Download presentation
Presentation is loading. Please wait.

1
Introduction in Prosthodontics (dental prosthetics)
Dr. Waseem Bahjat Mushtaha Specialized in prosthodontics

2
Introduction: Prosthesis: an artificial appliance which replace lost or congenitally missing tissue. Some prosthesis restore both function and appearance of tissue they replace other merely restore one of these factors.

3
Prosthetics: is the art and science of designing and fitting artificial substitutly to replace lost or missing tissue. Prosthodontics (dental prosthetics): Is the branch of dental art and science which with the replacement of missing teeth and oral tissue to restore and maintain oral form, function, appearance, phonetics and health.
: Is the branch of dental art and science which with the replacement of missing teeth and oral tissue to restore and maintain oral form, function, appearance, phonetics and health.")
5
Complete denture prosthodontics:
involves an artificial replacement of the lost natural dentition and associated structures of the maxilla and mandible for patient who has lost all their remaining natural teeth.

7
Function of complete denture:
1- Mastication: chew food for swallowing and digestion. 2- Speech (phonetics): the teeth either natural or artificial assist the tongue and lips to form some of the sounds of speech. 3- Appearance (aesthetic): is influence by the shape of jaws together with the position and occlusal relation ship of the teeth. 4- Health of the alveolar bone and the tempro mandibular joints (T.M.J).
: the teeth either natural or artificial assist the tongue and lips to form some of the sounds of speech. 3- Appearance (aesthetic): is influence by the shape of jaws together with the position and occlusal relation ship of the teeth. 4- Health of the alveolar bone and the tempro- mandibular joints (T.M.J).")
8
Complete dentures have three structures:
1- The fitting surface. 2- The occlusal surface. 3- The polished surface.

9
Anatomy and physiology in relation to complete denture
I- oral mucosa membrane (tissue compression) 1- The bone of the upper and lower edentulous jaws are covered with a soft tissues and the oral cavity is lined with soft tissue known as mucosa membrane. 2- This mucosa membrane is composed of two layer mucosa and sub mucosa. 3- Mucosa consists of stratified squamous epithelium.
 1- The bone of the upper and lower edentulous jaws are covered with a soft tissues and the oral cavity is lined with soft tissue known as mucosa membrane. 2- This mucosa membrane is composed of two layer mucosa and sub mucosa. 3- Mucosa consists of stratified squamous epithelium.")
10
4- The thickness and consistency of the sub mucosa are largely responsible for the support denture.
5- In the edentulous patient the crest of residual alveolar ridge + hard palate has masticatory mucosa have firmly attached to the supporting bone. 6- The sub mucosa in the region in the median palatine suture of the maxillary bone is extremely thin so will become inflamed when wearing denture.

