Download presentation
Presentation is loading. Please wait.

1
HRCT of Common Lung Diseases W. Richard Webb MD

2
Common Lung Diseases: HRCT Infections (pneumonia, airways disease) Infections (pneumonia, airways disease) Sarcoidosis Sarcoidosis Hypersensitivity pneumonitis Hypersensitivity pneumonitis UIP and idiopathic pulmonary fibrosis (IPF) UIP and idiopathic pulmonary fibrosis (IPF) Nonspecific interstitial pneumonia (NSIP) Nonspecific interstitial pneumonia (NSIP) Organizing pneumonia (OP or BOOP) Organizing pneumonia (OP or BOOP) Infections (pneumonia, airways disease) Infections (pneumonia, airways disease) Sarcoidosis Sarcoidosis Hypersensitivity pneumonitis Hypersensitivity pneumonitis UIP and idiopathic pulmonary fibrosis (IPF) UIP and idiopathic pulmonary fibrosis (IPF) Nonspecific interstitial pneumonia (NSIP) Nonspecific interstitial pneumonia (NSIP) Organizing pneumonia (OP or BOOP) Organizing pneumonia (OP or BOOP)
 Infections (pneumonia, airways disease) Sarcoidosis Sarcoidosis Hypersensitivity pneumonitis Hypersensitivity pneumonitis UIP and idiopathic pulmonary fibrosis (IPF) UIP and idiopathic pulmonary fibrosis (IPF) Nonspecific interstitial pneumonia (NSIP) Nonspecific interstitial pneumonia (NSIP) Organizing pneumonia (OP or BOOP) Organizing pneumonia (OP or BOOP) Infections (pneumonia, airways disease) Infections (pneumonia, airways disease) Sarcoidosis Sarcoidosis Hypersensitivity pneumonitis Hypersensitivity pneumonitis UIP and idiopathic pulmonary fibrosis (IPF) UIP and idiopathic pulmonary fibrosis (IPF) Nonspecific interstitial pneumonia (NSIP) Nonspecific interstitial pneumonia (NSIP) Organizing pneumonia (OP or BOOP) Organizing pneumonia (OP or BOOP)")
3
SarcoidosisSarcoidosis microscopic noncaseating granulomas in clusters microscopic noncaseating granulomas in clusters 60-70% have characteristic plain film findings 60-70% have characteristic plain film findings 10% have normal chest radiographs 10% have normal chest radiographs HRCT abnormal in most with normal radiographs HRCT abnormal in most with normal radiographs microscopic noncaseating granulomas in clusters microscopic noncaseating granulomas in clusters 60-70% have characteristic plain film findings 60-70% have characteristic plain film findings 10% have normal chest radiographs 10% have normal chest radiographs HRCT abnormal in most with normal radiographs HRCT abnormal in most with normal radiographs

4
small nodules, usually well-defined are typical small nodules, usually well-defined are typical patchy distribution patchy distribution upper lobe predominance in most upper lobe predominance in most the nodules show a perilymphatic distribution the nodules show a perilymphatic distribution typical lymph node enlargement or calcification in some patients is suggestive, but is not necessary for diagnosis typical lymph node enlargement or calcification in some patients is suggestive, but is not necessary for diagnosis small nodules, usually well-defined are typical small nodules, usually well-defined are typical patchy distribution patchy distribution upper lobe predominance in most upper lobe predominance in most the nodules show a perilymphatic distribution the nodules show a perilymphatic distribution typical lymph node enlargement or calcification in some patients is suggestive, but is not necessary for diagnosis typical lymph node enlargement or calcification in some patients is suggestive, but is not necessary for diagnosis Sarcoidosis: HRCT findings

5
perilymphatic nodules predominate in relation to the peripheral pleural surfaces and fissures, and the peribronchovascular interstitium perilymphatic nodules predominate in relation to the peripheral pleural surfaces and fissures, and the peribronchovascular interstitium interlobular septal nodules are less frequent and less numerous interlobular septal nodules are less frequent and less numerous centrilobular nodules can be seen involving the centrilobular peribronchovascular interstitium centrilobular nodules can be seen involving the centrilobular peribronchovascular interstitium in rare patients, the nodules appear random in distribution in rare patients, the nodules appear random in distribution perilymphatic nodules predominate in relation to the peripheral pleural surfaces and fissures, and the peribronchovascular interstitium perilymphatic nodules predominate in relation to the peripheral pleural surfaces and fissures, and the peribronchovascular interstitium interlobular septal nodules are less frequent and less numerous interlobular septal nodules are less frequent and less numerous centrilobular nodules can be seen involving the centrilobular peribronchovascular interstitium centrilobular nodules can be seen involving the centrilobular peribronchovascular interstitium in rare patients, the nodules appear random in distribution in rare patients, the nodules appear random in distribution Sarcoidosis: Nodules

6
Sarcoidosis Subpleural and peribronchovascular nodules

7
. Perilymphatic nodules in sarcoidosis: peribronchovascular and subpleural

8
. Perilymphatic nodules in sarcoidosis: peribronchovascular and subpleural

10
. Perilymphatic nodules in sarcoidosis: peribronchovascular and subpleural

11
. Perilymphatic nodules in sarcoidosis: peribronchovascular and subpleural

12
Sarcoidosis: interlobular septal nodules.

13
. Sarcoidosis with interlobular septal nodules

14
interlobular septal nodules with atypical basal distribution.

