Environmental pollution. Chronic inflammation of upper respiratory tract.

5
* Pathogenesis: Chronic irritation of the bronchial epithelium by cigarette smoke, environmental chemical…etc leads to: a. Epithelial changes: Hyperplasia, squamous metaplasia and dysplasia. b. Subepithelial changes: Hyperplasia of the mucous glands (increase mucin secretion) Hypertrophy of smooth muscle (leading to bronchial spasm). In old standing cases, marked fibrosis.
 Hypertrophy of smooth muscle (leading to bronchial spasm). In old standing cases, marked fibrosis.")
6
* Microscopic examination: Bronchi & bronchioles show:
* Gross features: The mucosa is hyperaemic, swollen and covered by mucus or muco-pus. * Microscopic examination: Bronchi & bronchioles show: Epithelial changes: Hyperplasia, squamous metaplasia and dysplasia. b. Subepithelial changes: Hyperplasia of the mucous glands, Chronic inflammatory cells and fibrosis. Hypertrophy of the smooth muscle.

7
* Clinical types of chronic bronchitis:
1. Simple chronic bronchitis: patients have a productive cough but no physiologic evidence of airflow obstruction. 2. Asthmatic chronic bronchitis: in individuals demonstrating hyper-reactive airways with intermittent bronchospasm and wheezing. 3. Obstructive chronic bronchitis: in some patients, especially heavy smokers, who develop evidence of associated emphysema.

8
* Complications: 1.Emphysema. 2.Bronchopneumonia. 3.Pulomonary hypertension and core pulmonale resulting in Rt. sided heart failure. 4.Bronchogenic carcinoma

9
2. Emphysema

10
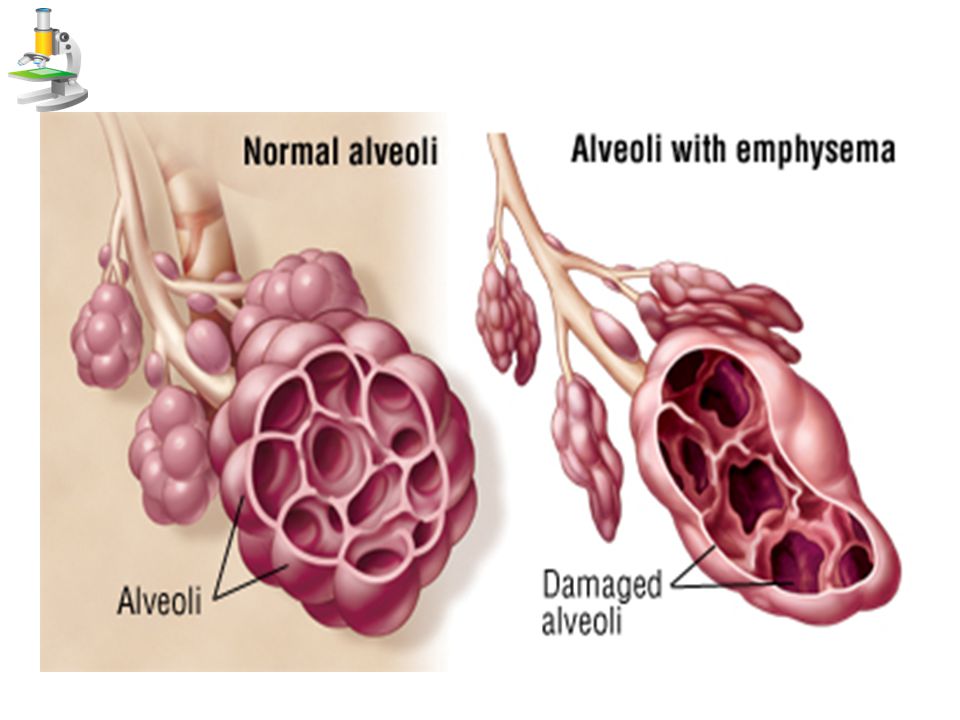
* Definition: Permanent dilatation of air spaces distal to the terminal bronchioles accompanied by damage of their walls without obvious fibrosis.