11
II- the alveolar ridges
1) The residual ridge consists of: 1- Denture – bearing mucosa. 2- Sub mucosa 3- Periostem 4- Under laying residual alveolar bone.
 The residual ridge consists of: 1- Denture – bearing mucosa. 2- Sub mucosa. 3- Periostem. 4- Under laying residual alveolar bone.")
12
Types of alveolar ridges and palate formation:
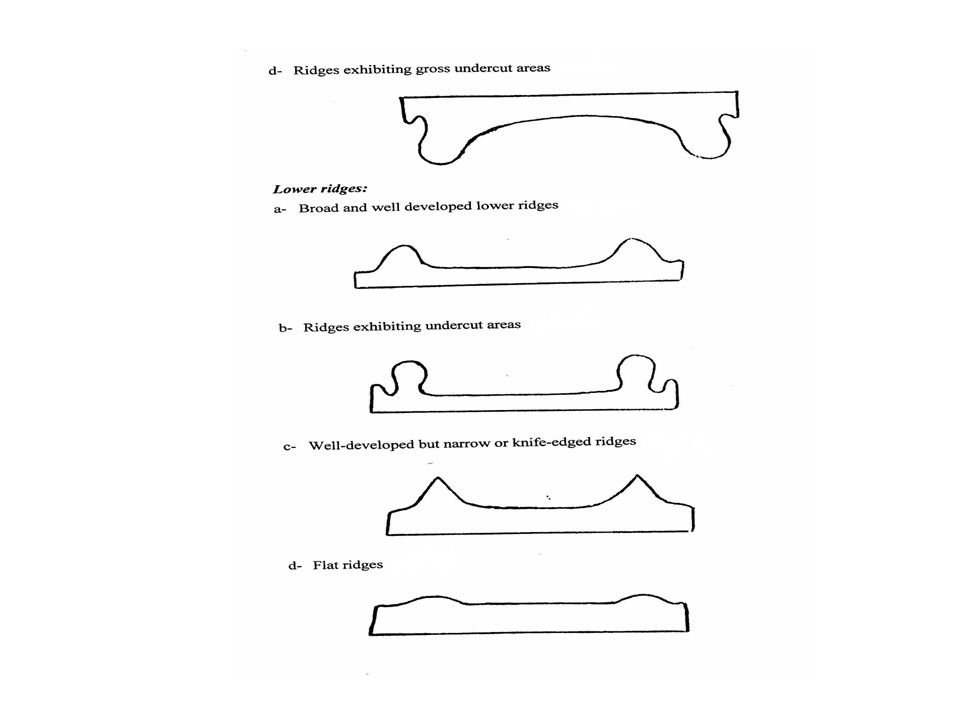
I- upper ridges 1- well – developed (upper ridge) but not abnormally thick ridges and palate with a moderate vault. 2- Flat –v- shaped palate usually associated with bulky ridge. 3- Flat palate with small ridge and shallow. 4- Ridge exhibiting gross under cut area.
 but not abnormally thick ridges and palate with a moderate vault. 2- Flat –v- shaped palate usually associated with bulky ridge. 3- Flat palate with small ridge and shallow. 4- Ridge exhibiting gross under cut area.")
14
II- lower ridge 1- Broad and well developed lower ridges.
2- Ridges exhibiting under cut areas. 3- Well developed but narrow or knife edged ridges. 4- Flat ridge.