16
. Centrilobular (peribronchovascular) nodules
 nodules")
17
. Sarcoidosis: centrilobular opacities mimicking tree-in-bud

18
. Sarcoidosis: centrilobular opacities mimicking tree-in-bud

19
Sarcoidosis: centrilobular nodules

20
Sarcoidosis: centrilobular nodules

21
Sarcoidosis: centrilobular nodules

22
. Sarcoidosis: nodules with a random distribution

23
large nodules or masses - 15-25% large nodules or masses - 15-25% » often upper lobe, parahilar (peribronchovascular) » air bronchograms (i.e. consolidation) » confluence of granulomas » satellite nodules (galaxy sign) » alveolar sarcoid ground-glass opacity ground-glass opacity » confluence of small granulomas large nodules or masses - 15-25% large nodules or masses - 15-25% » often upper lobe, parahilar (peribronchovascular) » air bronchograms (i.e. consolidation) » confluence of granulomas » satellite nodules (galaxy sign) » alveolar sarcoid ground-glass opacity ground-glass opacity » confluence of small granulomas Sarcoidosis: additional findings
 » confluence of granulomas » satellite nodules (galaxy sign) » alveolar sarcoid ground-glass opacity ground-glass opacity » confluence of small granulomas large nodules or masses % large nodules or masses % » often upper lobe, parahilar (peribronchovascular) » air bronchograms (i.e. consolidation) » confluence of granulomas » satellite nodules (galaxy sign) » alveolar sarcoid ground-glass opacity ground-glass opacity » confluence of small granulomas Sarcoidosis: additional findings.")
24
Sarcoidosis: subpleural and peribronchovascular nodules confluent nodules: masses with satellites.

25
. Sarcoidosis: subpleural and peribronchovascular nodules confluent nodules: masses with satellites

26
. confluent nodules: masses with satellites the galaxy sign Sarcoidosis: subpleural and peribronchovascular nodules

27
. confluent nodules: masses with satellites

28
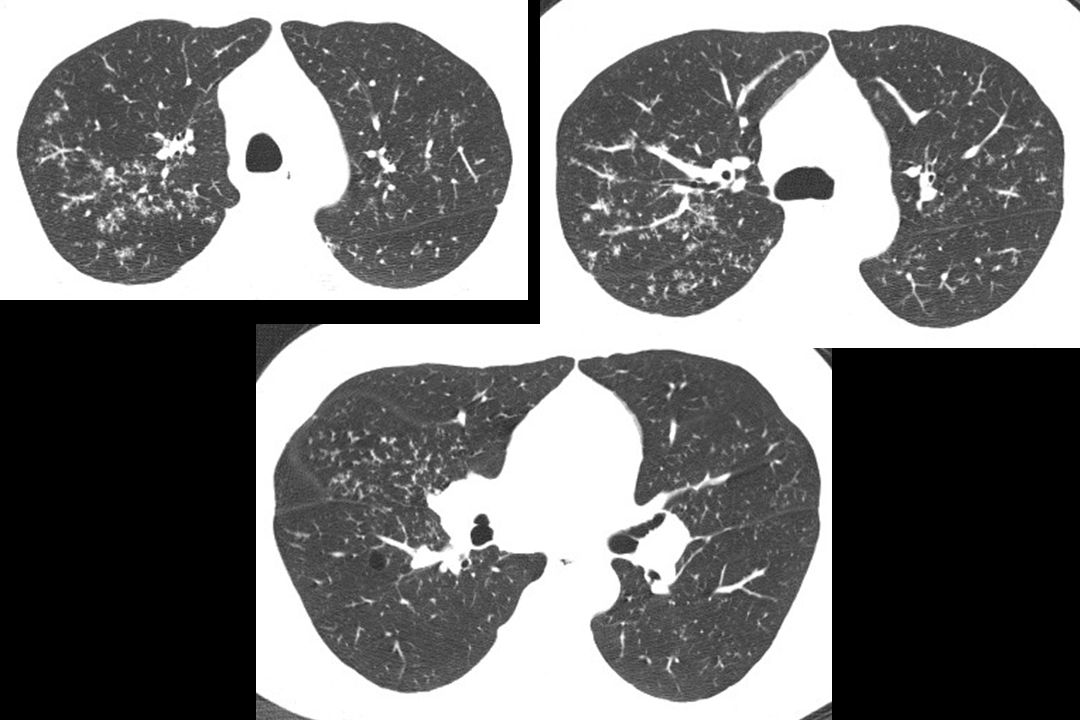
. Sarcoidosis: confluent nodules with air bronchograms

30
. Sarcoidosis: clustered small nodules with satellites and ground-glass opacity

31
Sarcoidosis: nodules and ground-glass opacity.

32
Sarcoidosis: ground-glass opacity.

33
obstruction of large airways obstruction of large airways endobronchial granulomas endobronchial granulomas small airway obstruction with mosaic perfusion and/or air trapping on expiratory scans small airway obstruction with mosaic perfusion and/or air trapping on expiratory scans obstruction of large airways obstruction of large airways endobronchial granulomas endobronchial granulomas small airway obstruction with mosaic perfusion and/or air trapping on expiratory scans small airway obstruction with mosaic perfusion and/or air trapping on expiratory scans Sarcoidosis: airway abnormalities

34
Sarcoid: airway abnormalities

35
45 year old with dyspnea bronch: sarcoidosis.

