Download presentation
Presentation is loading. Please wait.

1
Case presentation Samane Nabi Emergency medicine resident 93.5.14

2
(HAZRAT_E_RASUL HOSPITAL)
A 82 y old man with The chief complaint of WEAKNESS coming to ED (HAZRAT_E_RASUL HOSPITAL) At 22:45 Pm
 At. 22:45 Pm")
3
CC: Weakness PI: a 82 y old man was referred to ED With the chief complaint of generalized weakness which had been started 5 days before the entrance to ED. He complaint from intermittent burning retro sternal chest pain and epigastric pain that was radiated to the back with no relation to feeding It was accompanying with nausea, vomiting and cold sweating. content of vomiting was the eaten food and without blood and bile. He had no dyspnea. He had normal defication.no Melena. He had no fever. Patients with these symptom, was hospitalized for 2 days in another hospital before entrance to ED that due to the general deterioration, left center.

4
Dyspepsia or epigastric discomfort +
PMH: IHD + CCU addmition + HTN+ DM- Dyspepsia or epigastric discomfort +

5
Patient had not history of drug using.
DH & HH: Patient had not history of drug using. Alcohol – Smoking – Opium –

6
P/E: VS: PR: 97 BP: 100/60 RR:17 T: 35 Axillary O₂ sat: 90% BS: 250

7
Patient was conscious, ill and pail and he had cold sweating.
No JVD. Lung: normal Heart: s1 and s2 were detected with no pathologic sounds or murmur Abdomen: Guarding- , Distention-, Mild Epigastric Tenderness+ Extremities: Extremity pulses were symmetrically full.

8
What's your differential diagnosis?

9
Differential diagnosis
Example of a table Differential diagnosis 1. Acute coronary syndrome 2. Aortic dissection 3. Acute pancreatitis 4. Peptic ulcer perforation 5. Bowel perforation 6. GIB 7. Electrolyte disorder

10
ECG:

11
Patients with clinical suspicion of acute coronary syndrome, was treated.
com + pom Plavix ASA Enoxaparin Iv nitro Captopril Metoral O2 with mask Serial ECG Internist consultation

12
laboratory data: WBC: 13400 VBG: Neut: 90% PH: 7.43 HB: 16.2
HCT: 44 PLT: VBG: PH: 7.43 HCO3: 19.5 PCO2: 30.1 BE: -10

13
The patient was transferred to the resuscitation room
After 1 hour, the patient's clinical condition worsened. he opened the eyes with voice his blood pressure was non measurable. Only carotid pulse was palpable. The patient was transferred to the resuscitation room

14
Central vein line was inserted Foley catheter was inserted
CVP:2 Foley catheter was inserted Urine out put: 0

15
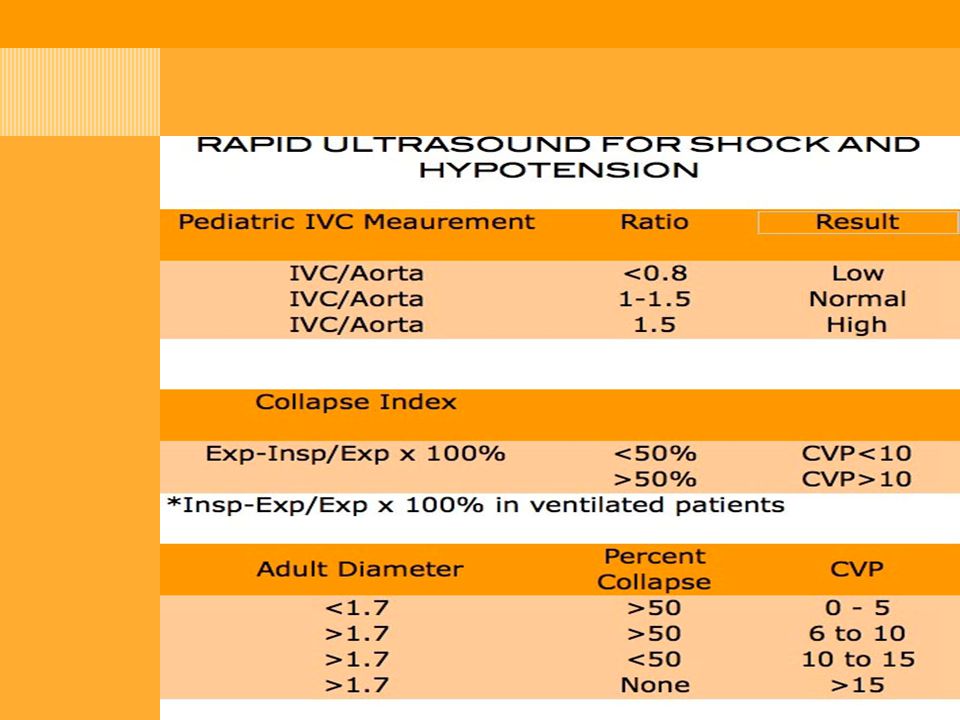
RUSH EXAM: IVC WAS Collapsed
No hypokinesia in heart, no tamponed no plural effusion In inter loop and Morison patch there was non homogenous fluid

16
In patient with septic shock
Vancomycin and meropenem was administered. After received of 2 liters normal slain CVP was 6 and urine out put was 200 cc BP: 100/60 PR: 90 Surgery consultation was done. CXR was taken.