16
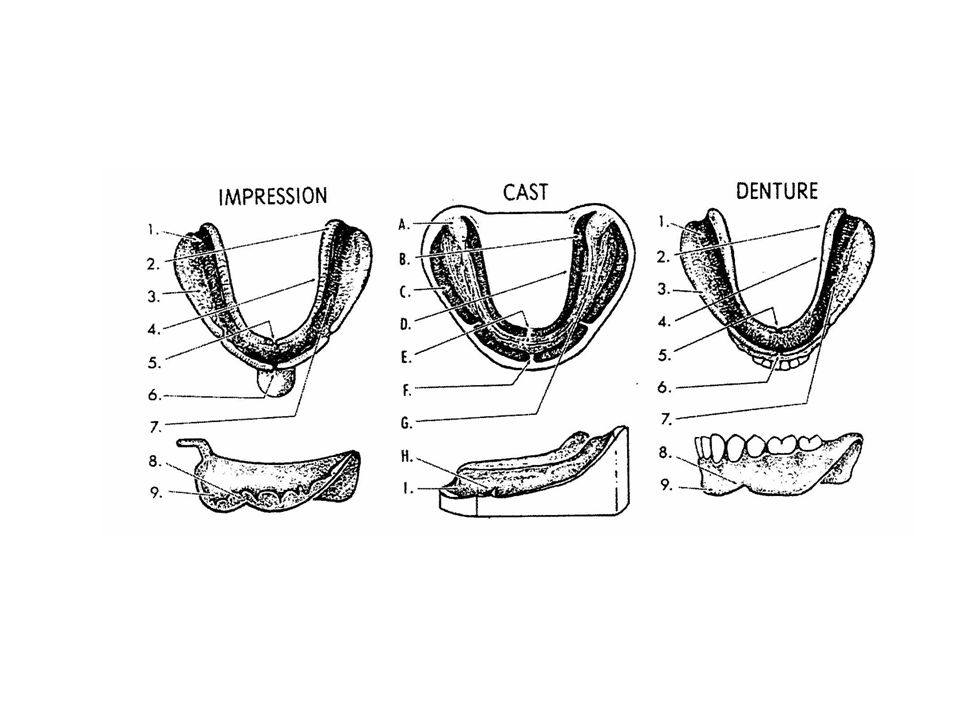
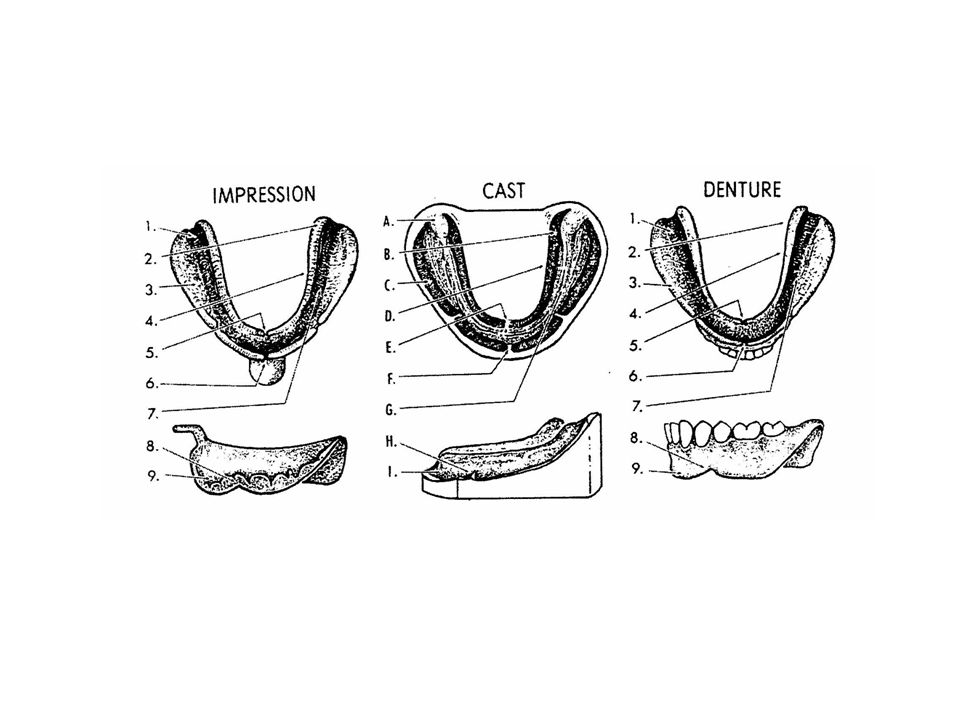
Anatomical land marks of complete dentures
I- INTRA ORAL ANATOMICAL LAND MARK II- EXTRA ORAL LANDMARK

17
Upper denture

18
I- INTRA ORAL ANATOMICAL LAND MARK
1- Stress bearing (supporting area). 2- Peripheral or limiting (sealing) areas
. 2- Peripheral or limiting (sealing) areas.")
19
Incisive papilla

20
I- supporting structure
1- Incisive papilla: 1) It is the elevation of the tissue that covers the incisive foramens (the opening of the nasopalatine canal which, carry the nasopalatine vessels and nerves). 2) Location, on the median line behind and between the central incisors. 3) In old edentulous mouth it is located on the center of the ridge due to resorption. 4) It may require relief in the finished denture base to prevent irritation of the nasopalatine nerve.
 It is the elevation of the tissue that covers the incisive foramens (the opening of the nasopalatine canal which, carry the nasopalatine vessels and nerves). 2) Location, on the median line behind and between the central incisors. 3) In old edentulous mouth it is located on the center of the ridge due to resorption. 4) It may require relief in the finished denture base to prevent irritation of the nasopalatine nerve.")
21
2- Rugae area

22
2- Rugae area: 1) The rugae are irregular shaped rolls of soft tissue.
2) Location, lie in the anterior part of the hard palate. 3) It is considered a secondary stress- bearing area for the upper complete denture. 4) With the natural dentitions, it assists in formation of sounds like the letter s.
 Location, lie in the anterior part of the hard palate. 3) It is considered a secondary stress- bearing area for the upper complete denture. 4) With the natural dentitions, it assists in formation of sounds like the letter s.")
23
Residual alveolar ridge