36
1 year later.

37
dynamic expiration Sarcoidosis: nodules and air trapping.

38
. Sarcoidosis: subpleural and peribronchovascular nodules

39
. dynamic expiration Sarcoidosis: air trapping inspiration

40
. dynamic expiration Sarcoidosis: air trapping

41
Sarcoidosis: late or fibrotic nodules decrease (but often remain visible) nodules decrease (but often remain visible) distortion of fissures, reticulation distortion of fissures, reticulation interlobular septal thickening interlobular septal thickening peribronchovascular fibrosis, usually upper lobe peribronchovascular fibrosis, usually upper lobe conglomerate masses of fibrous tissue conglomerate masses of fibrous tissue traction bronchiectasis traction bronchiectasis subpleural honeycombing in a few percent subpleural honeycombing in a few percent emphysema and cysts emphysema and cysts nodules decrease (but often remain visible) nodules decrease (but often remain visible) distortion of fissures, reticulation distortion of fissures, reticulation interlobular septal thickening interlobular septal thickening peribronchovascular fibrosis, usually upper lobe peribronchovascular fibrosis, usually upper lobe conglomerate masses of fibrous tissue conglomerate masses of fibrous tissue traction bronchiectasis traction bronchiectasis subpleural honeycombing in a few percent subpleural honeycombing in a few percent emphysema and cysts emphysema and cysts
 nodules decrease (but often remain visible) distortion of fissures, reticulation distortion of fissures, reticulation interlobular septal thickening interlobular septal thickening peribronchovascular fibrosis, usually upper lobe peribronchovascular fibrosis, usually upper lobe conglomerate masses of fibrous tissue conglomerate masses of fibrous tissue traction bronchiectasis traction bronchiectasis subpleural honeycombing in a few percent subpleural honeycombing in a few percent emphysema and cysts emphysema and cysts nodules decrease (but often remain visible) nodules decrease (but often remain visible) distortion of fissures, reticulation distortion of fissures, reticulation interlobular septal thickening interlobular septal thickening peribronchovascular fibrosis, usually upper lobe peribronchovascular fibrosis, usually upper lobe conglomerate masses of fibrous tissue conglomerate masses of fibrous tissue traction bronchiectasis traction bronchiectasis subpleural honeycombing in a few percent subpleural honeycombing in a few percent emphysema and cysts emphysema and cysts")
42
Sarcoidosis: early fibrosis with reticulation and distortion of fissures.

43
. Sarcoidosis: fibrosis with reticulation and septal thickening

44
Sarcoidosis: conglomerate fibrosis, traction bronchiectasis, posterior displacement of the hila.

45
. Complicated Silicosis peribronchovascular nodules and masses, satellite nodules

46
Sarcoidosis: fibrosis with traction bronchiectasis.

47
. Sarcoidosis: peribronchovascular fibrosis with traction bronchiectasis, mild honeycombing

48
Sarcoidosis: traction bronchiectasis and cysts.

49
.

50
. Sarcoidosis: fibrosis with cysts

51
. Sarcoidosis: traction bronchiectasis, cysts, emphysema, aspergilloma

52
Sarcoidosis: traction bronchiectasis and honeycombing.

53
Hypersensitivity Pneumonitis

54
Hypersensitivity Pneumonitis (HP) common common caused by inhalation of organic antigens caused by inhalation of organic antigens responsible antigen identified in only 50% responsible antigen identified in only 50% acute, subacute, and chronic stages acute, subacute, and chronic stages repeated exposures produce fever, chills, dry cough, dyspnea repeated exposures produce fever, chills, dry cough, dyspnea progressive symptoms over months or years progressive symptoms over months or years common common caused by inhalation of organic antigens caused by inhalation of organic antigens responsible antigen identified in only 50% responsible antigen identified in only 50% acute, subacute, and chronic stages acute, subacute, and chronic stages repeated exposures produce fever, chills, dry cough, dyspnea repeated exposures produce fever, chills, dry cough, dyspnea progressive symptoms over months or years progressive symptoms over months or years
 common common caused by inhalation of organic antigens caused by inhalation of organic antigens responsible antigen identified in only 50% responsible antigen identified in only 50% acute, subacute, and chronic stages acute, subacute, and chronic stages repeated exposures produce fever, chills, dry cough, dyspnea repeated exposures produce fever, chills, dry cough, dyspnea progressive symptoms over months or years progressive symptoms over months or years common common caused by inhalation of organic antigens caused by inhalation of organic antigens responsible antigen identified in only 50% responsible antigen identified in only 50% acute, subacute, and chronic stages acute, subacute, and chronic stages repeated exposures produce fever, chills, dry cough, dyspnea repeated exposures produce fever, chills, dry cough, dyspnea progressive symptoms over months or years progressive symptoms over months or years")
55
ongoing exposure ongoing exposure progressive symptoms over weeks to months progressive symptoms over weeks to months ill-defined peribronchiolar granulomas ill-defined peribronchiolar granulomas alveolitis and interstitial infiltration alveolitis and interstitial infiltration cellular bronchiolitis cellular bronchiolitis ongoing exposure ongoing exposure progressive symptoms over weeks to months progressive symptoms over weeks to months ill-defined peribronchiolar granulomas ill-defined peribronchiolar granulomas alveolitis and interstitial infiltration alveolitis and interstitial infiltration cellular bronchiolitis cellular bronchiolitis Hypersensitivity Pneumonitis: subacute stage