11
Respiratory acinus = Respiratory bronchioles + alveolar ducts + alveolar sacs.

12
* Types Centriacinar (centrilobular) emphysema.
Panacinar (panlobular) emphysema.
 emphysema.")
15
the whole respiratory acinus (RB+AD+alveoli)
Panacinar (panlobular) emphysema Centriacinar (centrilobular) emphysema 1. Site of involvement the whole respiratory acinus (RB+AD+alveoli) Central part of the respiratory acinus (respiratory bronchiole)
 emphysema. Centriacinar (centrilobular) emphysema. 1. Site of involvement. the whole respiratory acinus. (RB+AD+alveoli) Central part of the respiratory acinus (respiratory bronchiole)")
16
2. Pathogenesis Panacinar (panlobular) emphysema
Centriacinar (centrilobular) emphysema 2. Pathogenesis - Rare (5% of cases). - Affects young ages. - Related to congenital deficiency of anti-elastase (congenital α 1 antitrypsin deficiency). Therefore the action of elastase secreted from neutrophils and macrophages becomes unopposed. - Common (95% of cases). - Affects middle and old ages. - Related to cigarette smoking, explained by; 1. Elastase-antielastase imbalance theory: Smoking weaken the wall of air spaces by increasing elastase and decreasing antielastase via; 1. Accumulation of macrophages and neutrophils in the walls of air spaces which are the source of elastase enzyme. 2. Inhibit anti-elastase (α 1 antitrypsin) by oxidants (oxygen free radicals) secreted from neutrophils.
 emphysema. 2. Pathogenesis. - Rare (5% of cases). - Affects young ages. - Related to congenital deficiency of anti-elastase (congenital α 1 antitrypsin deficiency). Therefore the action of elastase secreted from neutrophils and macrophages becomes unopposed. - Common (95% of cases). - Affects middle and old ages. - Related to cigarette smoking, explained by; 1. Elastase-antielastase imbalance theory: Smoking weaken the wall of air spaces by increasing elastase and decreasing antielastase via; 1. Accumulation of macrophages and neutrophils in the walls of air spaces which are the source of elastase enzyme. 2. Inhibit anti-elastase (α 1 antitrypsin) by oxidants (oxygen free radicals) secreted from neutrophils.")
17
Panacinar (panlobular) emphysema
Centriacinar (centrilobular) emphysema 2. Chronic bronchitis theory: - It causes emphysema by: Accumulation of macrophages and neutrophils in the walls of air spaces with release of elastase. Bronchial obstruction by the mucous plugs leads to increased intraluminal pressure.
 emphysema. 2. Chronic bronchitis theory: - It causes emphysema by: Accumulation of macrophages and neutrophils in the walls of air spaces with release of elastase. Bronchial obstruction by the mucous plugs leads to increased intraluminal pressure.")
18
3. Gross features Panacinar (panlobular) emphysema
Centriacinar (centrilobular) emphysema 3. Gross features 1. Chest: Barrel-shaped chest: Increased antero-posterior diameter. Horizontal ribs. Wide subcostal angle. 2. Lungs: Lower lobes of the lungs are first affected. Markedly enlarged lungs. Very light. Pale. (due to vascular compression). Dry. Upper lobes are first affected. Moderate lung enlargement. C/S: clusters of dilated air spaces.
 emphysema. 3. Gross features. 1. Chest: Barrel-shaped chest: Increased antero-posterior diameter. Horizontal ribs. Wide subcostal angle. 2. Lungs: Lower lobes of the lungs are first affected. Markedly enlarged lungs. Very light. Pale. (due to vascular compression). Dry. Upper lobes are first affected. Moderate lung enlargement. C/S: clusters of dilated air spaces.")
19
Panacinar (panlobular) emphysema
Centriacinar (centrilobular) emphysema Consistency: feathery and pit on pressure. (due to loss of elastic tissue) Smooth outer surface with evident rib markings. Emphysematous bullae: coalescent wide air spaces along weak borders e.g. apex, anterior margin and free edge of the base). C/S: diffuse areas of large air spaces.
 emphysema. Consistency: feathery and pit on pressure. (due to loss of elastic tissue) Smooth outer surface with evident rib markings. Emphysematous bullae: coalescent wide air spaces along weak borders e.g. apex, anterior margin and free edge of the base). C/S: diffuse areas of large air spaces.")
20
Centriacinar emphysema

21
Panacinar emphysema

22
Emphysematous bollus

23
4. Microscopic Picture Panacinar (panlobular) emphysema
Centriacinar (centrilobular) emphysema 4. Microscopic Picture 1. Alveoli are: - Few in number, increased in size, distorted in shape. - Some alveolar septa rupture and the alveolar lumens coalesce to each other. 2. Alveolar walls are: thin with compressed capillaries and arterioles. Dilated respiratory bronchioles only with normal alveolar ducts and alveoli.
 emphysema. 4. Microscopic Picture. 1. Alveoli are: - Few in number, increased in size, distorted in shape. - Some alveolar septa rupture and the alveolar lumens coalesce to each other. 2. Alveolar walls are: thin with compressed capillaries and arterioles. Dilated respiratory bronchioles only with normal alveolar ducts and alveoli.")
24
II. C.V.S: Pulmonary hypertension & Rt. sided heart failure.
Panacinar (panlobular) emphysema Centriacinar (centrilobular) emphysema 5. Complications I. Respiratory system: Chronic bronchitis. Air embolism. Spontaneous pneumothorax (due to rupture of emphysematous bulla). Respiratory failure. II. C.V.S: Pulmonary hypertension & Rt. sided heart failure.
 emphysema. Centriacinar (centrilobular) emphysema. 5. Complications. I. Respiratory system: Chronic bronchitis. Air embolism. Spontaneous pneumothorax (due to rupture of emphysematous bulla). Respiratory failure. II. C.V.S: Pulmonary hypertension & Rt. sided heart failure.")
25
The end

Similar presentations









>")

Asthma 2)COPD 3)Comparison.>")



>")

 With atria and blood vessels on for.>")