24
3- Residual alveolar ridge
1) The residual alveolar ridge and most of the hard palate are considered the major or primary stress bearing area in the upper jaw. 2) The crest of the residual ridge is covered with layer of fibrous connective tissue which is most favorable for supporting the denture because of it is firmness and position. 3) The crest of ridge is described as a primary stress-bearing area and most tolerated to resisting the denture movement and resulting irritation
 The residual alveolar ridge and most of the hard palate are considered the major or primary stress bearing area in the upper jaw. 2) The crest of the residual ridge is covered with layer of fibrous connective tissue which is most favorable for supporting the denture because of it is firmness and position. 3) The crest of ridge is described as a primary stress-bearing area and most tolerated to resisting the denture movement and resulting irritation.")
25
Median palatine raphe

26
4- Median palatine raphe:
1) It is median suture formed by the union of the palatine processes of maxilla and horizontal plates of the palatine bones. 2) It is covered with mucosa membrane and little sub mucosa tissue. 3) This area may require selective relief with in denture base.
 It is median suture formed by the union of the palatine processes of maxilla and horizontal plates of the palatine bones. 2) It is covered with mucosa membrane and little sub mucosa tissue. 3) This area may require selective relief with in denture base.")
27
5- The tuberosities

28
5- The tuberosities 1) The posterior part of the maxillary alveolar ridge forms prominence called the tuberosity. 2) It is usually a bulbous extension of the residual ridge in the second and third molar region. 3) Terminating hamular notch.
 It is usually a bulbous extension of the residual ridge in the second and third molar region. 3) Terminating hamular notch.")
29
4) Large tuberosities bounded by deep salci offer very satisfactory denture
5) Tuberosities exhibiting gross undercuts may require surgical treatment. 6) They are identified in the finished denture by the tubercular fossa.
 Tuberosities exhibiting gross undercuts may require surgical treatment. 6) They are identified in the finished denture by the tubercular fossa.")
30
6- Fovea palatinae

31
6- Fovea palatinae: 1) These are indentations near the midline of the palate formed. 2) They are close to the vibrating line and always in soft tissue. 3) Which makes an ideal guide for the ending of the posterior border of the denture
 They are close to the vibrating line and always in soft tissue. 3) Which makes an ideal guide for the ending of the posterior border of the denture.")
32
7- Tours palatinus

33
7- Tours palatinus: 1) At the junction of the palatine process of the maxillary bone, in the midline or on each side lateral to the midline. 2) A bony projection is some times observed. 3) It varies in size and form. 4) If it is too large it should be surgically removed. 5) If it is small the denture base should be relieved of that area.
 At the junction of the palatine process of the maxillary bone, in the midline or on each side lateral to the midline. 2) A bony projection is some times observed. 3) It varies in size and form. 4) If it is too large it should be surgically removed. 5) If it is small the denture base should be relieved of that area.")
34
Border structures that limit the periphery of the upper denture (limiting structure)
1- The maxillary labial frenum: 1) It is a fibrous bond covered by mucosa membrane that extends from the labial aspect of the residual alveolar ridge to the lip. 2) It has no muscle fiber and has no action of it is own. 3) The labial in the labial flange of the denture must be just wide and deep enough to allow the frenum to pass through it without manipulation of the lip.
 It is a fibrous bond covered by mucosa membrane that extends from the labial aspect of the residual alveolar ridge to the lip. 2) It has no muscle fiber and has no action of it is own. 3) The labial in the labial flange of the denture must be just wide and deep enough to allow the frenum to pass through it without manipulation of the lip.")
35
The maxillary labial frenum