56
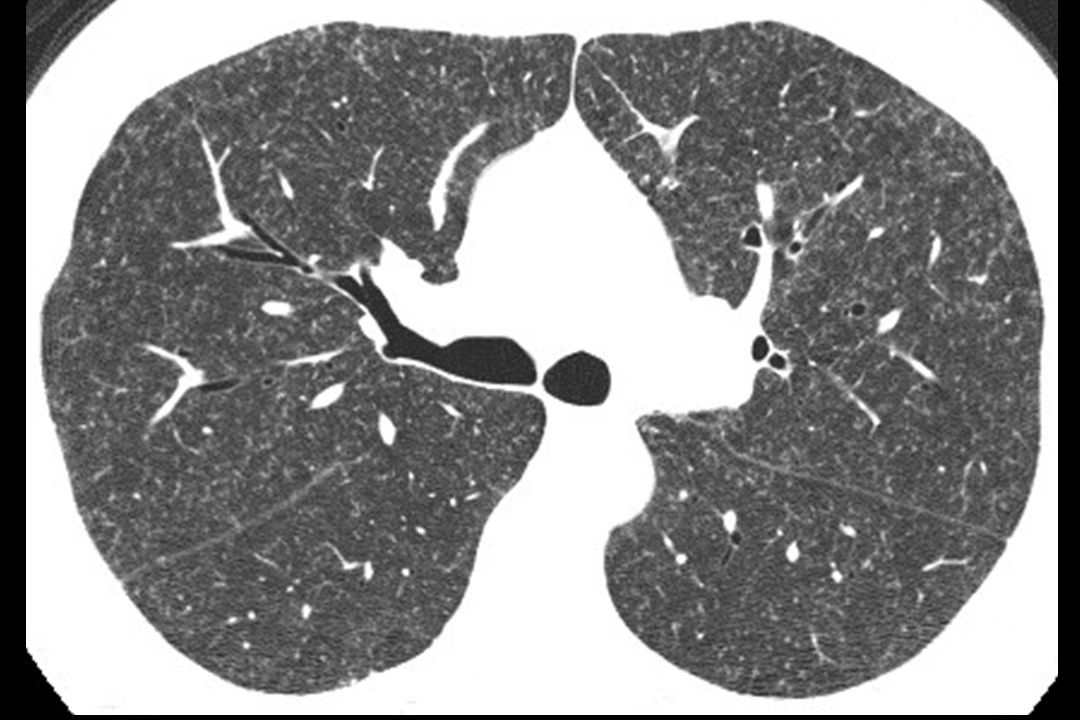
ill-defined centrilobular nodules (50-60%), usually of ground-glass opacity (granulomas) ill-defined centrilobular nodules (50-60%), usually of ground-glass opacity (granulomas) patchy ground-glass opacity (75-90%) (alveolitis) patchy ground-glass opacity (75-90%) (alveolitis) patchy mosaic perfusion; air trapping on expiratory scans (bronchiolitis) patchy mosaic perfusion; air trapping on expiratory scans (bronchiolitis) diffuse or predominant in mid lung zones; entire cross section of lung involved; no subpleural predominance diffuse or predominant in mid lung zones; entire cross section of lung involved; no subpleural predominance a few lung cysts in a few patients a few lung cysts in a few patients ill-defined centrilobular nodules (50-60%), usually of ground-glass opacity (granulomas) ill-defined centrilobular nodules (50-60%), usually of ground-glass opacity (granulomas) patchy ground-glass opacity (75-90%) (alveolitis) patchy ground-glass opacity (75-90%) (alveolitis) patchy mosaic perfusion; air trapping on expiratory scans (bronchiolitis) patchy mosaic perfusion; air trapping on expiratory scans (bronchiolitis) diffuse or predominant in mid lung zones; entire cross section of lung involved; no subpleural predominance diffuse or predominant in mid lung zones; entire cross section of lung involved; no subpleural predominance a few lung cysts in a few patients a few lung cysts in a few patients Hypersensitivity Pneumonitis: subacute stage
, usually of ground-glass opacity (granulomas) ill-defined centrilobular nodules (50-60%), usually of ground-glass opacity (granulomas) patchy ground-glass opacity (75-90%) (alveolitis) patchy ground-glass opacity (75-90%) (alveolitis) patchy mosaic perfusion; air trapping on expiratory scans (bronchiolitis) patchy mosaic perfusion; air trapping on expiratory scans (bronchiolitis) diffuse or predominant in mid lung zones; entire cross section of lung involved; no subpleural predominance diffuse or predominant in mid lung zones; entire cross section of lung involved; no subpleural predominance a few lung cysts in a few patients a few lung cysts in a few patients ill-defined centrilobular nodules (50-60%), usually of ground-glass opacity (granulomas) ill-defined centrilobular nodules (50-60%), usually of ground-glass opacity (granulomas) patchy ground-glass opacity (75-90%) (alveolitis) patchy ground-glass opacity (75-90%) (alveolitis) patchy mosaic perfusion; air trapping on expiratory scans (bronchiolitis) patchy mosaic perfusion; air trapping on expiratory scans (bronchiolitis) diffuse or predominant in mid lung zones; entire cross section of lung involved; no subpleural predominance diffuse or predominant in mid lung zones; entire cross section of lung involved; no subpleural predominance a few lung cysts in a few patients a few lung cysts in a few patients Hypersensitivity Pneumonitis: subacute stage")
57
. Subacute hypersensitivity pneumonitis