18
Bs: 119 Na: 138 K: 3.5 BUN: 63 Cr: 3.5 CTNT : Negative PT: 14 PTT: 35 INR: 1

19
Surgery consultation:
Spiral CT scan of abdomen & pelvic with IV and oral contrast

22
D1 perforation with Purulent discharge
Patient in 7 am transferred to operation room with Peritonitis diagnosis due to hallo viscus perforation Operation report: D1 perforation with Purulent discharge Distal gastrectomy with wound closing and gasterogegenostomy

24
After this surgery he transferred to SICU and because of anastomose leak and bowel evisceration Twice again operated. Patient any time win and after 30 days hospitalization and five times CPR expired.

25
in ED, shock is rarely listed as a primary
diagnosis. Arterial hypotension, defined as a systolic blood pressure (BP) below 100 mm Hg, is measured at least one time in 19% of ED patients; however, diagnosed traumatic, cardiogenic, or septic shock is less common, constituting about 1 to 3% of all ED visits.
 below 100 mm Hg, is measured at least one time in 19% of ED patients; however, diagnosed traumatic, cardiogenic, or septic shock is less common, constituting about 1 to 3% of all ED visits.")
26
Patients in the ED are in shock with no obvious cause.
Rapid recognition of shock requires immediate history and physical examination In general, patients with shock are ill, asthenic, pale, often sweating, and usually tachypneic or grunting, and often have a weak and rapid pulse. HR can be normal or low in shock. BP initially can be normal because of adrenergic reflexes. a single systolic BP less than 100 mm Hg in the ED is associated with a threefold increase in in-hospital mortality and a tenfold increase in sudden death. Shock can be strongly supported by the presence of a worsening base deficit or lactic acidosis.

27
Urine output provides an excellent indicator of organ perfusion.
The HR/systolic BP ratio may provide a better marker of shock than either measurement alone, a normal ratio is less than 0.8. Urine output provides an excellent indicator of organ perfusion. normal out put: >1.0 mL/ kg/hr , reduced: mL/kg/hr, severely reduced: <0.5 mL/ kg/hr A lactate concentration greater than 4.0 mM or a base deficit more negative than −4 mEq/L predicts the presence of circulatory insufficiency.

28
Empirical Criteria for Diagnosis of Circulatory Shock

29
MANAGEMENT: Monitoring Perfusion Status Quantitative Resuscitation
all patients with shock, HR, BP, and oxyhemoglobin saturation are continuously monitored Quantitative Resuscitation pulmonary artery catheter Lactate clearance Mixed venous oxygen saturation (SvO2) Ventilation Rapid sequence intubation is the preferred method of airway control in most patients with refractory shock. Volume Replacement The goal in volume replacement is slightly elevated left ventricular end-diastolic volume, which is a difficult measurement to make in the ED. The CVP is most often used to estimate right ventricular filling pressure and is used in some quantitative resuscitation.
 Ventilation. Rapid sequence intubation is the preferred method of airway control in most patients with refractory shock. Volume Replacement. The goal in volume replacement is slightly elevated left ventricular end-diastolic volume, which is a difficult measurement to make in the ED. The CVP is most often used to estimate right ventricular filling pressure and is used in some quantitative resuscitation.")
30
Definitions and Criteria for Septic, Hemorrhagic, and Cardiogenic Shock

31
Septic shock: Treatment begins by establishing adequate ventilation to correct hypoxia and acidosis and to reduce systemic oxygen consumption and left ventricular work. This often requires endotracheal intubation and sedation for mechanical ventilation. Etomidate !!!! The second goal is to achieve adequate ventricular filling. Initial volume replacement should include rapid infusion of 20 to 25 mL of crystalloid per kilogram. If hypo perfusion is persistent, 5- to 10-mL/kg boluses of a natural colloid (such as albumin) should be considered. Blood should be transfused in the ED to restore hematocrit to 30%. The third directive is to eradicate the infection with antimicrobial therapy and, where necessary, surgical drainage.
 should be considered. Blood should be transfused in the ED to restore hematocrit to 30%. The third directive is to eradicate the infection with antimicrobial therapy and, where necessary, surgical drainage.")
32
Septic shock refractory to volume restoration (urine output or BP remains low, lactate increases) requires vasopressor support. norepinephrine ( μg/min) The use of corticosteroids in the treatment of sepsis and septic shock has been investigated with mixed results. Most current guidelines recommend that low-dose hydrocortisone be administered only to patients receiving chronic steroid replacement and in patients with refractory shock despite adequate fluid and vasopressor support

Similar presentations