36
2- Labial vestibule and labial flange:
1) The labial flange of maxillary denture occupies a potential space bounded by: labial aspect of the residual alveolar ridge, the muco-labial alveolar fold, and the orbicularis oris muscle. 2) The length of this flange should not extend beyond the normal drape of the muco-labial fold. 3) The thickness of the flange depends up on the degree of alveolar resorption. 4) The denture border area between the labial frenum and the buccal frenum is known as the maxillary labial flange.
 The labial flange of maxillary denture occupies a potential space bounded by: labial aspect of the residual alveolar ridge, the muco-labial alveolar fold, and the orbicularis oris muscle. 2) The length of this flange should not extend beyond the normal drape of the muco-labial fold. 3) The thickness of the flange depends up on the degree of alveolar resorption. 4) The denture border area between the labial frenum and the buccal frenum is known as the maxillary labial flange.")
37
2- Labial vestibule and labial flange

38
3- Buccal frenum: 1) It is a some times a single fold of mucosa membrane, sometimes double and in some mouths, broad and fan shaped. 2) The buccal notch in the denture must be broad enough to allow the movement of the buccal frenum. 3) Inadequate provision for the buccal frenum or excess thickness of the flange distal to the buccal notch can cause dislodgment of the denture when the cheeks are moved posterioly as in abroad smile.
 It is a some times a single fold of mucosa membrane, sometimes double and in some mouths, broad and fan shaped. 2) The buccal notch in the denture must be broad enough to allow the movement of the buccal frenum. 3) Inadequate provision for the buccal frenum or excess thickness of the flange distal to the buccal notch can cause dislodgment of the denture when the cheeks are moved posterioly as in abroad smile.")
39
Buccal frenum

40
4- Buccal vestibule: 1) It is extended from the buccal frenum to the hamular notch. 2) It houses the buccal flange of the denture. 3) This space between the ridge and cheek. 4) The buccal flange of maxillary denture should fill but not over fill it. 5) The thickness of the distal end of the buccal flange of the denture must be adjusted to accommodate the ramus and cronoid process and masseter muscle as they function. The distal end of the buccal flange must not be too thick because the ramus will push the denture out of the place during opening or lateral movement of mandible.
 This space between the ridge and cheek. 4) The buccal flange of maxillary denture should fill but not over fill it. 5) The thickness of the distal end of the buccal flange of the denture must be adjusted to accommodate the ramus and cronoid process and masseter muscle as they function. The distal end of the buccal flange must not be too thick because the ramus will push the denture out of the place during opening or lateral movement of mandible.")
41
Buccal vestibule

42
5- Pterygomaxillary (hamular) notch
1) It is formed by the pterygoid process of sphenoid bone and the posterior end of maxilla, back to the tuberosity. 2) It is used as boundary of the posterior border of maxillary denture. 3) It is important for sealing.
 It is formed by the pterygoid process of sphenoid bone and the posterior end of maxilla, back to the tuberosity. 2) It is used as boundary of the posterior border of maxillary denture. 3) It is important for sealing.")
43
Pterygomaxillary (hamular) notch
 notch")
44
6- Vibrating line of the palate
1) It is an imaginary line drawn across the posterior part of the palate that marks the beginning of motion in the soft palate when the patients say "ah". 2) It extends from one pterygomaxillary notch to other. 3) It is not the junction between hard and soft palate. It is always in soft palate.
 It is an imaginary line drawn across the posterior part of the palate that marks the beginning of motion in the soft palate when the patients say ah . 2) It extends from one pterygomaxillary notch to other. 3) It is not the junction between hard and soft palate. It is always in soft palate.")
45
Vibrating line of the palate