58
.

59
.

60
.

64
.

65
Subacute HP: patchy GGO

66
post-treatment Hypersensitivity pneumonitis ground-glass opacity.

67
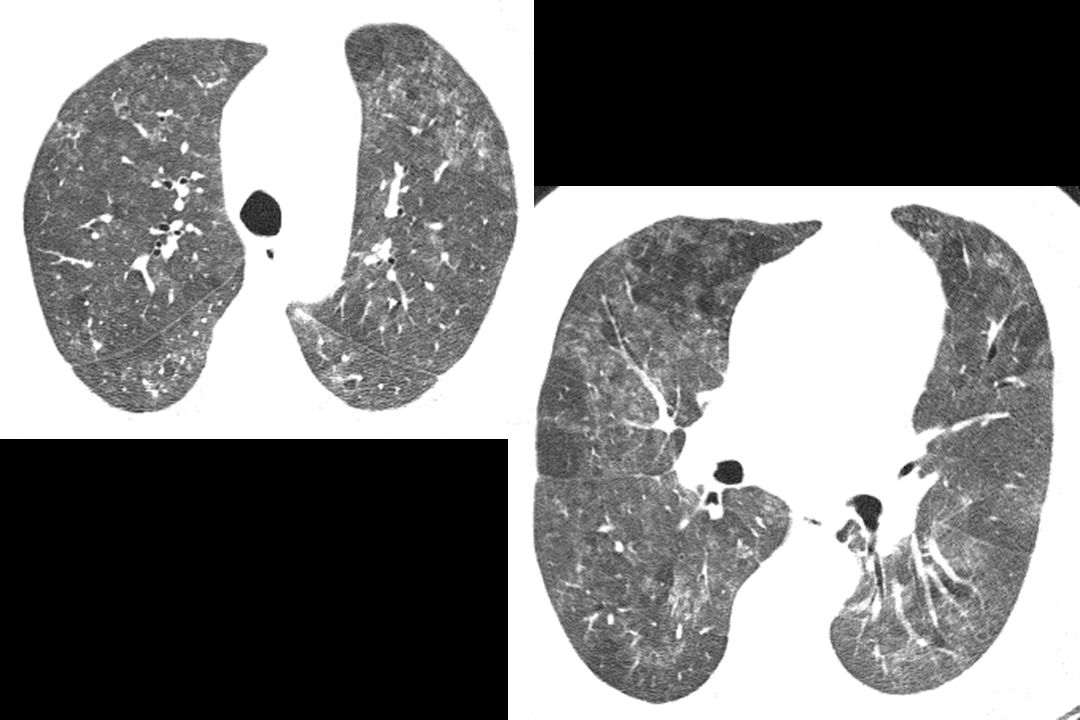
. ground-glass opacity + mosaic perfusion Headcheese sign ground-glass opacity = interstitial infiltration mosaic perfusion = bronchiolitis

68
headcheeseheadcheese headcheese - a jellied loaf or sausage containing chopped and boiled parts of the head, feet, tongue, and sometimes the heart of an animal, usually a hog headcheese - a jellied loaf or sausage containing chopped and boiled parts of the head, feet, tongue, and sometimes the heart of an animal, usually a hog it tastes like it looks it tastes like it looks headcheese - a jellied loaf or sausage containing chopped and boiled parts of the head, feet, tongue, and sometimes the heart of an animal, usually a hog headcheese - a jellied loaf or sausage containing chopped and boiled parts of the head, feet, tongue, and sometimes the heart of an animal, usually a hog it tastes like it looks it tastes like it looks

69
the headcheese sign Chung et al. JTI 2001; Webb. Radiology 2006 mixed attenuation with a geographic distribution - areas of increased, decreased, and normal opacity mixed attenuation with a geographic distribution - areas of increased, decreased, and normal opacity infiltrative dis with GGO, bronchiolitis with mosaic perfusion or air trapping infiltrative dis with GGO, bronchiolitis with mosaic perfusion or air trapping typical of HP typical of HP mixed attenuation with a geographic distribution - areas of increased, decreased, and normal opacity mixed attenuation with a geographic distribution - areas of increased, decreased, and normal opacity infiltrative dis with GGO, bronchiolitis with mosaic perfusion or air trapping infiltrative dis with GGO, bronchiolitis with mosaic perfusion or air trapping typical of HP typical of HP

70
headcheese headcheese sign

71
Hypersensitivity pneumonitis Headcheese sign.

72
lobular (geographic) ground-glass opacity and mosaic perfusion (air trapping) indicative of mixed infiltrative disease and bronchiolitis Headcheese sign Hypersensitivity Pneumonitis
 ground-glass opacity and mosaic perfusion (air trapping) indicative of mixed infiltrative disease and bronchiolitis Headcheese sign Hypersensitivity Pneumonitis")
75
mosaic perfusion.

76
expiration.

77
66 year old bird fancier with progressive dyspnea Hypersensitivity pneumonitis.

78
dynamic expiration.

79
Subacute HP: air trapping

80
. Biopsy proven HP

81
. expiratory scan

82
expiration Hypersensitivity pneumonitis air-trapping with lung cyst.

83
HRCT Diagnosis: Chronic HP, IPF, NSIP chronic HP: lobular areas of low attenuation, centrilobular ground-glass opacity nodules, absence of lower lobe predominance chronic HP: lobular areas of low attenuation, centrilobular ground-glass opacity nodules, absence of lower lobe predominance IPF: basal predominance of honeycombing, absence of subpleural sparing and nodules IPF: basal predominance of honeycombing, absence of subpleural sparing and nodules NSIP: subpleural sparing, absence of honeycombing and lobular low attenuation NSIP: subpleural sparing, absence of honeycombing and lobular low attenuation confident diagnosis in 53%; correct in 94% confident diagnosis in 53%; correct in 94% chronic HP: lobular areas of low attenuation, centrilobular ground-glass opacity nodules, absence of lower lobe predominance chronic HP: lobular areas of low attenuation, centrilobular ground-glass opacity nodules, absence of lower lobe predominance IPF: basal predominance of honeycombing, absence of subpleural sparing and nodules IPF: basal predominance of honeycombing, absence of subpleural sparing and nodules NSIP: subpleural sparing, absence of honeycombing and lobular low attenuation NSIP: subpleural sparing, absence of honeycombing and lobular low attenuation confident diagnosis in 53%; correct in 94% confident diagnosis in 53%; correct in 94% 288 Silva et al. Radiology 2008; 246:288