46
7- Posterior palatal border (Potsdam)
1) The distal edge of the maxillary denture base terminates in the posterior palatal seal area. 2) This denture edge generally ends at or before the vibrating line. 3) The seal of this border must be situated in the region of compressible tissue just distal to the hard palate. (But it must be anterior to the vibrating line).
 The distal edge of the maxillary denture base terminates in the posterior palatal seal area. 2) This denture edge generally ends at or before the vibrating line. 3) The seal of this border must be situated in the region of compressible tissue just distal to the hard palate. (But it must be anterior to the vibrating line).")
47
Posterior palatal border (Potsdam)
")
48
8- The soft palate Patient may be broadly divided in to classes with regard to non mobile area: 1) Those whose palates exhibit movement at the junction of the hard palate and soft palate. 2) Those whose soft palates move some distance behind the junction.
 Those whose palates exhibit movement at the junction of the hard palate and soft palate. 2) Those whose soft palates move some distance behind the junction.")
49
The width of the area available for the posterior palatal seal will depend up on the curvature of the soft palate. There are three classes of curvature of soft palate: Glass I: the soft palate has a gentle curvature and allows for abroad posterior palatal seal area. Glass II: the soft palate has a medium curvature and allow for a medium width of the posterior palatal seal area. Glass III: the soft palate has a sharp and abrupt curvature and allows for a narrow posterior palatal seal area.

50
The soft palate

52
II- lower denture Intra oral structures that support the lower denture (supporting structure): 1) Residual alveolar ridge: The crest of the residual alveolar ridge is covered by fibrous connective tissue, but in many mouths the under lying bone is and without a good bony plate covering it.

54
2) External oblique ridge
1- It is a bony ridge. 2- It begins at the junction of alveolar ridge and the ramus of the mandible. 3- It descends obliquely downward and forward across the outer surface of the body. 4- It fades out at appoint nearly opposite the mesial surface of the first molar. 5- It is recorded in the impression and wed as appoint reference in the impression making.

56
3) The buccal shelf of bone
1- Location: it is the area between the mandibular buccal frenum and the anterior edge of masseter 2- This area is bonded: - Medially: the crest of residual ridge. - Anteriorly: buccal frenum. - Laterally: external oblique ridge. - Distally: retromolar pad. 3- The buccal shelf offers excellent resistance to forces (primary stress bearing area of the mandibular denture) due to: - It is at right angles to the vertical occlusal forces. - Very wide. - It is covered with good smooth cortical bone.
 due to: - It is at right angles to the vertical occlusal forces. - Very wide. - It is covered with good smooth cortical bone.")
58
4) Retromolar region and pad:
1- It is a triangular soft pad of tissue at the distal end of the lower ridge. 2- It must be covered by denture base. 3- Sealing the retromolar pad aids in the stability of the denture. 5) Mylohyoid ridge (internal oblique ridge): 1- It descends obliquely down and across the inner surface of the body of the mandible. 2- It begins in the region of the third molar and continuous downwards and forwards to the lower border of the mandible near the midline.
 Mylohyoid ridge (internal oblique ridge): 1- It descends obliquely down and across the inner surface of the body of the mandible. 2- It begins in the region of the third molar and continuous downwards and forwards to the lower border of the mandible near the midline.")
60
6) Mental foramen 1- location: on the buccal surface of the mandible in the premolar region. 2- Mental nerves and vessels pass thought it. 3- In cases of extreme ridge resorption it is usually located on the crest of the ridge. 4- Pressure from the denture may cause pain and numbness (require relief in finished denture)
")
61
7) Torus mandibularis 1- It is bony projection.
2- Sometimes found on the lingual surface in the premolar region. 3- If it is too large it will require surgical removal. 4- If small, the denture should be relived in that area.