84
48 year old man with dyspnea

88
Hot tub lung

89
Immunocompetent subjects Immunocompetent subjects symptoms within hours of hot tub use symptoms within hours of hot tub use dyspnea, cough, hypoxemia, fever dyspnea, cough, hypoxemia, fever nonnecrotizing granulomas, often bronchiolocentric nonnecrotizing granulomas, often bronchiolocentric MAC (mycobactium avium) found on culture, less often on biopsy, and in the hot tube MAC (mycobactium avium) found on culture, less often on biopsy, and in the hot tube likely a hypersensitivity reaction likely a hypersensitivity reaction resolution without antibiotic treatment resolution without antibiotic treatment Immunocompetent subjects Immunocompetent subjects symptoms within hours of hot tub use symptoms within hours of hot tub use dyspnea, cough, hypoxemia, fever dyspnea, cough, hypoxemia, fever nonnecrotizing granulomas, often bronchiolocentric nonnecrotizing granulomas, often bronchiolocentric MAC (mycobactium avium) found on culture, less often on biopsy, and in the hot tube MAC (mycobactium avium) found on culture, less often on biopsy, and in the hot tube likely a hypersensitivity reaction likely a hypersensitivity reaction resolution without antibiotic treatment resolution without antibiotic treatment
 found on culture, less often on biopsy, and in the hot tube MAC (mycobactium avium) found on culture, less often on biopsy, and in the hot tube likely a hypersensitivity reaction likely a hypersensitivity reaction resolution without antibiotic treatment resolution without antibiotic treatment Immunocompetent subjects Immunocompetent subjects symptoms within hours of hot tub use symptoms within hours of hot tub use dyspnea, cough, hypoxemia, fever dyspnea, cough, hypoxemia, fever nonnecrotizing granulomas, often bronchiolocentric nonnecrotizing granulomas, often bronchiolocentric MAC (mycobactium avium) found on culture, less often on biopsy, and in the hot tube MAC (mycobactium avium) found on culture, less often on biopsy, and in the hot tube likely a hypersensitivity reaction likely a hypersensitivity reaction resolution without antibiotic treatment resolution without antibiotic treatment")
90
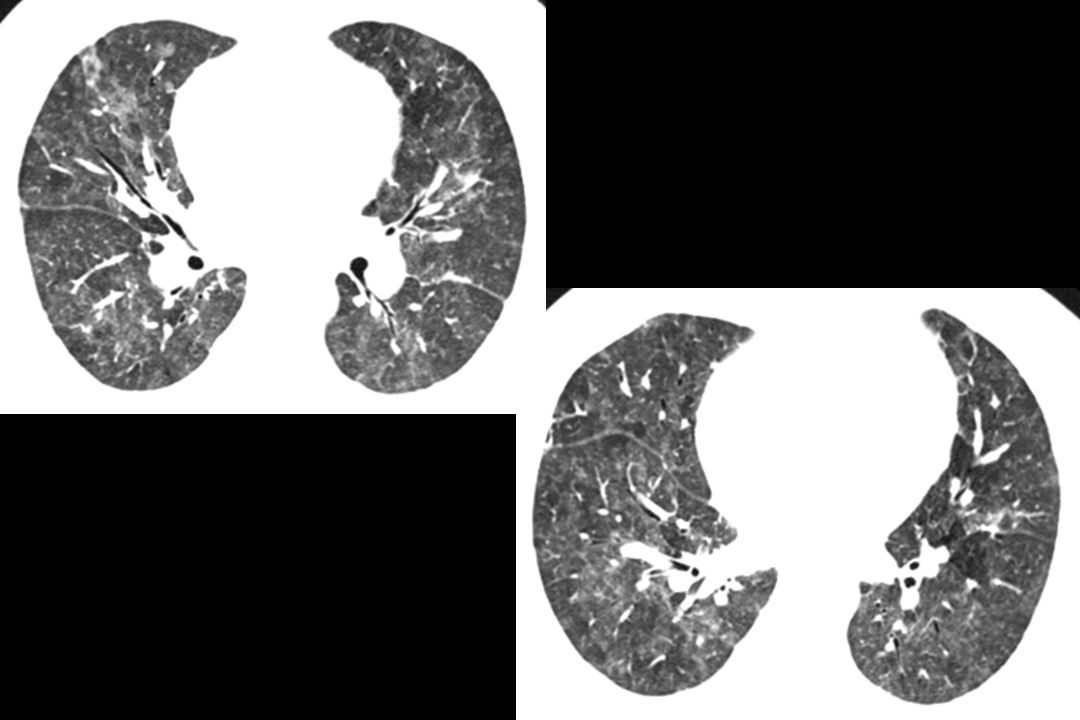
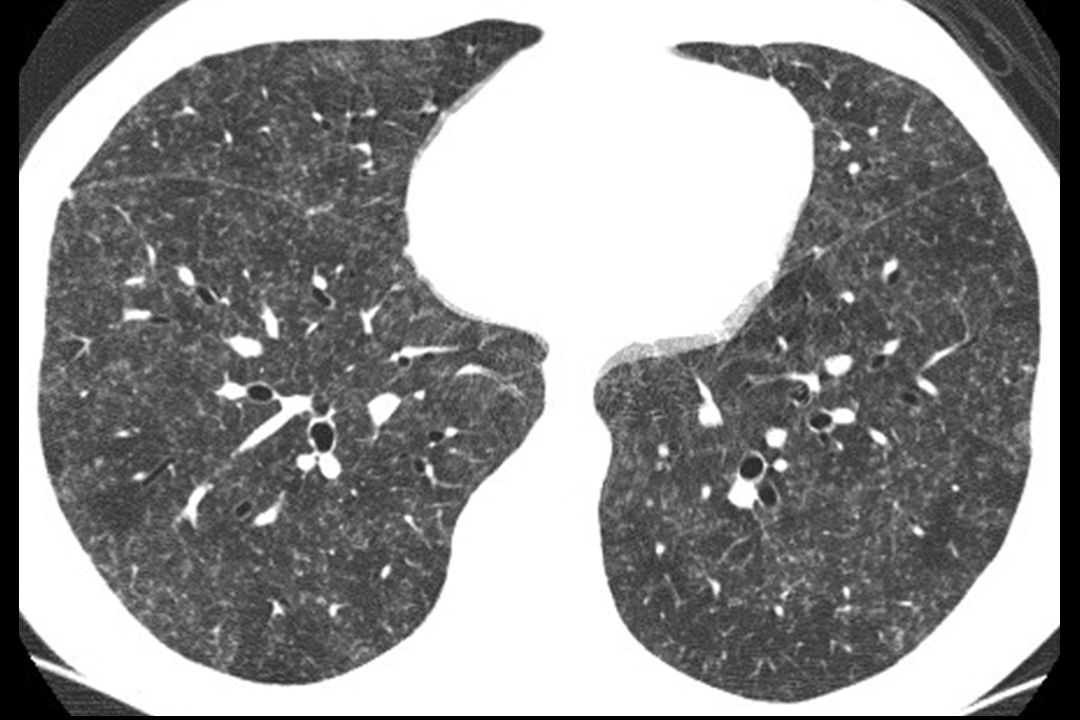
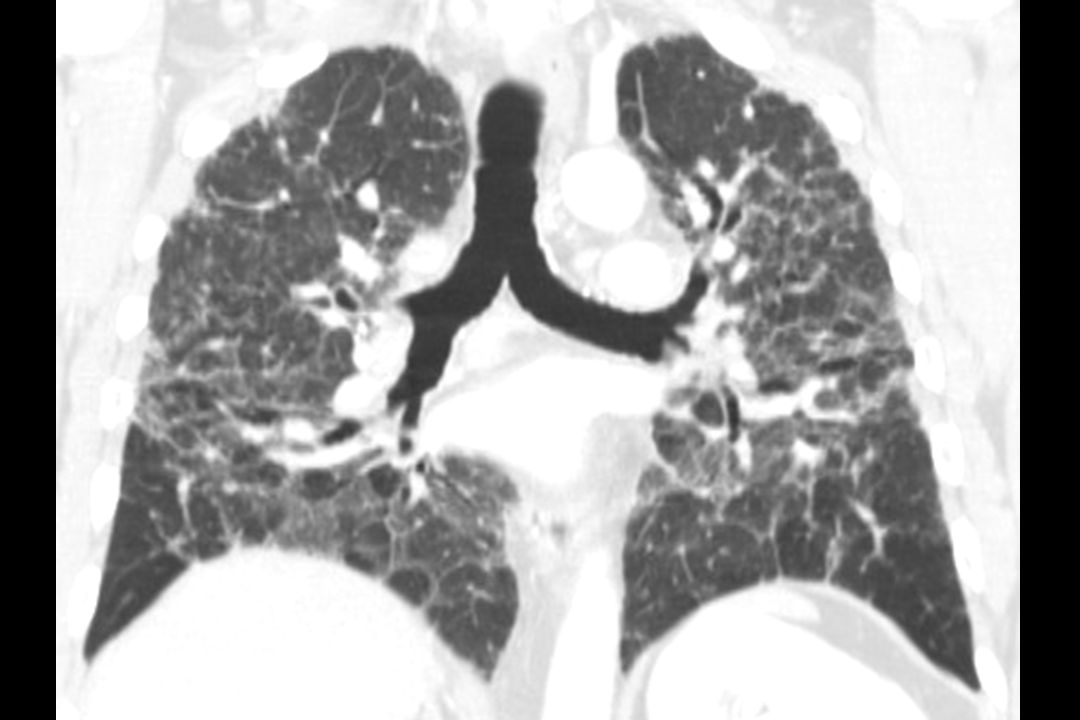
Hypersensitivity Pneumonitis: chronic stage long term or repeated exposure long term or repeated exposure irregular fibrosis: coarse scars, septal thickening, traction bronchiectasis, honeycombing in some irregular fibrosis: coarse scars, septal thickening, traction bronchiectasis, honeycombing in some patchy, lacks a subpleural distribution in most patchy, lacks a subpleural distribution in most diffuse or predominantly involving mid lung zones diffuse or predominantly involving mid lung zones upper lobe involvement (atypical for IPF) upper lobe involvement (atypical for IPF) superimposed findings of subacute disease in some: ground-glass opacity or nodules superimposed findings of subacute disease in some: ground-glass opacity or nodules headcheese sign with findings of fibrosis headcheese sign with findings of fibrosis long term or repeated exposure long term or repeated exposure irregular fibrosis: coarse scars, septal thickening, traction bronchiectasis, honeycombing in some irregular fibrosis: coarse scars, septal thickening, traction bronchiectasis, honeycombing in some patchy, lacks a subpleural distribution in most patchy, lacks a subpleural distribution in most diffuse or predominantly involving mid lung zones diffuse or predominantly involving mid lung zones upper lobe involvement (atypical for IPF) upper lobe involvement (atypical for IPF) superimposed findings of subacute disease in some: ground-glass opacity or nodules superimposed findings of subacute disease in some: ground-glass opacity or nodules headcheese sign with findings of fibrosis headcheese sign with findings of fibrosis
 upper lobe involvement (atypical for IPF) superimposed findings of subacute disease in some: ground-glass opacity or nodules superimposed findings of subacute disease in some: ground-glass opacity or nodules headcheese sign with findings of fibrosis headcheese sign with findings of fibrosis long term or repeated exposure long term or repeated exposure irregular fibrosis: coarse scars, septal thickening, traction bronchiectasis, honeycombing in some irregular fibrosis: coarse scars, septal thickening, traction bronchiectasis, honeycombing in some patchy, lacks a subpleural distribution in most patchy, lacks a subpleural distribution in most diffuse or predominantly involving mid lung zones diffuse or predominantly involving mid lung zones upper lobe involvement (atypical for IPF) upper lobe involvement (atypical for IPF) superimposed findings of subacute disease in some: ground-glass opacity or nodules superimposed findings of subacute disease in some: ground-glass opacity or nodules headcheese sign with findings of fibrosis headcheese sign with findings of fibrosis")
91
Hypersensitivity Pneumonitis: progression 6 month follow-up.

92
. Chronic HP

93
.

100
chronic HP: reticulation and traction bronchiectasis.

101
chronic hypersensitivity pneumonitis.

102
subacute HP: ground-glass opacity chronic HP: reticulation and traction bronchiectasis.

103
HRCT of Common Lung Diseases W. Richard Webb

Similar presentations














>")









 r Thin elastin-rich connective component containing.>")