62
Border structures that limit the periphery of the lower denture (limiting structures)
1) The mandibular labial frenum: 1- It is a band of fibrous connective tissue that helps to attach the orbicularis oris (muscle of the lip) 2- It is accommodated by a groove in the mandibular denture.
 The mandibular labial frenum: 1- It is a band of fibrous connective tissue that helps to attach the orbicularis oris (muscle of the lip) 2- It is accommodated by a groove in the mandibular denture.")
64
2) The mandibular vestibule and labial flange:
The part of the denture that extends between the labial notch and the buccal notch is called the mandibular labial flange. 3) Buccal frenum: 1- This attachment connects with continuous band through the corner of the mouth And on up to the buccal frenum of the maxilla.
 Buccal frenum: 1- This attachment connects with continuous band through the corner of the mouth And on up to the buccal frenum of the maxilla.")
66
4) Buccal vestibule and buccal flange:
1- It extends from the buccal frenum posteriorly to the out side back corner of the retromolar pad and from the crest of the residual alveolar ridge to the cheek. 2- It houses the buccal flange of the mandibular denture. 5) Masseter muscle influence area: 1- The distobuccal corner of the mandibular denture must coverage rapidly to avoid displacement due to contracting pressure of the masseter muscle. (Whose anterior fibers pass out side buccinator in this region)
 Masseter muscle influence area: 1- The distobuccal corner of the mandibular denture must coverage rapidly to avoid displacement due to contracting pressure of the masseter muscle. (Whose anterior fibers pass out side buccinator in this region)")
68
6) Lingual flange area (alveolingual sulcus):
The distal extention of the lingual flange lies in the lingual pouch. Lingual pouch (retromylohoid fossa): Is the area bounded medially by the tongue, laterally by the mandible, posteriorlly by the palatoglussus arch, which is formed in part by the palatoglossus muscle and in part by the lingual extention of the superior constructor muscle and anteriorly by the posterior 3 mm of the mylohoid muscle. Forward on the lingual extension, the area is influence by the mylohoid muscle, which attaches to the mylohoid ridge. The flange extends below and medially from the mylohoid ridge to fill the fold formed by the tongue and the tissue of the floor of the mouth. This means that the inner surface of this flange does not rest on mucosa membrane over bone, but on soft tissue. It leaves the bony attachment at the mylohoid ridge, and the flange extends out under the tongue to fill the fold. The forward part of the flange area of this region over the sublingual stand usually is shallow because of the movement of the tissue that is controlled indirectly by the mylohoid muscle.
: Is the area bounded medially by the tongue, laterally by the mandible, posteriorlly by the palatoglussus arch, which is formed in part by the palatoglossus muscle and in part by the lingual extention of the superior constructor muscle and anteriorly by the posterior 3 mm of the mylohoid muscle. Forward on the lingual extension, the area is influence by the mylohoid muscle, which attaches to the mylohoid ridge. The flange extends below and medially from the mylohoid ridge to fill the fold formed by the tongue and the tissue of the floor of the mouth. This means that the inner surface of this flange does not rest on mucosa membrane over bone, but on soft tissue. It leaves the bony attachment at the mylohoid ridge, and the flange extends out under the tongue to fill the fold. The forward part of the flange area of this region over the sublingual stand usually is shallow because of the movement of the tissue that is controlled indirectly by the mylohoid muscle.")
70
7) Lingual frenum 1- It is anterior attachment of the tongue.
2- Very resistant and active and often wide. 3- It needs complete functional trimming to avoid having the attachment displace the lower denture.

75
II- EXTRA ORAL LANDMARK

76
II- EXTRA ORAL LANDMARK
1) Inter papillary line This is an imaginary line running between the two pupils of the pupils of the eye when the patient is looking straight forward. 2) ala-tragus line This is an imaginary line running from the inferior border of the ala of the nose to the superior border of the tragus of the ear (camper's line). (Establishing the posterior occlusal plane of the artificial teeth).
 Inter papillary line. This is an imaginary line running between the two pupils of the pupils of the eye when the patient is looking straight forward. 2) ala-tragus line. This is an imaginary line running from the inferior border of the ala of the nose to the superior border of the tragus of the ear (camper s line). (Establishing the posterior occlusal plane of the artificial teeth).")
77
3) Canthus tragus line This is an imaginary line running from the outer canthus of the eye to the superior border of the ear. (Aid in locating the position of the condyles). 4) naso-labial sulcus 1- This is a depression that extends downward and laterally to the corner of the mouth. 2- It becomes deeper and more prominent with aging and due to loss of teeth. 3- It should be restored to normal contour by proper positioning of the anterior teeth and proper contouring of the upper labial flange.
. 4) naso-labial sulcus. 1- This is a depression that extends downward and laterally to the corner of the mouth. 2- It becomes deeper and more prominent with aging and due to loss of teeth. 3- It should be restored to normal contour by proper positioning of the anterior teeth and proper contouring of the upper labial flange.")
79
5) Vermilion border 1- It is the transitional epithelium between the mucosa membrane of the lip and skin. 2- The amount of the vermilion border showing depends on: 1. Bulk of orbicularis oris muscle. 2- The amount of labial alveolar bone. 3- Alignment of teeth. 3- Following the loss of teeth and resorption of bone There is a reduction in the amount of vermilion border showing. It should be restored with dentures.

81
6) Philtrum: 1- It is a diamond shaped area between the base of the nose and center of the upper lip. 2- It becomes distorted with the loss of teeth and becomes flat, it should be restore by normal shape with denture 7) Modiolus: 1- This is located at the confluence (meeting place) of the buccinator and other facial muscles. 2- The arch form of maxillary teeth support it 3- With the loss of teeth it droops giving the characteristic look of the edentulous person (sunken cheek)
 Modiolus: 1- This is located at the confluence (meeting place) of the buccinator and other facial muscles. 2- The arch form of maxillary teeth support it. 3- With the loss of teeth it droops giving the characteristic look of the edentulous person (sunken cheek)")
83
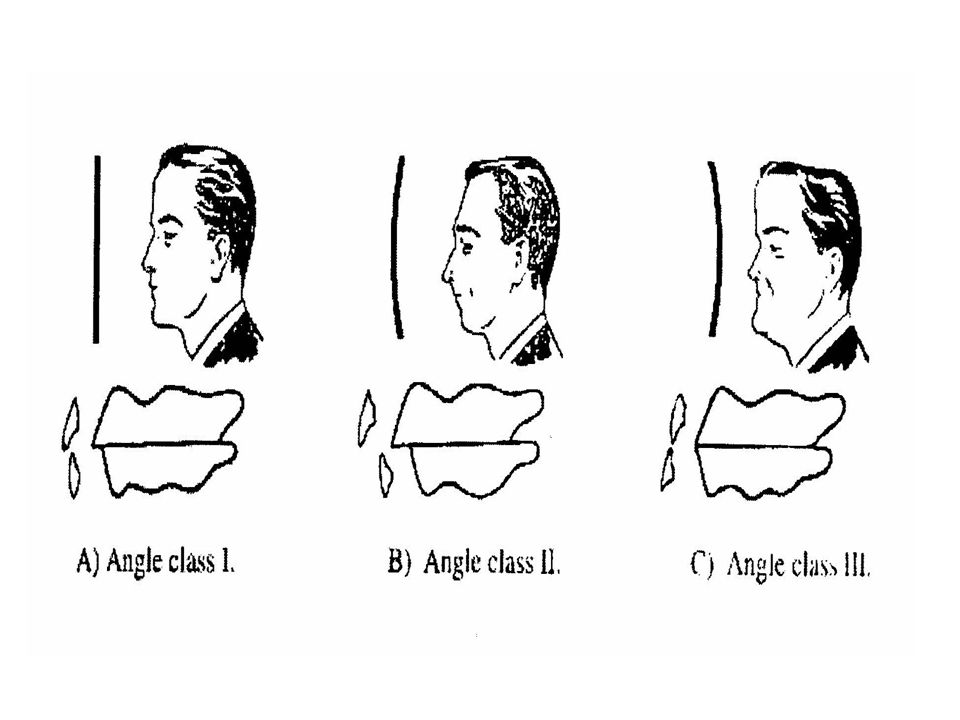
8) Mento labial sulcus 1- It runs from side to side horizontally between lower lip and chin 2- Its curvature indicates the maxillo-mandibular relation.

84
a- Angle class I: the curvature is gentle with an obtus angle (normal anterioposterior relation)
b- Angle class II: this represents a retruded mandibular position The mento-labial sulcus present an acute angle when the lower lip is folded toward the chin C-angle III: this is a protruded maxillo mandibular relation when the mento labial sulcus may an angle of almost 180º

86
ما أطيبك حيا وميتا يا رسول الله

Similar presentations






























. All rights reserved. No part of this product may be reproduced or transmitted.>")





